


Peter K. C. Goon1, David C. Greenberg2, Laszlo Igali3 and Nick J. Levell1
Departments of 1Dermatology and 3Pathology, Norfolk and Norwich University Hospital, Colney Lane, Norwich, NR4 7UY, and 2National Cancer Registration Service, Public Health England, Unit C, Magog, Cambridge, United Kingdom. E-mail: peter.goon@nhs.net
Accepted Dec 2, 2015; Epub ahead of print Dec 3, 2015
Epidemiological data on a very common skin cancer, squamous cell carcinoma (SCC), are lacking in the UK. Rates of SCC of the skin worldwide appear to be increasing (1–3) but accurate data in many countries are lacking due to incomplete cancer registration. The problems encountered include multiple cancer diagnoses, duplicate reports, reporting delays, misclassification of race/ethnicity, and pitfalls in estimations of cancer incidence rates (4). Common practices in the UK include only registering the first case of non-melanoma skin cancer (NMSC) in an individual patient, with non-inclusion of subsequent tumours and non-differentiation of multiple tumours. Cancer registry data from all home countries in the UK for 2011 showed there were 102,628 cases of NMSC registered: 57,800 (56%) in men and 44,828 (44%) in women, giving a male:female ratio of around 1.3:1. The majority of NMSCs are either basal cell carcinomas (BCCs) or SCCs. We have shown previously (5) that BCC cancer registry data represent a 2.0–2.2 fold underestimate of real incidence rates in the UK, due to the registration practices mentioned.
The aim of this work was to estimate the number of SCCs of the skin requiring surgical treatment in this region, and in the UK each year, and to compare these data with those collected by our cancer registries.
Methods
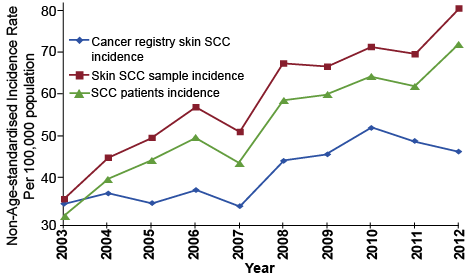
Data from the Eastern Office, National Cancer Registration Service, Public Health England, was obtained from 2003 to 2012. These were compared with the incidence of SCCs of skin recorded from East Norfolk and Waveney (ENW): (Breckland, Broadland, Great Yarmouth, North Norfolk, Norwich, South Norfolk and Waveney community districts) in the Eastern Region of the UK, from 2003 to 2012. These areas represent the catchment area of the histopathology service at the Norfolk and Norwich University Hospital (NNUH). Skin SCC histology results from each hospital in the region are coded and recorded monthly by the International Classification of Diseases categories ICD10/ICDO-2.
We confirm that there have been no changes in catchment area for the pathology laboratory or change of practice protocols for the pathologists involved for the period of study. We can also confirm that there have been no changes in physician patterns of referral of lesions over the study period. There were also no incentives for primary care physicians to remove skin lesions. Pathological diagnostic criteria and routines have not changed during the period of study.
Vallejo-Torres et al. (6) have estimated the costs of diagnosing and treating NMSC in the UK. We have used their calculations for “bottom-up” and “top-down” estimates to calculate the estimated costings in pounds sterling (analyses and definitions of these terms clarified in their paper and beyond the scope of this one). Their estimate per case of NMSC was a mean cost of £889 (bottom-up analyses) and £1,226 (top-down analyses), respectively, in 2008 to the NHS in England.
Results
Over the 10-year study-period stated above, the population of ENW increased by approximately 10.4%. The number of skin SCC samples increased 2.8 fold (by 182.8%), while patient numbers with SCC also increased 2.8 fold (by 185.9%). Table SI1 and Fig. 1 show a significantly lower recording of SCC by the registry compared with histology records. Further, the data show that registry data recorded a decrease in skin SCC whereas the histology and patient data record a large increase between 2003 and 2012. A similar fall in recording of BCC data has been described (5).
The UK population was estimated to be 63.7 million in 2012 (7). The ENW population was estimated to be 865,300 which represented 1.35% of the national population. When our data are extrapolated nationally, this then represents an estimate of 51,555 cases of skin SCC samples from 46,074 patients. The estimate of skin SCC for the whole of the UK in 2012 would be approximately 23,604 cases based on UK national cancer registry data (assuming that skin SCC represent 23% of the total NMSC).
A potential confounder is that ENW has a higher population of elderly people (defined here as 65 years and over) = 22.5%. The national figure is 16.9% of the total population. This represents an 11.1% increase from the national mean (7). Another important confounding factor is the amount of sunshine available across the UK. The UK national mean is 1,493 h/year. In Eastern England, the mean has been calculated at 1,570 h/year. This represents a 5.2% increase from the national mean (8). Finally, another important confounder is the percentage of Caucasian (white) people in the population. ENW has a high percentage of White British, White Irish, White gypsy/traveller and White Other (96.4%) compared to the national mean of 85.4% (Data from the Office of National Statistics, Census 2011). This represents an increase of 12.9% from the national mean (9).
When these factors are given equal weighting, our data represent a cumulative increase of 27.4% from the national means, therefore an approximation to the mean would therefore be an estimated 37,428 cases of skin SCC for the UK in 2012. This figure represents a 58.6% increase over the estimated figure from national cancer registry data (23,604). We suggest that this figure reflects more accurately the true UK incidence for SCC skin in view of the previously noted inefficiencies in the data recording in the cancer registries.
When we use these techniques for estimating the total UK incidence for SCC skin in 2011, we derive a figure of 31,876. This will place SCC of skin in the top 5 most common cancers (potentially lethal) in the UK (after Bowel, prostate, lung and breast cancer) (Fig. S11) (10).
Discussion
NMSC incidence figures from UK national cancer registries have been acknowledged to be far from comprehensive. Recording NMSC has not been a priority within registries probably because of the common perception that NMSC are non-lethal so data are incomplete. Most registries here in the UK record only the first NMSC of each histological type (e.g. BCC or SCC) per individual, and it is thought that much information on small NMSCs treated in primary care and the private sector does not reach the registries because they are commonly treated in the community by topical means such as creams or cryotherapy, and not excised. A previous study from our group showed that BCC is underestimated by cancer registries by a factor of 2–2.2 (5).
This study shows that skin SCCs represent a highly significant subset of NMSC, which has a large impact on healthcare resources. NMSC do not show up in most analyses due to the fact that BCCs are very rarely fatal, but SCCs of skin may metastasize and cause fatalities. The frequent exclusion of NMSC from national statistics on the basis that they are not fatal is fallacious. We show also when SCC of skin is included in national statistics for the most common cancers in the UK in 2011, it ranks as number 5, just behind breast, lung, prostate and colorectal (Fig. S11) (10).
We have estimated that the annual costs of diagnosing and treating skin SCCs in the UK for 37,428 cases of SCC would range from £33 to £46 million (6). These costs do not include patient costs incurred in the receipt of treatment, productivity losses and premature mortality which would impose large additional burdens to these estimated costs. However, it was estimated that the total cancer burden to the UK in 2009 was approximately £15.8 billion (excluding NMSC) (11), and skin SCC would only represent ~0.3% of this if included. Perhaps this is one potential reason that NMSC are not a high priority in purely financial terms.
These analyses show that 1) Skin SCC is one of the most common potentially fatal cancers in the UK. 2) Skin SCC has increased 2.8 fold over 10 years in our region, and is likely to have increased for the rest of the UK also. 3) SCC of the skin is likely to be an increasing burden to the total healthcare costs and resources of the UK in the future. 4) The estimates given by our cancer registries are likely to be a significant underestimate due to recognised inefficiencies in the system. 5) The continuing annual increases in both SCC Skin and BCC in the UK are not well recognised, and their impact on the UK’s healthcare is underestimated.
The authors declare no conflict of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2310
References


