


Departments of 1Dermatology and 2Pediatrics, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya 466-8550, and 3Department of Medical Technique, Nagoya University Hospital, Nagoya, Japan. *E-mail: takeichi@med.nagoya-u.ac.jp
#These authors contributed equally and should be considered as first authors.
X-linked agammaglobulinaemia (XLA), also known as Bruton’s agammaglobulinaemia, is characterized by low or negligible levels of serum immunoglobulins (1). XLA is caused by mutations in the gene coding for Bruton’s tyrosine kinase (BTK). Deficiency of BTK leads to a developmental block in B-cell differentiation; hence, patients essentially lack antibody-producing plasma cells and are susceptible to various infectious diseases (2). Infections with unusual organisms, such as Helicobacter cinaedi, may also be troublesome (3). H. cinaedi, previously known as Campylobacter cinaedi, has been frequently reported in HIV-positive patients (4). In immunocompromised patients, the spectrum of illnesses caused by H. cinaedi includes recurrent fever, bacteraemia, arthritis, osteomyelitis, cellulitis, abdominal abscesses and diarrhoea. However, signs of inflammation, such as fever, may be delayed in immunocompromised patients, possibly due to the absence of functional antibodies required for opsonization and phagocytosis (3). A few cases of XLA with chronic infections, leg cellulitis and pyoderma gangrenosum-like ulcer, caused by H. cinaedi have been reported, although common Helicobacter species have been recognized as pathogens in many more patients with XLA (3, 5, 6). In this report, we describe a patient with XLA complicated by recurrent cellulitis caused by H. cinaedi.
The proband is a 38-year-old Japanese man with agammaglobulinaemia that was diagnosed in infancy. He had been treated with pH4-treated acidic normal human immunoglobulin. He had had recurrent episodes of feverish, painful swelling and erythemas on the dorsum of the right hand, the left lower leg and the left ankle since the age of 36 years. On one occasion, the feverish swelling and erythemas accompanied by pain on the left lower leg was also accompanied by high fever and elevation of circulating C-reactive protein at 2.36 mg/dl (normal range: 0–0.3 mg/dl) and he was hospitalized. The results of laboratory tests were as follows: white blood cell (WBC) count 8,400/mm3 (normal 3,800–8,500/ mm3); IgG 1,169 mg/dl (870–1,700 mg/dl) under treatment with pH4-treated acidic normal human immunoglobulin; IgA < 1 mg/dl (110–410 mg/dl); and IgM < 1 mg/dl (35–220 mg/dl). One week after the onset of swelling, the erythemas developed into brown macules (Fig. 1A, B). A skin biopsy from the left lower leg revealed slight fibrosis and mild lymphocytic infiltration in the upper dermis. Repeated cultures for microorganisms from venous blood samples detected a spirillum (Fig. 1C). No bacterial culture or PCR tests were performed on the skin samples. H. cinaedi was confirmed by PCR using the specific primers for the 16S rRNA of H. cinaedi (7) and by mass spectrometry (MS) with Vitek MS (BioMérieux, Durham, NC, USA), using a matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) system. Intravenous ampicillin/sulbactam (6.0 g/day) for one week followed by oral amoxicillin (1,500 mg/day) decreased the skin redness and improved the laboratory results, but there was a recurrence one month later. Treatment was switched to oral minocycline (200 mg/day) for 3 months based on the results of antimicrobial susceptibility tests, which reduced the frequency of recurrence from once per month to once every 3 months.
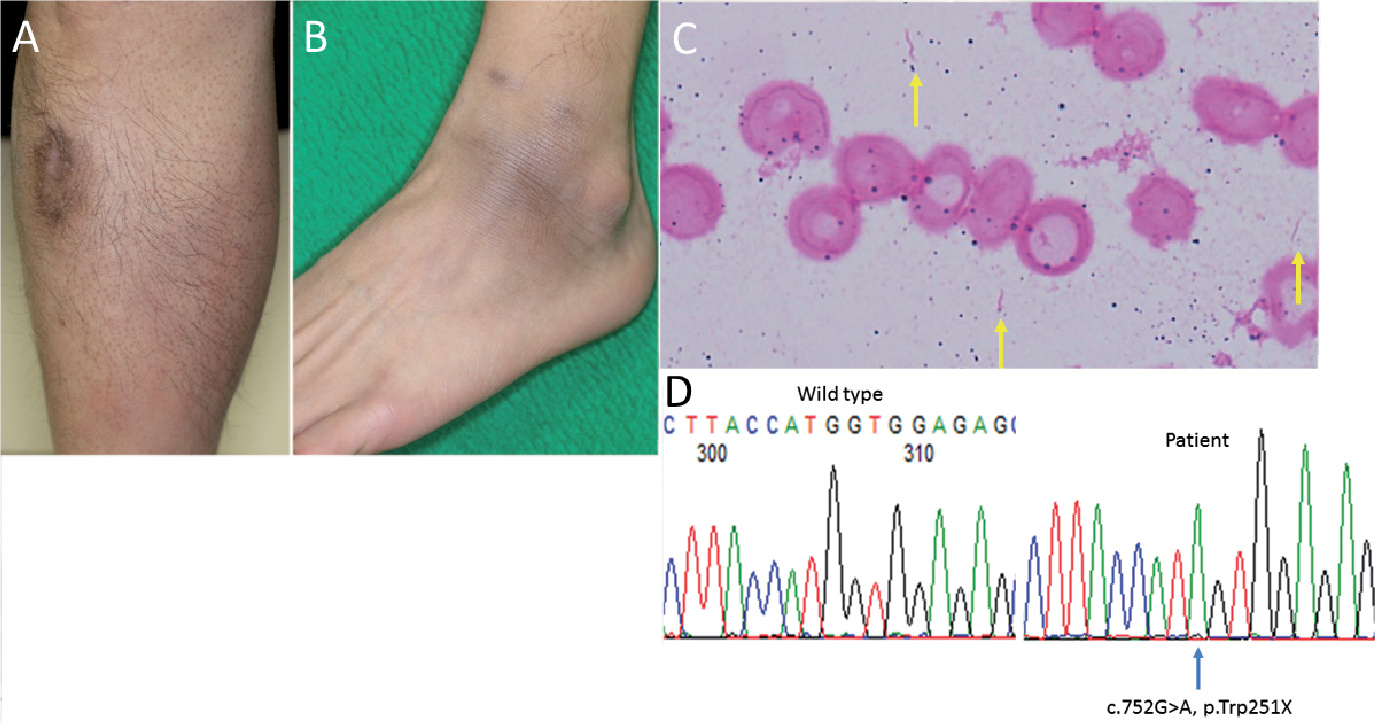
Fig. 1. Clinical images and microbial smear examination of the patient. Brown macules and swelling are present on (A) the left lower leg and (B) the left ankle one week after the onset of swelling. (C) Gram-staining of the microbial smear from the patient’s peripheral blood culture reveals spirilla (yellow arrows). (D) Sanger sequencing confirms a hemizygous c.752G>A transition (p.Trp251X) of BTK in the patient.
Ethical approval was obtained and all research was performed in accordance with the principles of the Declaration of Helsinki. After written informed consent was obtained, BTK gene mutational analysis was performed on the affected individual. Sanger sequencing confirmed a novel hemizygous nonsense mutation in BTK, c.752G>A (p.Trp251X) (Fig. 1D), according to GenBank accession no. NM_000061.
The truncating mutation c.753G>A at the identical tryptophan residue Trp251 was reported previously in BTK as a pathogenic variant in an individual with XLA (8). In addition, a nonsense mutation of the next tryptophan, p.Trp252X, has been reported (9, 10). Thus far, no strong correlation has been observed between a specific mutation in BTK and the severity of the disease, although individuals with amino acid substitution mutations or splice mutations tend to be diagnosed at older ages and to have milder deficiency of serum IgM and slightly more B cells in peripheral circulation (11).
H. cinaedi inhabits the intestinal tract of various healthy
animals, including hamsters, rats, cats, dogs, foxes, monkeys and humans. The present patient had kept a cat for 10 years. Bacteria derived from the cat’s bowel or the patient’s own bowel might have invaded the skin through minor traumas, cutaneous ulcers or erosions, or lesions of folliculitis or tinea pedis, which might have led to the bacteraemia and recurrent cellulitis, although the exact route of entry may not be identifiable (12, 13).
We detected H. cinaedi by specific PCR and matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS). MALDI-TOF MS is a recently developed efficient method for direct routine identification of bacterial isolates in blood culture, and this technique will probably replace conventional identification methods of bacteria in blood cultures (14, 15). However, in the case of a mixture of species, only one is identified, and false identification can occur with MALDI-TOF MS (14). Thus, Gram-staining of blood culture samples is still necessary. It is also important for clinicians to consider the possibility of chronic infections caused by unusual organisms, especially in immunocompromised hosts.
In conclusion, we report here an XLA case with chronic skin infection caused by H. cinaedi. Our results strongly suggest the importance of checking bacteraemia carefully by the appropriate techniques in immunocompromised patients, such as those with XLA.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize