


1Center for Chronic Pruritus, Department of Dermatology, University Hospital Mu?nster, Münster, 2CVderm, German Center for Health Services Research in Dermatology, Institute for Health Services Research in Dermatology and Nursing, University Medical Center Hamburg-Eppendorf, 3Research & Development, Beiersdorf AG, Hamburg, Germany
Currently valid itch intensity scales, such as the visual analogue scale (VAS), are indispensable, but they can be influenced by the patient’s overall health status. The aim of this study was to evaluate the reliability and validity of the Dynamic Pruritus Score (DPS), a new instrument comparing reduction in current pruritus with a defined earlier time-point. Eighty-one randomly selected adults (50 females, mean age 53.9 years) recorded their pruritus at visit 1 and repeatedly at visit 2 on the DPS, VAS, numerical rating scale, and on health status questionnaires (EuroQol; EQ-5D), skin-related quality of life (Dermatology Life Quality Index; DLQI), anxiety and depression (Hospital Anxiety and Depression Scale; HADS) and patient benefit (Patient Benefit Index; PBI). Intraclass correlation showed high reliability for both DPS and VAS (r > 0.9, p < 0.001), while the DPS has shown higher concurrent validity (rDPS to PBI = 0.570; p < 0.001). The DPS can then be considered an alternative instrument to the VAS for assessment of pruritus in adults. Further research is needed to confirm these results with a more representative sample size.
Key words: pruritus; itch; Dynamic Pruritus Score; measurement tools; transient receptor potential melastatin-8; TRPM8.
Accepted May 16, 2016; Epub ahead of print Jun 28, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Sonja Ständer, Center for Chronic Pruritus, Department of Dermatology, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: sonja.staender@uni-muenster.de
Chronic pruritus (CP), associated with multiple diseases, is one of the most frequent symptoms in medicine and has a high impact on quality of life (QoL) (1). The current point-prevalence of CP, defined as pruritus lasting for more than 6 weeks (2), is estimated at 14–17% in the general population, with a higher prevalence in dermatological patients (3, 4). At present, intensity scales, such as the visual analogue scale (VAS) or numeric rating scale (NRS), are most frequently used to measure the intensity of pruritus (5, 6). Although the VAS and NRS remain essential, they are not optimal instruments, because their scores are influenced by a variety of pruritus-independent factors, such as mood or sleep disorders, psychosomatic symptoms, overall health status, comorbidities and co-medications (6–8). VAS, NRS and the verbal rating scale (VRS) allow static 1-point-ratings only and might not indicate the real direction of change in pruritus. Their advantage is that they provide valid results on clinical benefits when used together with short recall periods of 1–3 days (9). However, taking into account information from only the previous 3 days limits the impression of the overall course and trend in pruritus and may give false-positive or false-negative feedback.
The concept of a 2-point framed health outcome measurement, comparing the current situation with that of an earlier time-point is established for pain, using the Patient’s Global Impression of Change (PGIC); an 8-point scale ranging from strong worsening to strong improvement (10). In neuropathic pain, the PGIC shows more sensitive data on the course of pain compared with the intensity scales painVAS and painNRS (10). Accordingly, PGIC is recommended by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT; www. http://www.immpact.org/) for use in clinical trials as a core outcome parameter (11). Such an instrument has not yet been developed specifically for chronic pruritus, although the pruritus 5-D scale makes an attempt in this direction (12). The third question of the 5-D scale asks: “Over the past 2 weeks has your itching gotten better or worse compared with the previous month?” Three answers are possible for getting better (completely resolved, much better, little bit better), 1 for “Unchanged” and 1 for “Getting worse”. However, this scale is not sensitive enough to determine the exact course of itch, as it does not allow the selection of numbers in-between the predefined answers. In dermatology, the Patient Benefit Index (PBI) follows the concept of a 2-time-point framed measurement of a therapy’s benefit and showed great advantages in the assessment of the course of dermatoses (13). The PBI calculates a score out of 2 questionnaires, which were completed before and after the therapy. At baseline, patients rank 27 pre-defined aims related to the expected benefit of a therapy on a 5-point scale (from not important to very important). After therapy, patients are shown the same list of aims again and indicate to what extent these goals have been achieved (from ‘’not at all’’ to ‘’very much’’). Out of these 2 questionnaires, an index is calculated by averaging the preference weighted results of all items (results between a score of 0–4 possible; clinical meaningful cut-off: PBI≥1) (14). One of the first items in PBI is “improvement of itch or burning” but by collecting more than 20 additional items it does not allow a final conclusion to be drawn on the course of pruritus alone. A tool for pruritus, which is comparable to the PGIC in pain, and which is addressed to capture specifically the course of itch was not yet available. However, as new instruments minimizing the influence of external parameters are necessary for improved pruritus measurement, we made an attempt to develop such a tool. The objective of this study was the development, and testing for feasibility and validation of a new itch measurement tool, the so-called Dynamic Pruritus Score (DPS). The DPS assesses the change in pruritus intensity, compared with a defined earlier time-point, enabling a more precise interpretation of the course of pruritus.
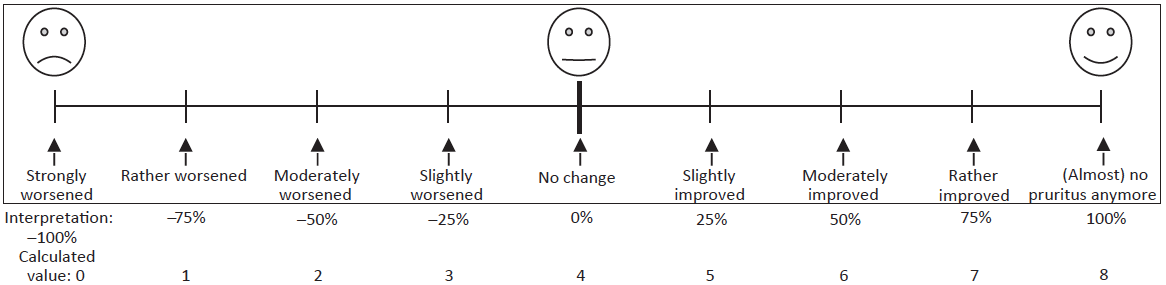
In an expert panel, members of the special interest group Scoring Itch in Clinical Trials of the International Forum for the Study of Itch (IFSI) (6), developed and finally agreed on 3 different versions of a scale, which enable the assessment of current pruritus in comparison with an earlier time-point: (i) a horizontal line measuring itch improvement with 11 scale marks, labelled with numeric-verbal description (e.g. “50% improvement: itch only half as intense”), in addition asking the patient to state the percentage improvement or, alternatively, stating that itch has increased; (ii) a line with 2 extremes (right: 100% reflecting (almost) complete improvement of CP; left: –100% meaning severe worsening of CP; each compared with an earlier time-point). In-between, anchors mark the area of 0: no change; 25%/–25%: slightly improved/worsened, 50%/–50%: moderately improved/worsened, 75%/–75%: rather improved/worsened. Three faces above the line help the subjects to understand the DPS (Fig. 1); (iii) 2 VAS measuring itch intensity at treatment start and currently, with extremes labelled with “no itch” and “worst imaginable itch” and additional 5 “smileys” each.
Fig. 1. Dynamic Pruritus Score (DPS) scale (visual version for patients). Patients can see the line with verbal descriptions and faces above (in the frame) and an explanation that the extreme right equals 100% improvement (=no pruritus), and extreme left 100% worsening (=strongly worsened pruritus) compared with an earlier time-point (in this study, 2 weeks previously).
These variants of scales were applied in 38 consecutively recruited patients with chronic itch of the Center for Chronic Pruritus in Münster for feasibility: patients completed all 3 scales and indicated on a separate feasibility questionnaire which of these versions they found: (i) easy, (ii) difficult, and (iii) quickest to complete (multiple selections in each question possible). Scale version II was most often rated easy to complete (scale I, n = 13; scale II, n = 24; scale III, n = 19) and less difficult to complete (scale I, n = 3; scale II, n = 0; scale III, n = 5). Version II was rated quickest to complete (scale I, n = 9; scale II, n = 12; scale III, n = 10). Version II showed the smallest number of missing values (scale I, n = 3; scale II, n = 1, scale III, n = 2). There were several misunderstandings in the use of scales: in scale I, some patients did not use the scale, but wrote comments (n = 3) or made several crosses (n = 2). In scale II, some made the cross on faces instead of the line (n = 2). On scale III, the most irregularities occurred, such as making the cross on faces (n = 5), between faces (n = 2), or on the side next to the scale (n = 1), or writing a comment (n = 1).
We chose to continue with version II, because it was the best in all categories (most easy, least difficult, and quickest), had the lowest number of both missing values and the lowest number of misunderstandings (15).
In a prospective, longitudinal, open study conducted at the Center for Chronic Pruritus, Department of Dermatology, University Hospital Mu?nster, Germany, the reliability and validity of DPS was assessed. Data management and statistical analysis were conducted in the German Center for Health Services Research in Dermatology (CVderm) of the Institute for Health Services Research in Dermatology and Nursing (IVDP) of the University Clinics of Hamburg. All subjects gave written informed consent for data collection and analysis. The Ethics Committee of the University of Münster approved the trial (2010-179-f-S), which is registered at the German Clinical Trials Register #DRKS00005970.
Over a period of 37 months, 81 randomly selected subjects, aged 20–81 years, mean age 53.9 ± 16.3 years (31 males aged 57.1 ± 14.5 years and 50 females aged 51.9 ± 17.1 years) with chronic pruritus (> 6 weeks, VAS ≥ 3 and < 8, (VAS 0–10)) before visit 1. According to the classification of the IFSI, patients had pruritus on inflamed skin (37.1%; IFSI group I; atopic dermatitis (n = 28), chronic urticaria (n = 2), Table I), chronic pruritus on non-inflamed skin (but all with xerosis or single scratch lesions, 48.1%, IFSI group II) and chronic pruritus with chronic scratch lesions (14.8%; IFSI group III; i.e. prurigo nodularis (n = 12)) with 81.1% of the total subjects with xerosis and 34% of (non-prurigo) patients with scratch lesions (Table I) allowing the use of DLQI in all subjects (1, 16). Subjects showing pregnancy or lactation, active psychosomatic, psychiatric or malignant diseases, exacerbated and/or infected atopic dermatitis, addictive drug or medication abuse, allergy to any of the treatment’s ingredients, participation in another clinical study within the 4 weeks preceding the study, or using therapies up to 1–2 weeks before the onset of the study, which could influence its outcome (antihistamines, corticosteroids, immunomodulators, topical calcineurin inhibitors, topical steroids, menthol or capsaicin) were excluded from participation in this trial.
Table I. Summary of baseline demographics and clinical characteristics of 81 subjects
In order to enable detection of the pruritus course and a change in pruritus intensity, all subjects were treated twice daily with Eucerin® lotion (Beiersdorf) containing a cooling compound (combination of 2 transient receptor potential melastatin-8 (TRPM8) – agonists) during the course of the study (days 1–14) (17).
Data were collected before and after pruritus treatment. At day 1 (Visit 1) and before treatment the subjects completed the questionnaires related to skin type and skin condition, VAS (mean itch intensity within the previous 12 h: VASmean12h), the health state by EQ-5D (EuroQol (18)) and by VAS, the skin-related quality of life (Dermatology Life Quality Index; DLQI (1)), the anxiety and depression HADS (Hospital Anxiety (HADS-A) and Depression (HADS-D) Scale (19)) and the patient needs (Patient Needs Questionnaire; PNQ), which is the first page of the Patient Benefit Index-pruritus (PBI-P) (14)) questionnaires. NRS (Numeric Rating Scale (20)) was assessed by physician interview as following: average itch intensity within the previous 12 h (NRSmena12h), within the previous 2 weeks (NRSmean2wk), and maximum itch intensity in the previous 2 weeks (NRSmax2wk).
At Visit 2 (day 14) time 0, subjects again completed the skin condition, EQ-5D, DLQI, HADS, the patient benefit PBQ (Patient Benefit Questionnaire), which is the second page of PBI-P (14)) and the DPS (Fig. 1, German language version) questionnaires. For statistical comparison of DPS with itch intensity, subjects completed the current (current VAS) and the 2 weeks ago remembered (memory VAS) itch intensity via VAS. The physician again asked about NRSmean12h, NRSmean2wk, and NRSmax2wk. The percentual change in pruritus severity to baseline was assessed orally by the physician (physician dynamic score).
After 1 h (time 60) the subjects completed the same questionnaires again (except for the one about skin condition), in order to analyse the reliability of DPS. The DPS intended to assess the change in pruritus between V1 and V2. Thus, the subjects were asked how strongly the pruritus had changed in comparison with onset of therapy.
Similar to the analysis of the PGIC in pain, for statistical calculation, DPS response scales were coded into numbers with anchors at 9 possible answers: strongly worsened (0), rather worsened (1), moderately worsened (2), slightly worsened (3), no change (4), slightly improved (5), moderately improved (6), rather improved (7), (almost) no pruritus (8), allowing all numbers in-between 0 and 8 with higher values indicating less pruritus intensity (Fig. 1).
Data management was carried out with SPSS 22.0, and statistical analysis with SAS 9.3 for Windows. All data were described by distributional characteristics, such as mean and standard deviation (SD) or frequencies, depending on the type of the data. Test–retest reliability was explored for both DPS and VAS-Delta using the intraclass correlation coefficient (ICC) by applying a 2-way mixed model with measures of absolute agreement. The VAS-Delta was calculated by subtraction of current VAS at V2 at time 0 or at time 60 from VASmean12h at day 1. Concurrent validity was assessed by calculating correlations between DPS and the Delta of already validated instruments, such as EQ-5D, DLQI, HADS and PNQ and PBQ, the second item out of 27 of PBI-P (no longer experience of pruritus). The Delta of DLQI, EQ-5D, EQ-5D-VAS, HADS-A and HADS-D were defined as value at baseline V1 – value at V2 time-point 0 min. Correlations were tested with the Spearman rs coefficients, since the data were not normally distributed. The Mann-Whitney U test was applied to compare the DPS between atopic dermatitis and chronic pruritus patient groups.
Of the 86 subjects included in the study, due to loss of follow-up, a final total of 81 (94.2%) subjects were included in the analysis (Table I). At visit 1 (V1) before treatment, physician-assessed mean NRS showed a moderately intensive chronic pruritus (Table II). At V2, the NRS was significantly reduced (p < 0.001, Table II). The mean ± SD DPS noted by the physician was 34.5 ± 32.2% improvement. Patient-assessed mean DPS at time 0 (V2) was 5.0 ± 1.6 (n = 74) and, at 60 min, 5.2 ± 1.6 (n = 72) corresponding to the answer ‘’slightly improved’’ (Table III). Mean ± SD VAS-Delta was 2.4 ± 2.1 (n = 58) at time 0 and 2.5 ± 1.9 (n = 71) at time 60, which was a clinically meaningful reduction in pruritus (Table III). The corresponding mean ± SD values of Delta for DLQI, EQ-5D, EQ-5D-VAS, HADS-A and HADS-D were: 1.8 ± 4.3 (n = 62), –1.6 ± 14.3 (n = 66), –3.3 ± 18.0 (n = 65), 0.7 ± 2.3 (n = 62) and –0.9 ± 3.7 (n = 62). PBI-P was 1.4 ± 1.3 (n = 53) and PBI-P item 2 (“to be free of itching”) was 4.0 ± 0.3 (n = 51).
Table II. Delta of mean numeric rating scale (NRS) values from Visit 1 to Visit 2
Table III. Distributional characteristics of Dynamic Pruritus
Score (DPS) and VAS-Delta after treatment at V2, at time 0 and at time 60 min
The ICC for DPS was 0.911 (p < 0.001) and for VAS-Delta 0.938 (p < 0.001). Neither DPS nor VAS-Delta showed statistically significant differences between test and re-test.
At V2, time 0, the memory VAS was moderately correlated rs = 0.340 (p = 0.011; n = 55) with the VASmean12h at V1. The DPS was moderately correlated rs = 0.427 (p < 0.001; n = 55) with the VAS delta (memory VAS – current VAS). The correlation between DPS and VAS Delta rs = 0.131 (p = 0.339; n = 55) was not statistically significant. Both DPS (rs = 0.035; p = 0.737; n = 74) and VAS-Delta (rs = 0.039; p = 0.773; n = 58) were not statistically correlated with age.
Correlations between DPS or VAS-Delta and DLQI-Delta, PBI-P, PBI-P item 2, EQ-5D-Delta, EQ-5D-VAS Delta, HADS-A-Delta and HADS-D-Delta were also calculated (Table IV). In contrast to VAS-Delta, where all correlations were not statistically significant, DPS was moderately correlated with DLQI-Delta rs = 0.367 (p = 0.005) and strongly correlated with physician’s DPS rs = 0.526 (p < 0.001) and PBI-P rs = 0.570 (p < 0.001).
Table IV. Spearman’s correlations of Dynamic Pruritus Score
(DPS) and of VAS-Delta with other pruritus measurement instruments
Subgroup analysis in the atopic dermatitis and chronic pruritus groups did not show any statistically significant difference (p = 0.469) between their DPS distributions. The other subgroups were too small for statistical analysis.
In the past we have shown that although VAS and NRS both have high discriminative sensitivity for assessment of pruritus, both are influenced by a tendency of subjects to choose towards the middle of the scales, especially in the category of moderate pruritus (VAS/NRS values ~5) (8). This tendency is frequently observed in daily routine, and impairs the correct interpretation of pruritus intensity, both in daily routine and in clinical trials. In order to reduce such confounding factors we developed the DPS, which assesses the total change in pruritus intensity in relation to an earlier time-point. Thus, this instrument allows us to obtain information about the direction of pruritus change over a longer time-period (in this study: 2 weeks), independent of other factors.
In our study, NRS values decreased significantly, and the distribution of VAS-Delta at both time-points 0 and 60 min at V2 were negatively skewed, confirming a reduction in pruritus. This reduction could be related to the daily-applied TRPM8-treatment (17), although this study was not controlled. However, this allows us to analyse the reliability of the DPS in the clinical context of a course change in pruritus. All subjects assessed the different scales repetitively after a time interval of 1 h, in order to evaluate whether the scales were reproducible. DPS has shown high reliability (21) with an ICC of 0.911 (p < 0.001). Although VAS-Delta showed slightly higher reliability, with an ICC of 0.938 (p < 0.001), DPS was better in terms of concurrent validity. DPS was moderately correlated with DLQI-Delta rs = 0.367 (p = 0.005) and strongly correlated with the dynamic score noted by the physician rs = 0.526 (p < 0.001) and with PBI-P rs = 0.570 (p < 0.001) when testing Spearman’s correlations between DPS and already validated instruments, such as EQ-5D, DLQI, HADS and PBI-P. On the other hand, VAS-Delta (12 h recall period at each visit) was neither correlated with any of the valid quality of life instruments (recall period of 7 days) nor with the other assessments (HADS, PBI, EQ-5D). The difference in concurrent validity between DPS and VAS-Delta was unexpectedly high, but demonstrates that a different method of assessment of pruritus might give different results. The better concurrent validity of DPS might point to the fact that data assessed by DPS reflects to a higher degree the outcome that is related to other QoL measures in comparison with VAS. Irrespective of the initial severity of pruritus at baseline, DPS normalizes the assessment of the course of pruritus in all patients, by asking for the percentage change between –100 and +100. This results in comparable data between patients. Using VAS, the baseline is different between patients, resulting in different VAS-Delta, even if patients experience the same reduction in pruritus. For example, a patient with a baseline of 8 and a VAS-Delta of 4 has a 50% reduction, similar to a patient with a baseline of 4 and a VAS-Delta of 2. Thus, the calculation of mean delta values in a cohort of patients might be misleading. This challenge of VAS-Delta interpretation is an issue for the statistical analysis and determination of the (minimal) clinical benefit. Finally, a methodological bias in this study cannot be ruled out completely, as the recall periods for the validated questionnaires are long (e.g. DLQI=7 days) and more comparable to DPS, which considers the whole time between baseline and end of therapy, while VAS reflects only the previous 12 h (in this trial).
In conclusion, the DPS is the first tool that is comparable to PGIC in pain and specifically captures the course of itch. Similar to the PGIC in pain we coded the DPS response scales into numbers (0–9). This is a feasible calculation in clinical trials. An alternative for clinical use is to display the results as percentage change, which might be more understandable information. The DPS validated here for a recall period of 2 weeks can be implemented in clinical trials, which follow a 2-week-visit interval. The 4-week interval is not yet validated, but seems likely to show similarly good results. This study shows that DPS could be considered as an alternative or additional instrument to VAS, to assess pruritus from the patient’s perspective. Nevertheless, a multicentre study would be required to confirm and extend the results of the current trial with a more representative sample of subjects.
The authors would like to thank Ngoc Quan Phan for assistance in patient recruitment and Helena Karajiannis for assistance in the preparation of the manuscript.
The study was sponsored by Beiersdorf AG, Hamburg, Germany. KAJ and GN are employees of Beiersdorf. SST has received research grants and honorariums from Beiersdorf for this study. The other authors declare no conflicts of interest.
The DPS licence is held by Dr Ständer. For use in clinical trial: please contact sonja.staender@uni-muenster.de. For academic use: free. Trial registration at DRKS #DRKS00005970.


 Click to show fullsize
Click to show fullsize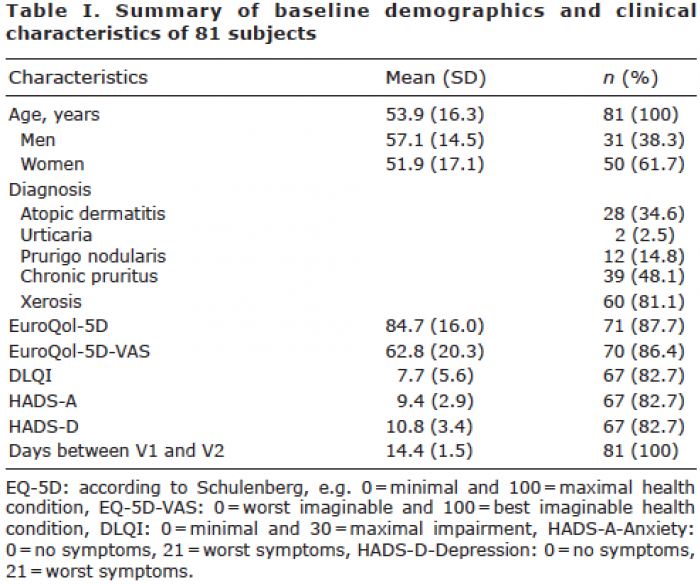 Click to show fullsize
Click to show fullsize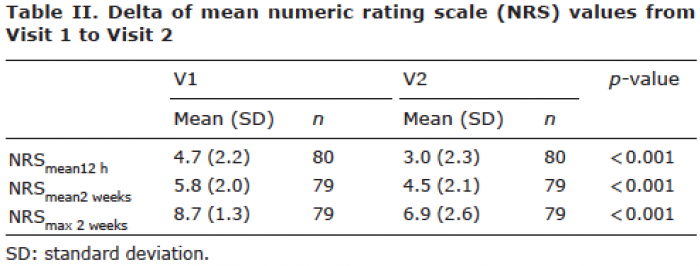 Click to show fullsize
Click to show fullsize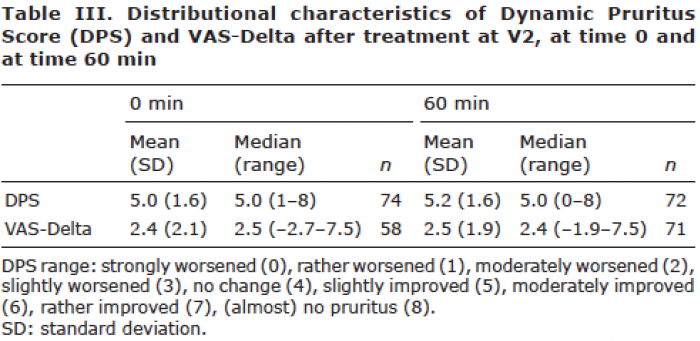 Click to show fullsize
Click to show fullsize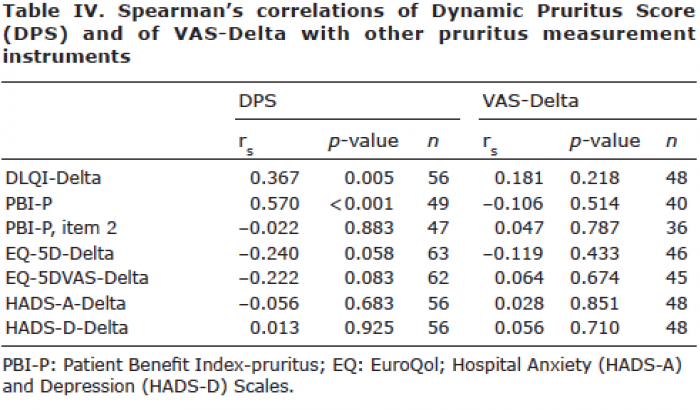 Click to show fullsize
Click to show fullsize