


1Department of Dermatology and Venereology, Institute of Clinical Sciences, The Sahlgrenska Academy at University of Gothenburg, 2Department of Dermatology and Venereology, The Sahlgrenska University Hospital, Gothenburg, and 3Department of Dermatology and Venereology, Skåne University Hospital, Lasarettsgatan 15, SE-221 85 Lund, Sweden. *E-mail: henrik.sonnergren@med.lu.se
Accepted May 11, 2016; Epub ahead of print May 13, 2016
Pinch-grafting is a treatment for foot and leg ulcers, first described by Reverdin in 1869. A pinch of the epidermis and a thin layer of dermis is lifted with the fingers or a nipper and removed with a scalpel and used as a skin-graft on the ulcer bed (1). Several reports have described acceptable results for pinch-grafting with 22–40% healing rates at 8–12 weeks (2–5). Punch-grafting is an alternative treatment, in which a biopsy punch is used instead of a nipper for extracting the graft from the donor site (6). However, only one study, with 22 patients, has evaluated punch-grafting of leg and foot ulcers, showing a 50% healing rate at a mean of 2.5 months (7).
At Sahlgrenska University Hospital, punch-grafting has primarily been used for ulcers when conservative treatment has been unsuccessful. The method has been described previously (7).
Considering the lack of clinical evaluations of the punch-grafting technique, the aim of the current study was to evaluate the clinical outcome of punch-grafting as a treatment for difficult-to-heal leg and foot ulcers.
The study protocol was assessed by the regional ethics review board to not require ethical approval, since it was a retrospective evaluation of a treatment used in clinical practice.
A single-centre retrospective cohort study was performed by collecting data from electronic medical records at the Department of Dermatology, Sahlgrenska University Hospital. Included cases had been treated with punch-graft for one or several leg or foot ulcers from January 2004 to September 2013 (for exclusion criteria see Table SI). Baseline was set as the date of the first punch-grafting. After grafting, compression therapy is performed as standard, with a low-elastic compression bandage, for all patients with venous and mixed arterial-venous insufficiency ulcers, as well as for ulcers of other aetiology if arterial circulation permits. In selected cases of venous insufficiency, intermittent pneumatic compression (IPC) is used in addition. For assessment of a 12-month follow-up, charts were requested from the primary care provider and other healthcare providers.
In the study the classifications venous, arterial, pressure, diabetic, mixed or other ulcers were used. Due to the retrospective approach, ulcers were classified based on clinical assessment and diagnosis in the medical charts. Data were obtained regarding patient characteristics, comorbidity, healing frequency at 3 and 12 months, time to wound closure for ulcers healed within 12 months, hospitalizations, outpatient visits, vascular surgery, antibiotic treatments, analgesic medication and complications to treatment.
A number of ulcers were grafted more than once; however time to wound closure was calculated based on the date of the first punch-graft treatment. Wound closure was defined as medical record descriptions of complete wound healing, complete re-epithelialization and no need for further treatment with dressings, in accordance with the European Wound Management Association (EWMA) guidelines (8).
Fisher’s exact test and Wilcoxon rank-sum test were used for 2-sample comparisons. A Cox proportional hazards model was used with the wounds “time to healed” as the dependent variable. Healing times longer than 365 days were treated as censored at 365 days. Ulcer duration before treatment, type of wound, patient age and localization were used as predictors. The same model was used for each wound type, with year of treatment (categorized as 2004 to 2008, or 2009 to 2013) added as a predictor. All tests were 2-tailed. p < 0.05 was considered statistically significant.
A total of 213 patients with 284 ulcers treated with punch-graft were included in the study (mean?±?standard deviation (SD) age 73.2?±?13.6, age range 23–96 years, 61% women). The patients had a high degree of comorbidity regarding cardiovascular disease, diabetes, history of deep venous thrombosis and vascular surgery in the punch-grafted extremity (Table SII). Table SIII presents the patient baseline data.
The distribution of ulcer type showed venous aetiology in 43.7% of ulcers, followed by mixed, other, arterial and diabetic ulcers, but no pressure ulcers (Table SIV). The group of other ulcers mainly included vasculitis and traumatic ulcers, as well as numerous other aetiologies. The mean?±?SD duration of all ulcers was 24.9?±33.8 months (Table SIV).
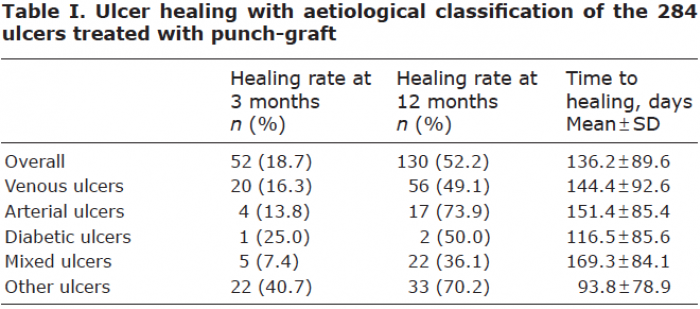
At 3 months 18.7%, and at 12 months 52.2%, of ulcers were healed. The mean?±?SD overall time to healing was 136.2?±?89.6 days (Table I). Ulcer healing at 3 months stratified regarding patient age indicated a correlation that younger patients healed to a larger extent (Table SV) but statistical models showed no significant correlation between time to healing and ulcer duration (p = 0.285), patient age (p = 0.478) or location of the ulcer (p = 0.4776). A correlation between time to healing and type of ulcer was found only for arterial (p = 0.0486) and other ulcers (p = 0.0005). Other ulcers had the shortest mean time to healing.
The overall use of analgesics was slightly higher at 3 months compared with baseline, but included less use of non-narcotic prescriptions, narcotic prescriptions and transdermal analgesic patches (Table SIII). Complications were found in 27.7% of patients (n = 59), the most common being infection of the treated ulcer (n = 55) and the donor site (n = 3), and 28.5% (n = 81) underwent one or several repeated punch-graftings (62 repeated once; 14 repeated twice; 5 repeated 3 times). Notably, 2 complications of difficult-to heal ulcer at the donor site both occurred in patients with vasculitis.
The clinical outcome of punch-graft treatment in the current study showed a markedly lower healing rate than the 40% at 3 months reported for pinch-graft (3) and also compared with the 50% in the only previous study of punch-graft (7). In comparison, randomized trials of grafting of venous ulcers with human skin equivalent have reported 63–71% healing and split-thickness autografts have been reported to result in complete healing of 67.5% of cases at 6 months (9).
As expected (10, 11), venous aetiology was the most common in the current study. Mixed ulcers were more common than expected, which may be explained by the fact that this type is more difficult to heal compared with other aetiologies and, therefore, punch-graft is more often used for this group. Furthermore, the age distribution indicates that punch-graft is more commonly used in the elderly population, which corresponds with leg ulcers being more frequent in older people (12). However, this may also suggest that no selection has been done for punch-graft treatment, and that there is a lack of criteria to determine which patients may benefit from the punch-graft treatment.
The mean duration of treated ulcers was 2 years, and ulcers chosen for punch-graft are thus the ones that have failed to heal and where other treatments have shown unsatisfactory results. This means that the punch-graft-treated patients include the ulcers with a poor healing potential, affecting the healing result. However, no significant correlation between the ulcer duration and healing after punch-graft was found.
Since this is a retrospective non-controlled cohort study the conclusions that can be drawn are limited. Data on ulcer size and diameter were not available from all patient charts, and data on ulcer healing could thus not be correlated with ulcer size. Data on ulcer aetiology were based on the clinical assessment and diagnosis in the medical charts and thus were not standardized. Neither could a standardized pain assessment, such as VAS, before and after treatment be utilized, due to the retrospective study approach. It would also be of greater value to have a control group undergoing another treatment method for comparison of the outcome in order to evaluate the effectiveness of punch-grafting.
The healing rates in this study were lower than those in previous studies on pinch- and punch-graft, indicating that the method is not selected for the patients with most potential benefit of the treatment. Even so, it is difficult to draw any conclusions regarding these results, due to the study design, and a comparative study is required.
The authors warmly thank Mr Martin Gillstedt, MSc, Department of Dermatology, Sahlgrenska University Hospital, for excellent statistical assistance with this study.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize