


Yo Kaku1, Atsushi Otsuka1*, Hideaki Tanizaki1, Rintaro Shibuya1, Yuichiro Endo1, Yumi Nonomura1, Masahiro Hirata2, Masakazu Fujimoto2, Katsuyuki Ohmori3, Takaki Sakurai2 and Kenji Kabashima1*
Departments of 1Dermatology, 2Diagnostic Pathology, and 3Laboratory Medicine, Kyoto University Graduate School of Medicine, 54 Shogoin-Kawara, Sakyo, Kyoto 606-8507, Japan. *E-mail: otsukamn@kuhp.kyoto-u.ac.jp; kaba@kuhp.kyoto-u.ac.jp
Accepted Dec 2, 2015; Epub ahead of print Dec 3, 2015
Ichthyosiform mycosis fungoides (MF) is a rare variant of MF, occurring in 3.5% of MF patients according to one study (1, 2). Patients with ichthyosiform MF exhibit clinical manifestations similar to those of acquired ichthyosis; histologically, however, they show epidermotropism of atypical lymphocytes. Ichthyosiform MF is characterized by indolent course and usually good response to phototherapy. Even among patients with conventional MF, dual CD4/CD8-positive MF is extremely rare, in contrast to a relatively high incidence of a mixture of CD4-positive neoplastic cells and inflammatory CD8-positive infiltrating lymphocytes. We report here a case of ichthyosiform MF with aggressive extracutaneous involvement, including cardiac involvement, with a dual CD4/CD8-positive immunophenotype.
CASE REPORT
A 43-year-old Japanese man was referred to our department with a 2-year history of extensive ichthyosis of the trunk and the extremities (Fig. 1A, B). He had a history of malaise and night sweats for 3 months, and abnormal cardiological findings and uveitis were found at the referring hospital. Physical examination revealed extensive ichthyosis of the trunk and the extremities without patches, plaques and tumours or diffuse erythrodermic change. Skin biopsy revealed a dense band-like infiltration of lymphocytes just beneath the epidermis with significant epidermotropism of small to medium-sized lymphocytes with irregular hyperchromatic nuclei with Pautrier’s microabscess (Fig. 1C, D). Focal, slight acanthosis with thin, compact orthokeratosis or parakeratosis was present (Fig. 1C, D).
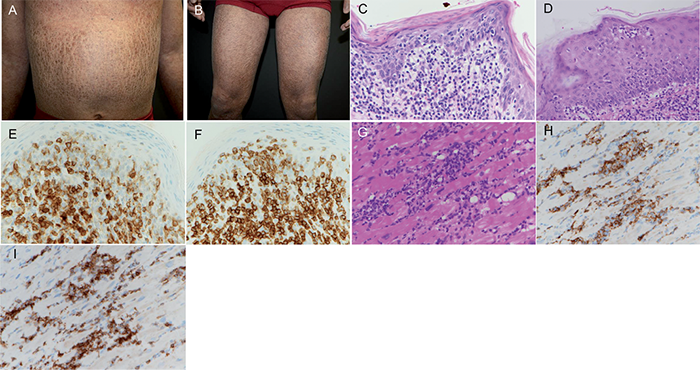
Fig. 1. Clinical and histopathological pictures of skin and heart biopsy. (A, B) Generalized ichthyosis of the trunk and extremities. (C) Histopathological examination of the skin revealed significant epidermotropism of atypical lymphocytes (haematoxylin and eosin (HE) ×400). (D) Pautrier’s microabscess was present (HE ×400). Epidermotropic lymphocytes were immunoreactive for both CD4 (E) and CD8 (F) (×400). (G) Percutaneous intravenous endomyocardial biopsy of interventricular septum revealed atypical lymphocytic infiltration into muscle bundles (HE ×400). The lymphocytes were immunoreactive for both CD4 (H) and CD8 (I) (×400).
Contrast-enhanced computed tomography (CT) and 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) showed bilateral inguinal and axillary lymphadenopathy and mild splenomegaly. Biopsy of an axillary lymph node revealed marked expansion of the subcapsular paracortical area with diffuse infiltration of small to medium-sized atypical lymphocytes. Complete blood count revealed leukocytosis (12.4 × 109/l leukocytes; normal 3.2–9.6 × 109/l) with 16.0% of morphologically abnormal lymphocytes. Other blood chemistry values were normal, except for the following elevated values: lactate dehydrogenase (317 IU/l; normal 124–226 IU/l), soluble interleukin-2 receptor (3,240 U/ml; normal 145–519 U/ml), angiotensin-converting enzyme (26.0 IU/l; normal 8.3–21.4 IU/l), immunoglobulin G (2,052 mg/dl; normal 826–1,840 mg/dl) and uric acid (9.6 mg/dl; normal 3.8–7.0 mg/dl). Human T-cell lymphotropic virus type 1 (HTLV-1) serology was negative. Bone marrow aspiration revealed normocellular marrow. Holter electrocardiogram (ECG) showed 73-beat sustained ventricular tachycardia (VT). Contrast-enhanced CT and FDG-PET did not show any nodular lesions or abnormal uptake in cardiac muscles. Percutaneous intravenous endomyocardial biopsy of the interventricular septum revealed atypical lymphocytic infiltration into the muscle bundles (Fig. 1G). Immunohistochemical staining of atypical lymphocytes showed CD3+, CD20–, CD4+ and CD8+ in the skin, lymph nodes and heart (Fig. 1E, F, H, I). PCR analysis for T-cell receptor (TCR) gene rearrangement indicated T-cell monoclonality in the cutaneous lesion, but not in the lymph node or cardiac muscle. Flow cytometry (FCM) analysis revealed a population of dual CD4+/CD8+ immunophenotype: 28.3% in the skin, 32.8% in the lymph node, and 24.7% in the blood (Fig. S11). The dual CD4+/CD8+ immunophenotype shows a large sized population in forward scatter in FCM. These cells were also positive for CD2, CD3, CD5, CD7, HLA-DR and TCR alpha-beta.
The patient was diagnosed with dual CD4/CD8-positive ichthyosiform MF with lymph node, peripheral blood and cardiac involvement (T2N3M1B1 stage IVB). Gemcitabine therapy was administered by our hospital’s haematological unit and resulted in an improvement in ichthyosis. Morphologically abnormal cells were no longer detected in peripheral blood. After the treatment with fluorometholone eye drops and chemotherapy, the uveitis disappeared immediately. Although VT responded very well to the amiodarone treatment, cardiac dysfunction did not improve after the chemotherapy. The patient was subsequently treated with allogenic umbilical cord blood transplantation. The patient remains under careful observation.
DISCUSSION
To the best of our knowledge, this is the second reported case of dual CD4/CD8-positive ichthyosiform MF. The immunophenotype of ichthyosiform MF is usually a T helper phenotype (CD4+ and CD8–), as in conventional MF. Most previously reported ichthyosiform MF cases have shown a favourable indolent course, whereas aggressive clinical course and poor prognosis have rarely been reported. In contrast, the one reported case of Stage IIA dual CD4/CD8-positive ichthyosiform MF showed limited response to psoralen plus ultraviolet A (PUVA) therapy and oral corticosteroid treatment: after discontinuation of this therapy, the infiltration of atypical lymphocytes in the epidermis became more severe (3). This was only one case, and further studies are needed, but dual CD4/CD8-positive ichthyosiform MF might be associated with poor prognosis compared with CD4-positive CD8-negative ichthyosiform MF.
Cardiac involvement has not previously been reported in ichthyosiform MF. In patients with conventional MF, it is rarely seen and the previous data on cardiac involvement have been obtained predominantly through autopsy. The rates of cardiac involvement were reported as 33% and 38% in 2 autopsy series (4, 5). When cardiac symptoms are present in an MF patient, cardiac infiltration of neoplastic cells should be considered as a possible cause of cardiac manifestation, even if no detectable mass lesion is present. It is unknown whether the uveitis is a manifestation of ichthyosiform MF or an incidental occurrence.
In summary, we report here a case of ichthyosiform MF with aggressive extracutaneous involvement including the lymph nodes, peripheral blood and heart. Further studies are necessary to identify whether dual CD4/CD8-positive ichthyosiform MF is associated with a more aggressive outcome than the usual merely CD4+ (or less frequently CD8+) phenotype.
The authors declare no conflicts of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2305
REFERENCES


