


Maki Akahoshi-Ikeda1, Seiji Yoshizawa2, Junichi Motoshita3, Masutaka Furue4 and Satoshi Takeuchi1,4*
Departments of 1Dermatology, 2Rheumatology, 3Pathology, Federation of National Public Service Personnel Mutual Aid Associations, Hamanomachi Hospital, Nagahama 3-3-1, Chuo-ku, Fukuoka 810-8539, and 4Department of Dermatology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan. *E-mail: takeuchi-s@hamanomachi.jp
Accepted Feb 24, 2016; Epub ahead of print Feb 26, 2016
Pyoderma gangrenosum (PG) is a neutrophilic dermatosis induced by trauma or infection, which frequently appears on the lower legs. Various autoimmune diseases and systemic tumour necrosis factor (TNF)-α-blocking treatment cause PG, suggesting that T-cell-mediated reactions are involved in the aetiology. We report here for the first time a case of PG occurring during treatment with abatacept, a T-cell co-stimulation blocker. In addition, we discuss a possible underlying disease mechanism.
CASE REPORT
A 64-year-old woman had had rheumatoid arthritis (RA) since 10 years. Her condition had gradually deteriorated despite systemic treatment with corticosteroids and methotrexate. Although she was positive for anti-hepatitis type B virus antibody, systemic administration of immunosuppressants and biological agents was used with care to improve her seriously impaired quality of life. Tacrolimus and etanercept did not produce satisfactory results. She showed a good initial response to adalimumab; however, the biologic gradually became ineffective (secondary failure) and was replaced with infliximab, another anti-TNF-α treatment. Infliximab also showed secondary failure, even with an increased dosage. We then treated her with abatacept, a fusion protein composed of the Fc region of IgG1 and the extracellular domain of cytotoxic T lymphocyte-associated protein (CTLA)-4, which inhibits co-stimulatory transduction between dendritic cells (DCs) and T cells, to prevent their activation. The application of abatacept effectively soothed her RA symptoms, without prominent adverse effects. However, one year after the start of abatacept, accumulating red papules appeared on her right thigh and became aggravated, forming an ulcer with a moth-eaten appearance, red halo, and mild spontaneous pain over the course of the previous month (Fig. 1A). Blood tests indicated mild anaemia and elevation of C-reactive protein (CRP), immunoglobulin, and anti-nuclear antibody levels. Histological examination of the ulcerative lesion showed dense inflammatory infiltration through the dermis to the subcutaneous tissue (Fig. 1B). The abscesses formed a granulation tissue with numerous neutrophils, lymphocytes, and hyperplastic micro-vessels with fibrin deposition (Fig. 1C). The ulcerative lesion responded well to orally administered 20 mg/day prednisolone, and the dosage was tapered by 5 mg/day biweekly. The ulcer re-epithelized 8 weeks after its first appearance.
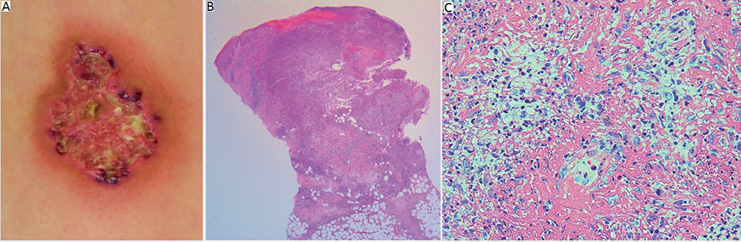
Fig. 1. Clinical manifestation and histopathology of the ulcerative lesion (5 cm in diameter). (A) Ulcer with a moth-eaten appearance, necrotic tissue, and a red halo. (B) Massive infiltration of neutrophils and lymphocytes through the dermis to the subcutaneous tissue (original magnification × 40). (C) Proliferation of small vessels with fibrin deposition containing numerous neutrophils observed within the abscess (original magnification × 400).
DISCUSSION
RA is a T-cell-mediated autoimmune disease. Therefore, co-stimulatory transduction via CD80/86 on DCs to CD28 on T cells, as well as major histocompatibility complex T-cell receptor transduction is important in the disease aetiology (1). In the later phase of T-cell activation, CTLA4, another CD80/86 ligand, appears on T cells to inactivate them with its much higher affinity to CD80/86 than that of CD28. Abatacept mimics the fundamental T-cell inactivation process with its fused CTLA4 extracellular domain (2) and is used for intractable RA.
PG is characterized by chronic, refractive skin ulcers induced by minor trauma or local infection. Systemic (or local) treatment with corticosteroids, immunosuppressants (3) and some biological agents (e.g. anti-TNF-α treatment) are reportedly effective treatments (4–6). Autoimmune diseases, such as ulcerative colitis, Crohn’s disease, RA, aortitis syndrome, and some biologics (7) cause PG, suggesting a possible involvement of T-cell-mediated reactions in the aetiology. Brooklyn et al. (8) showed that most of the infiltrating lymphocytes were T cells, and that they expanded oligoclonally, suggesting the presence of a specific antigen. Furthermore, Mittal et al. (9) showed that the same T-cell repertoires existed in the circulating blood flow, suggesting a contribution of systemic T-cell-mediated immunity to PG aetiology. Consistent with these reports, numerous CD4+ and CD8+ mononuclear cells were observed in the present case (Fig. 2A and B). In addition, CD8 T cells appeared to play an important role in the formation of neutrophilic dermatosis in an animal model (10).
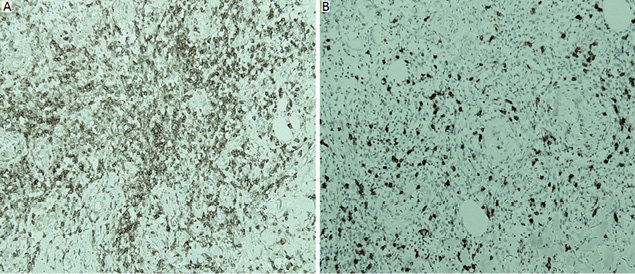
Fig. 2. Immunohistochemical staining of infiltrating lymphocytes. (A) CD4-positive lymphocytes are dominant in the mononuclear infiltrate, and (B) there are also many CD8-positive lymphocytes. (original magnification × 200).
Both RA itself and paradoxical reactions to biological agents (an effect opposite to that which would normally be expected) (11–13) could have caused PG in the present case. However, we consider the former option as less likely because the patient’s RA was well-controlled with abatacept (Fig. S11).
Theoretically, abatacept should suppress T-cell-mediated diseases, such as PG, by inactivating T cells. The agent, however, could enhance regulatory T-cell functions but diminish the number of circulating regulatory T cells (14). This might not affect its ability to control RA symptoms; however, we wonder if de novo T-cell-mediated reactions due to trauma and/or infection (known PG triggers) occurring under such conditions might induce PG. In addition, CTLA4 blockade could result in both reduced and enhanced Th1 responses depending on the degree of T-cell receptor cross-linking (15). We speculate that, in certain conditions, abatacept might facilitate a T-cell-mediated immune reaction by unbalancing the relationship between effector and regulatory T cells in terms of function and/or the cell number that could cause PG (16) as a paradoxical reaction.
In conclusion, we report here a case of PG in a patient with RA treated with abatacept and discuss a possible underlying disease mechanism.
The authors declare no conflicts of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2380
REFERENCES


