


1Institute of Environmental Medicine, Karolinska Institutet, 2Department of Clinical Science and Education, Stockholm South General Hospital, Karolinska Institutet, and Sach’s Children’s Hospital, and 3Institute of Environmental Medicine, Karolinska Institutet, and Centre for Occupational and Environmental Medicine, Stockholm County Council, Stockholm, Sweden
#Both authors contributed equally and should be considered as first authors.
Water exposure on the skin of the hands has previously been studied in adults. The aim of this study was to investigate self-reported water exposure in adolescents in the BAMSE cohort in Stockholm, Sweden. A questionnaire including a question on daily water exposure on the hands was answered by 3,091 adolescents at age 16 years. Exposure > 10 times/day was reported by 28.7% and > 20 times/day by 3.1%; boys had somewhat higher exposure than girls (p = 0.03). In a multivariate analysis, adolescents with dry skin reported higher exposure (adjusted odds ratio (ORadj) 1.4; 95% CI 1.2–1.7), while no statistically significant exposure differences were found in relation to hand eczema or atopic dermatitis. Reported exposure may be considered as baseline exposure during a period of life with limited occupational and domestic duties.
Key words: atopic dermatitis; dry skin; hand eczema; risk factor; wet work.
Accepted Jul 4, 2016; Epub ahead of print Jul 7, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Birgitta Meding, Institute of Environmental Medicine, Karolinska Institutet, Box 210, SE-171 77 Stockholm, Sweden. E-mail: birgitta.meding@ki.se
Water exposure on the hands in adults and wet work have been studied in a number of recent publications, with the primary focus on occupational exposure (1–10). Large differences in exposure have been shown previously in the adult general population in Sweden, with the highest exposure reported in jobs in the service sector, e.g. kitchen and restaurant work, cleaning and hairdressing (3, 4, 9). Water exposure correlates to the wider concept of “wet work” (3) and is one of several causative factors for hand eczema (11, 12). In Germany there is a regulation defining “wet work” as having wet hands for > 2 h/day, or frequent daily hand washing, or wearing occlusive gloves for > 2 h/day (13). Non-occupational water exposure in adults is also considerable (10). However, little is known about water exposure on adolescents’ hands.
The present study is part of the epidemiological project BAMSE (Barn [children], Allergy, Milieu, Stockholm, Epidemiological survey) (14). In this project, lifestyle and environmental risk factors for the development of atopic dermatitis (AD), asthma and rhinitis are studied. Results regarding the occurrence of hand eczema, the correlation between AD and hand eczema and the prevalence of contact allergy have been reported previously from the project (15–17). At follow-up at 16 years of age a question on frequency of daily water exposure on the hands was included.
The aim of the present study was to investigate the extent of self-reported water exposure on the hands in adolescents in a population-based cohort study.
The BAMSE project includes a closed population-based birth cohort. The children were recruited consecutively at birth and followed up to 16 years of age (14). All children born between 1994 and 1996 in predefined areas of Stockholm, Sweden, were invited to participate. Seventy-five percent (n = 4,089) of the eligible children were included (14). Data on environmental exposure and history of parental allergy were obtained shortly after birth (median age 2 months). Subsequently, parents answered questionnaires concerning manifestations of AD, asthma and rhino-conjunctivitis when the children were 1, 2, 4, 8, 12 and 16 years of age. At the follow-ups at ages 12 and 16 years the children also answered questionnaires. A question about water exposure on the hands was included in the questionnaire completed at 16 years of age, as were questions about hand eczema and dry skin (see below).
A total of 4,089 children was included in the original BAMSE cohort; retention through to age 16 years was 78% (n = 3,181) (17). In the present study, the population is defined as all adolescents who answered the question on water exposure; in total 3,091 (97.2%), girls 1,573/3,091 (50.9%) and boys 1,518/3,091 (49.1%). Most (99%) were still attending school and 98% were living with at least one of their parents.
Water exposure. The question used was: “How many times a day are your hands exposed to water?” There were 5 possible responses (not at all, 1–10 times, 11–20 times, 21–30 times, and > 30 times).
Dry skin. “Have you during the past 12 months been bothered by dry skin?” (yes/no).
Hand eczema. For lifetime prevalence the question was: “Have you ever had hand eczema (itching eruptions, vesicles or itching rash)?” (yes/no), and for the 1-year period prevalence “Have you had hand eczema on any occasion during the past 12 months?” (yes/no) (15).
Atopic dermatitis. AD at age 1, 2 and 4 years: dry skin and itchy rash with a typical age-specific location for at least 2 weeks the year before follow-up and/or doctor’s diagnosis of eczema since the last follow-up. AD at age 8 and 16 years: dry skin in combination with itchy rash and typical localization the year before follow-up and/or doctor’s diagnosis of eczema since the last follow-up. AD at age 12 years: dry skin in combination with itchy rash and typical localization the year before follow-up and/or doctor’s diagnosis of eczema since the age of 10 years (16).
Occasional AD. Fulfilling the definition of AD at one or more follow-ups up to the age of 4 years, but not from 4 to 16 years, or vice versa (16).
Persistent AD. Fulfilling the definition of AD at one or more follow-ups up to the age of 4 years and at one or more follow-ups from 4 to 16 years (16).
The study was approved by the Regional Ethics Review Board in Stockholm, Sweden. The principles of the Declaration of Helsinki were followed and all parents gave their written informed consent that their children were allowed to participate.
Groups were compared using Student’s t-test for parametric data and the χ2-test or Fisher’s exact test for non-parametric data. Differences were considered significant at p < 0.05.
A multivariate logistic regression analysis was used to examine a possible correlation between water exposure and sex, dry skin, hand eczema at age 16 years, AD ever, and AD at age 16 years. The logistic regression is presented as odds ratios (ORadj) with 95% confidence intervals (95% CIs). Prior knowledge was used to choose the included variables. Each variable was adjusted for all the other variables in the analysis. Analyses were performed with STATA Statistical Software (release 11.1; Stata Corp, College Station, TX, USA). In Fig. 1 data from a previous study are reproduced (with permission) (10).
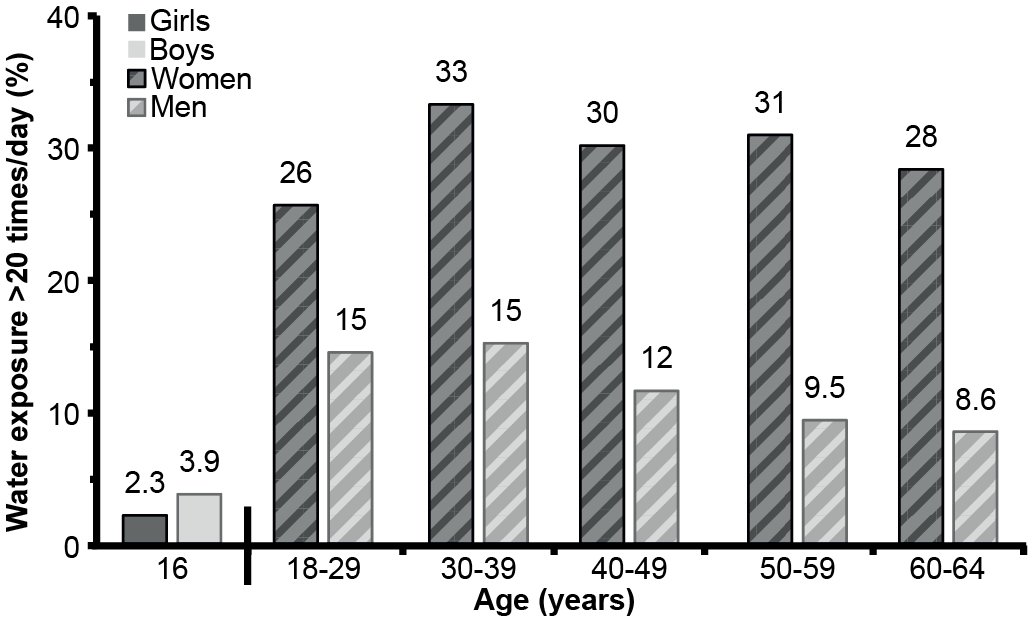
Fig. 1. Self-reported skin water exposure on the hands > 20 times/day. Data for girls and boys, age 16 years, from the present study, and previous data on adults from the Swedish National Environmental Health Survey 2007 (10, with permission).
Low exposure to water on the skin (0–10 times/day) was reported by 71.4%, exposure > 10 times/day by 28.7% and > 20 times/day by 3.1%. Boys reported somewhat higher exposure than girls (p = 0.03) (Table I).
Table I. Self-reported skin water exposure on the hands at age 16 years in relation to sex, dry skin, hand eczema, and atopic dermatitis (AD)
Dry skin during the past 12 months was reported by 1,202 individuals (39%) and they reported more frequent exposure to water than those who did not report having dry skin (p < 0.001) (Table I). Water exposure in girls and boys with dry skin did not differ significantly (p = 0.07). Of those who reported dry skin, 60% fulfilled the criteria of AD ever.
Water exposure in relation to occurrence of hand eczema at age 16 years (1-year period prevalence) is shown in Table I. No statistically significant difference was found in water exposure between those with and without hand eczema (p = 0.1), or between girls and boys with hand eczema (p = 0.9) (data not shown). Analysing water exposure in relation to hand eczema ever (lifetime prevalence) did not reveal any significant differences (p = 0.3) (data not shown).
Water exposure in relation to AD is presented in Table I. Results for the variables AD ever, AD at age 16 years, occasional AD and persistent AD are presented. When comparing with the reports given by those with no AD, no statistically significant differences were found. There were also no significant exposure differences between girls and boys in relation to AD (data not shown).
Logistic regression analysis was used to analyse water exposure in relation to sex, dry skin, hand eczema at age 16 years, AD ever, and AD at age 16 years (Table II). Water exposure ≤ 10 times/day was used as reference, and exposure > 10 times/day as dependent variable. Dry skin gave a significantly increased ORadj 1.4 (95% CI 1.2–1.7).
Table II. Results of a multivariate logistic regression analysis on reported daily water exposure at age 16 years
The adolescents in this large population-based birth cohort reported a fairly low level of water exposure on the hands in comparison with the results of earlier studies in adults. Boys reported a slightly higher exposure than girls, in contrast to the evident female preponderance reported in adults.
Water exposure at age 16 years is to be regarded as a baseline figure, reported in a period of life with low occupational exposure, as almost all the participating adolescents were still attending school. Most of the adolescents were still living in their parental homes, implying limited domestic wet work duties for many of them, although exceptions may occur.
In Sweden there is a long tradition of epidemiological surveillance, and both occupational and non-occupational skin exposure to water have been investigated in the general population (3, 4, 9, 10). In adults (age 18–64 years) high all-day water exposure on the hands, >20 times/day, was reported by 21.7% (10), compared with 3.1% among the adolescents in the present study. The proportion of individuals with low exposure, ≤ 10 times/day, was 71.4% in the adolescents, in contrast to 41.8% previously reported in adults (10). It is thus apparent that water exposure during adolescence is much lower than that later in life, which is probably largely due to less occupational and domestic exposure.
In the present study, 2.3% of the girls and 3.9% of the boys stated all-day exposure > 20 times/day (Fig. 1). In the previous study in adults, the corresponding figures were 25.7% of the women and 14.6% of the men in the youngest age group, 18–29 years (10). The high extent of water exposure in adults seems to appear rather soon after individuals leave school and is probably due to both domestic and occupational exposure. The large difference between the sexes, with more prominent water exposure in women, is probably related to gender differences in choice of occupation and in exposure patterns outside of work (9, 10). Interestingly, this high level of all-day water exposure in young adult women appears to remain at a similar high level later in life, at least up to age 65 years. In contrast, a decreased exposure after age 40 years has been noted in men (10). A further follow-up of the BAMSE cohort is planned and will provide us with the possibility of assessing whether the “adult exposure pattern” will appear in this cohort.
It has been shown that prolonged water exposure may induce skin irritation (18–20). External factors, such as exposure to skin irritants, e.g. wet exposure, and exposure to contact allergens, are well-known risk factors for hand eczema. The present study did not find any increased occurrence of hand eczema in relation to the reported water exposure; however, this is not expected, as the question used reflects current exposure to water, which might not have influenced the onset of the hand eczema in many of the cases. In addition, few individuals reported a high level of exposure.
In a previous report from the BAMSE project, the incidence of hand eczema was 573/100,000 person years; the same magnitude in adolescents as found previously in adults, but the 1-year period prevalence was lower; 5.2% (15). Female predominance was noted regarding both incidence and prevalence. In the present study, the almost even distribution of water exposure between the sexes indicates that there should be factors other than water exposure that explain the female dominance of hand eczema in adolescence. Of the adolescents with hand eczema 73% had symptoms of AD at some point during follow-up (16).
We did not find any correlation between AD and the reported water exposure, which might have been expected, since reducing exposure to water is common advice given to people with AD. It is likely that many of the participants with AD had not, at this young age, fully considered the importance of reducing skin water exposure on their hands. No written information regarding skin water exposure has been given in connection with previous BAMSE examinations. When considering choice of occupation it is important to be aware of the increased risk of hand eczema for individuals with history of AD (21–24). There is a defect in the skin barrier function related to AD (25), which entails an increased propensity to experience skin irritation.
Logistic regression analysis revealed that dry skin was the only variable significantly related to water exposure on the hands > 10 times/day. A history of dry skin is one of a number of criteria used for AD (26). An interesting observation in the present study is that as many as 40% of those who reported dry skin did not fulfill further criteria of AD ever. The question regarding dry skin is not restricted to the hands, in contrast to the question on water exposure. It is not evident how to interpret the self-reports of dry skin. A tendency to over-report water exposure when having dry skin is a possibility that cannot be ruled out. The concept of dry skin is usually based on subjective reports without generally accepted clinical definitions and the occurrence varies (6–73%) in different publications (27–30). The importance of skin water exposure is highly relevant considering current research regarding the skin barrier, dry skin, filaggrin mutations and eczema (30–32).
This is the first study in which reports on skin water exposure in adolescents have been presented. When collecting self-reported data, validated questions should be used, if possible. A question on occupational exposure to water has been validated previously through observation in adults, resulting in a correlation of 0.680 and 0.521, respectively, regarding frequency of exposure (33, 34). The question used in the present study had a similar wording as the validated question; the only difference was that exposure during the entire day was asked for, not only exposure at work. It might be difficult to perform a validation by observation regarding all-day exposure. The question used for 1-year period prevalence of hand eczema has previously been validated in adults, where it was found that the question gives an underestimation of the true prevalence (sensitivity 53–59%, specificity 96–99%) (35). The cohort design of the BAMSE project, the large population-based sample size and high response rate are all strengths of the present study.
In conclusion, the extent of water exposure on skin of the hands at age 16 years is low and may be considered as baseline exposure during a period of life with limited occupational and domestic duties. At this age, the difference in exposure between the sexes is small, with a somewhat higher exposure in boys than girls.
The study was supported with grants from AFA Insurance, Karolinska Institutet, the Welander-Finsen Foundation, the Swedish Asthma and Allergy Association’s Research Foundation, the Foundation for Health Care Sciences and Allergy Research, the Centre for Allergy Research (CfA), the Stockholm County Council, the Swedish Research Council for Health, Working Life and Welfare, Sweden, and the European Commission’s Seventh Framework 29 Program MeDALL (grant agreement 261357).
The authors thank the adolescents and their parents for participating in the BAMSE cohort, and all the staff involved in the study.


 Click to show fullsize
Click to show fullsize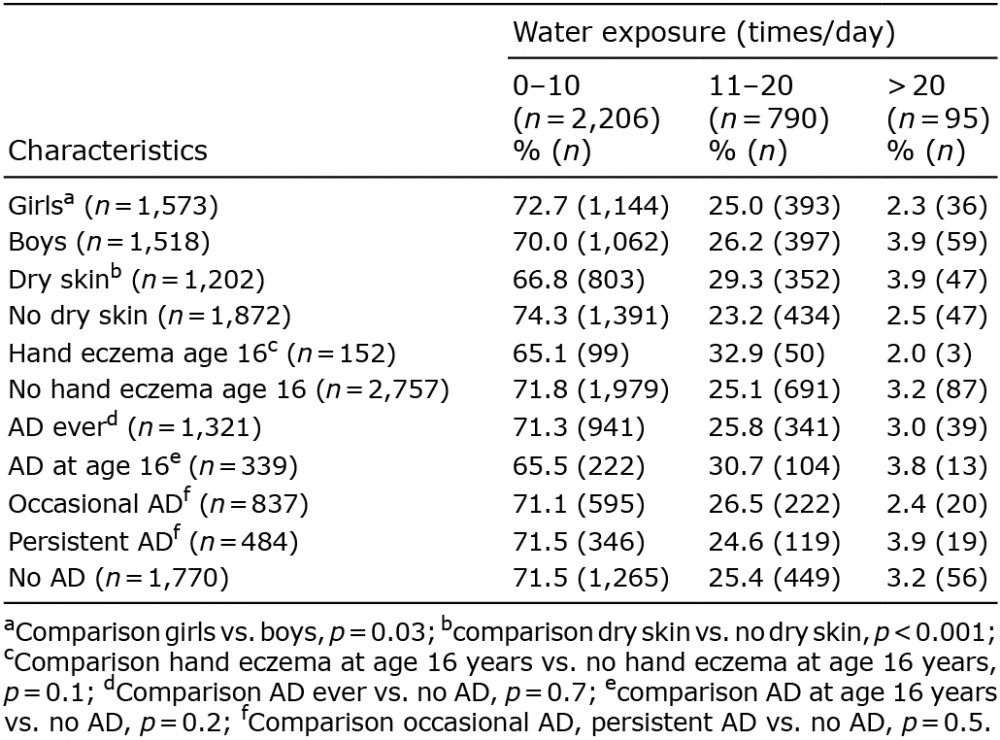 Click to show fullsize
Click to show fullsize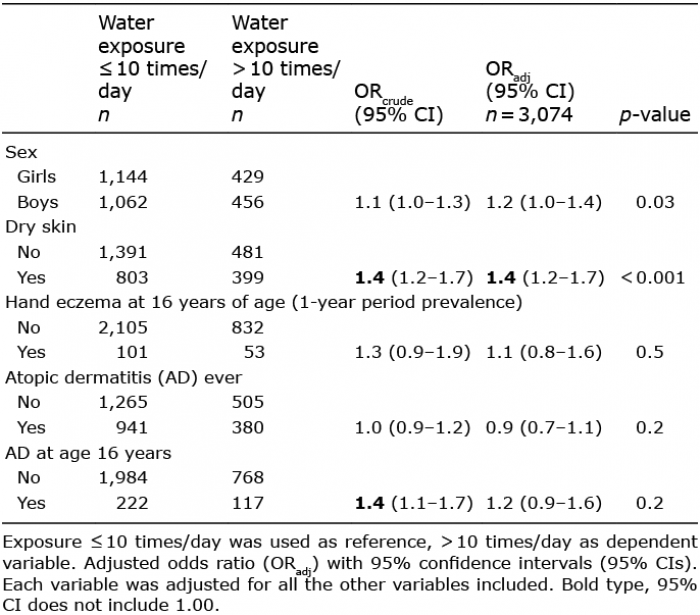 Click to show fullsize
Click to show fullsize