


1Department of Dermatology, Nagoya University Graduate School of Medicine, Nagoya, 466-8550, 2Department of Pathology, Tokyo Metropolitan Cancer and Infectious Diseases Center, Komagome Hospital, Tokyo, 3Division of Dermatology, Okazaki City Hospital, Okazaki, and 4Division of Pathology, Toyokawa City Hospital, Toyokawa, Japan. *E-mail: miro@med.nagoya-u.ac.jp
Accepted May 11, 2016; Epub ahead of print May 13, 2016
Angiofibroma of soft tissue (AFST) was first reported in 2012 (1). AFST is a tumour with a well-defined margin, characterized by angiogenesis and the proliferation of spindle cells. Clinically, AFST is a slow-growing tumour that most commonly occurs on the lower limbs, with a female predilection (1, 2). We report here a case of AFST on the face, which was diagnosed by the detection of gene rearrangement in the nuclear receptor coactivator 2 gene (NCOA2).
A 50-year-old woman visited a local clinic with a 2-year-history of a slowly growing subcutaneous mass on her left cheek (Fig. 1a). Palpation revealed a mobile, firm mass, 3 cm in diameter, with a well-defined margin, accompanied by mild tenderness. One year later, the patient underwent incisional biopsy of the mass and was referred to us for further evaluation and treatment. We examined the tumour with magnetic resonance imaging (MRI). The tumour had enlarged from 8 × 10 mm (Fig. 1b, c) to 10 × 25 mm in 12 months; therefore, total excision was performed.
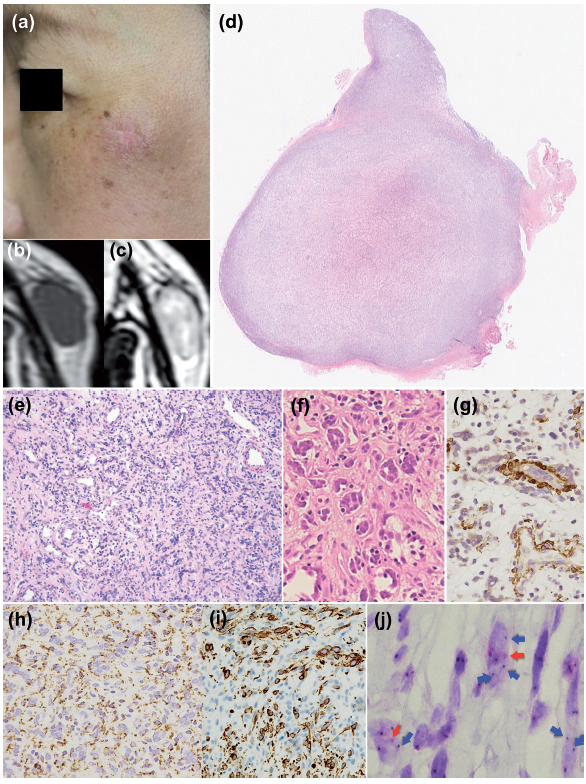
Fig. 1. Angiofibroma of soft tissue (AFST) (a) Clinical features of AFST on the patient’s face at her initial visit to us. There is a surgical scar on the tumour. (b) Magnetic resonance imaging (MRI) T1, (c) MRI T2; in MRI images, the patient has a well-defined mass on the left cheek. The size is 8 × 10 mm. T1- and T2-weighted MRI images illustrate the tumour as having hypointense and hyperintense signals, respectively. This imaging pattern is indicative of an inflammatory lesion or a benign tumour. (d) Histopathologically, the tumour is sharply demarcated with no apparent capsule (haematoxylin and eosin (HE) staining, original × 12.5). (e) The proliferation of spindle cells, small vessels and the infiltration of lymphocytes are seen in the tumour (HE staining, original × 40). (f) Giant cells are also observed in the tumour (HE staining, original × 200). Immunohistochemically, the tumour cells are (g) weakly positive for α-smooth muscle actin (α-SMA) and (h) positive for CD68 and (i) desmin (original × 200, respectively). (j) Chromogenic in situ hybridization (CISH) for detection of nuclear receptor coactivator 2 gene (NCOA2) rearrangement (original × 1,000). Unpaired signals (red and blue arrows), representing NCOA2 disruption, are observed in some tumour cells.
Histopathologically, the tumour was well defined, but un-encapsulated. It was located between the subcutaneous fat tissue and the zygomaticus minor (Fig. 1d–f). It was composed of spindle cells and giant cells, accompanied by a network of proliferating small vessels and myxoid stroma. Around the tumour, there was infiltration of inflammatory cells, mainly lymphocytes. Immunohistochemical investigation found that the tumour was positive for desmin (Fig. 1i) and D2-40, weakly positive for α-smooth muscle actin (α-SMA), partially positive for CD68 (Fig.1 g, h), and negative for CD31, CD34 and S-100. The Ki-67 index was 3%. Differential diagnoses considered were: nodular fasciitis, solitary fibrous tumour and giant cell angiofibroma; however, these were ruled out from the clinical and histopathological findings.
Considering the possibility of AFST, we therefore performed chromogenic in situ hybridization (CISH) with paraffin-embedded specimens of the lesion, using a break-apart probe for NCOA2, as reported previously (3–5). Some spindle cells were positive for gene rearrangement in NCOA2 (Fig. 1j). This finding led to a diagnosis of AFST.
To date, approximately 40 cases of AFST have been reported worldwide. AFST tends to grow slowly. In the literature, we found one case that had been followed up for more than 10 years before resection (1). AFST may be misdiagnosed as low-grade sarcoma (1). In fact, Marino-Enriquez & Fletcher (1) reported that 4 out of 28 AFST cases developed local recurrence, even though a positive surgical margin was detected at the initial resection in only one of the 4 patients with recurrence. Metastasis of AFST has never been reported (1). The most common sites of AFST are the limbs, particularly the lower extremities (1). To our knowledge, this is the first reported case of AFST on the face. AFST on the limbs is usually not tender; only 2 patients out of the 29 reported AFST cases on the limbs (6.9 %) reported feeling tenderness (1). In contrast, the present patient had tenderness on the AFST lesion on their face.
To confirm the diagnosis of AFST, we performed CISH for detection of gene rearrangement of NCOA2 and obtained positive results. It was reported that 7 out of 14 cases of AFST were positive for NCOA2 gene rearrangement (3). This is because NCOA2-rearranged cells can be infrequent and only found in limited numbers of tumour cells. In such a tumour, CISH is a useful adjunct, which enables sensitive analysis of tumour cells and which is superior to reverse transcription polymerase chain reaction (RT-PCR) and fluorescence in situ hybridization (FISH) (5).
In conclusion, the present case clearly indicates that AFST can occur on the face and suggests that CISH for NCOA2 gene rearrangement is a powerful diagnostic tool for AFST, especially for AFST lesions on unusual body sites. To avoid overtreatment, we propose that it is important to make a precise diagnosis of AFST and to distinguish it from more aggressive tumours of the soft tissues.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize