


Departments of 1Dermatology and 2Pediatrics, National Defense Medical College, 3-2 Namiki, Tokorozawa 359-8513, Saitama, and 3Human DNA Analysis Research Group, Kazusa DNA Research Institute, Chiba, Japan. *E-mail: tasaderm@ndmc.ac.jp
Accepted Aug 16, 2016; Epub ahead of print Aug 18, 2016
Molluscum contagiosum is a common viral infection of the skin and a frequent complication of atopic dermatitis. This infection usually occurs in children, and persistent infection up to middle age is rare.
A 55-year-old man presented with generalized eczema and nodules. Physical examination revealed eczematous skin lesions on the face, trunk and extremities, with localized lichenification (Fig. 1A). Poikilodermatous skin changes were observed in the anterior neck and upper chest (Fig. 1B). In addition, numerous whitish dermal nodules 0.5–2 cm in diameter were observed on the trunk and extremities (Fig. 1C, D). Eczema had been noticed since infancy, while dermal nodules appeared at approximately 20 years of age. The patient’s height was 155 cm and his hair was slightly sparse (Fig. 1E), but bamboo-like hair features were not evident. He had protruding ears, scoliosis, hallux valgus, congenital absence of 7 permanent teeth, but no nail changes. His past history included congenital hip dislocation, bronchial asthma during infancy, duodenal ulcer, psychological depression, bilateral ocular retinal detachment and cataract, and recurrent herpetic keratoconjunctivitis. He had no history of recurrent bacterial infections on the skin or in the respiratory tract. Computed tomography revealed no abnormal findings, including thymoma. Histological examination of the eczematous lesions revealed acanthosis with weak spongiosis and dermal lymphocytic infiltration. The whitish nodules were histopathologically diagnosed as molluscum contagiosum (Fig. 1F). We were unable to obtain detailed clinical information for other family members. The results of laboratory tests are shown below and in Table I. The patient showed markedly increased levels of serum IgE (82,362 IU/ml) with specific IgE against house dust (49.3 UA/ml, class 4), Dermatophagoides farinae (50.2 UA/ml, class 5), Japanese cedar (42.7 UA/ml, class 4), Japanese cypress (3.23 UA/ml, class 2), Japanese alder (1.67 UA/ml, class 2), ragweed (3.54 UA/ml, class 3), crab (5.61 UA/ml, class 3), shrimp (3.35 UA/ml, class 2), tuna (1.09 UA/ml, class 2), Candida (57.2 UA/ml, class 5) and Staphylococcus aureus enterotoxin A (5.16 UA/ml, class 3). Serum levels of thymus and activation-regulated chemokine (TARC) (34,050 pg/ml) were also elevated. Serum total IgG was slightly low (737 mg/dl), but IgG antibodies against viruses, such as herpes simplex virus, herpes zoster virus, cytomegalovirus, mumps virus, rubella virus, and measles virus, were produced normally. Lymphocyte proliferative responses to concanavalin A and phytohaemagglutinin were decreased. Negative results were obtained for anti-human immunodeficiency virus antibody and human T-cell leukaemia virus antibody. T-cell receptor excision circles (TREC) and Igκ-deleting recombination excision circles (KREC) analyses (1, 2) were normal, indicating that congenital αβT-cell deficiency and/or B-cell deficiency in primary immunodeficiency diseases (PIDs), such as severe combined immunodeficiency, were unlikely.
Fig. 1. Clinical and histopathological manifestations. (A, B) Eczematous and poikilodermatous skin changes with protruding ears. (C, D) Numerous whitish nodules on the lower limbs. (E) Slightly sparse hair in the occipital region. (F) Whitish nodules histopathologically characterized by downward proliferation of epidermal cells containing eosinophilic Molluscum bodies (haematoxylin and eosin staining; original magnification × 100).
Table I. Results of some immune function tests
Whole-exome sequencing analysis was then performed on an Hiseq1500 platform (Illumina, San Diego, USA) to screen for mutations in the disease genes. No mutations were detected in STAT3, TYK2, DOCK8, or PGM3 genes, indicating that hyper-IgE syndrome (3–5) was unlikely. Further exome analyses revealed the absence of mutations for the following disease genes: SPINK5 (Netherton syndrome), CDSN (peeling skin syndrome), IKBKG (anhidrotic ectodermal dysplasia with immunodeficiency), ERCC2/XPD, ERCC3/XPB, GTF2H5 (IBIDS: ichthyosis, brittle hair, impaired intelligence, decreased fertility, and short stature), GJB2 (KID syndrome: keratitis-ichthyosis-deafness), FALDH (Sjögren-Larsson syndrome), and DKC1 (dyskeratosis congenita). Filaggrin gene mutations specific for Japanese atopic dermatitis patients were not detected (6).
Flow cytometric analysis of peripheral blood revealed low levels of CD8 T cells and γδ T cells, and almost complete absence of HLA-DR (+)/CD11c (+) myeloid dendritic cells and HLA-DR (+)/CD123 (+) plasmacytoid dendritic cells.
This case of molluscum contagiosum was peculiar, not only in terms of the disease duration, but also in terms of the sizes of the individual nodules, which were relatively larger than usual. We initially postulated that the patient had an immune-deficiency syndrome manifesting atopic dermatitis-like features, such as hyper-IgE syndrome and severe combined immunodeficiency. However, these diseases were unlikely, based on the results of genetic and TREC analyses, respectively. Wiskott-Aldrich syndrome, which cannot be screened for by TREC analysis, also shows atopic dermatitis-like skin symptoms, but our patient did not have thrombocytopaenia. The present case showed not only atopic dermatitis-like features, but also several abnormal morphological appearances. Nevertheless, no known diseases seem to match the symptoms of our patient, and these findings were further confirmed by whole-exome sequencing analysis. We are unaware of any similar cases in the literature. We thus have been unable to reach a definitive diagnosis and identify the genes responsible for our patient’s condition.
Flow cytometric analysis showed extremely decreased numbers of CD8 T cells and γδ T cells, and an almost complete absence of myeloid dendritic cells and plasmacytoid dendritic cells. Recently, type I interferon derived from plasmacytoid dendritic cells was shown to play a key role in protective immunity against molluscum contagiosum infection (7). Although the aetiological mechanisms and genes underlying the skin manifestations and immunological abnormalities in our case remain uncertain, persistent molluscum infection could be due to impaired plasmacytoid dendritic cell- and CD8 cell-mediated anti-virus immunity.


 Click to show fullsize
Click to show fullsize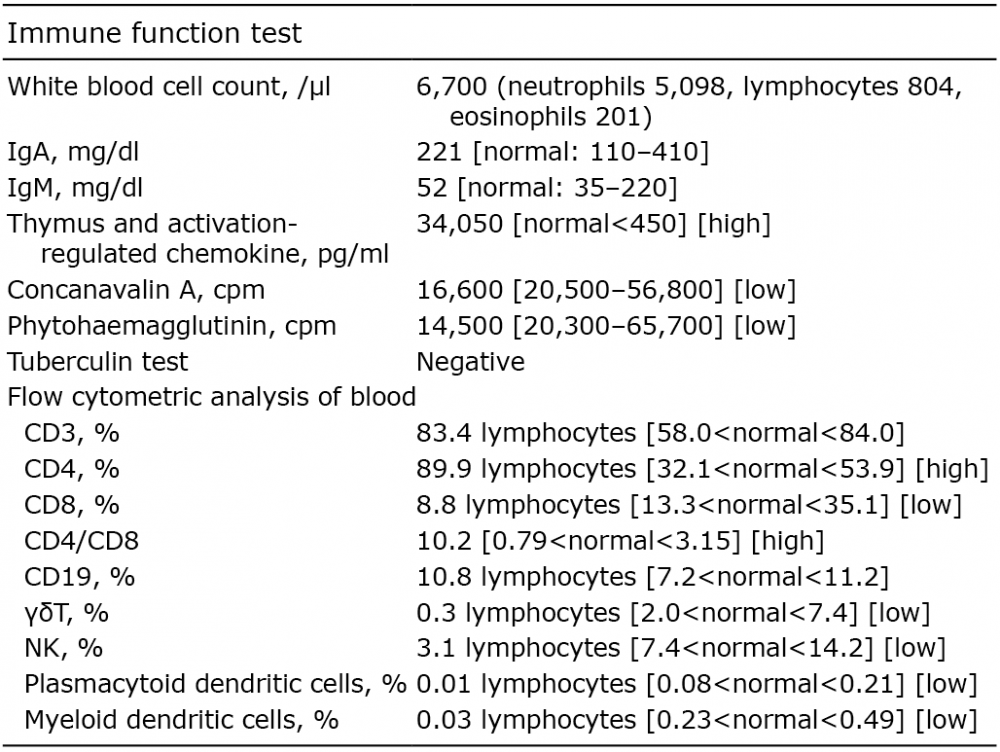 Click to show fullsize
Click to show fullsize