


1Department of Dermatology, and 2Department of Hematology and Oncology, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya 466-8550, Japan. *E-mail makiyama@med.nagoya-u.ac.jp
Accepted Aug 29, 2016; Epub ahead of print Aug 30, 2016
Patients with immunodeficiency are prone to lympho-proliferative disorders. Such conditions are categorized by WHO as “immunodeficiency-associated lymphoproliferative disorders” (1). Furthermore, lymphoproliferative conditions in non-post-transplant patients receiving immunosuppressive therapy are subcategorized as “other iatrogenic immunodeficiency-associated lymphoproliferative disorders” (1). This subcategory comprises a broad spectrum of lymphoproliferative dis-orders, including lymphomas (1, 2). We report here a rare case of extranasal NK/T-cell lymphoma (ENKTL) associated with anti-tumour necrosis factor (anti-TNF) and thiopurine therapy.
Extranodal natural killer/T-cell lymphoma, nasal type (EN-NK/T-NT) is a rare T-cell lymphoma that has strong associations with Epstein-Barr virus (EBV). When EN-NK/T-NT presents at locations other than the upper aerodigestive tract, it is called ENKTL and tends to be highly aggressive (1). In patients with inflammatory bowel disease receiving anti-TNF and thiopurine therapy, the risk of lymphoma has been under constant debate (3–5). The present case suggests that EBV-associated NK/T-cell lymphoma may be a rare, but life-threatening complication in patients who receive anti-TNF and thiopurine therapy.
A 42-year-old woman had been admitted for treatment of a retractable gastric ulcer arising from atypical entero-Behcet’s disease and was referred to our department with tender ery-thema on her legs that had appeared suddenly 3 days earlier. She had a medical history of polymyositis. The patient had been taking prednisolone, 10–20 mg daily, for approximately 5 years. She had been receiving anti-TNF antibody therapy for a total of 3 months; adalimumab was used twice at 80 mg and 160 mg biweekly, and this biologic was later switched to infliximab, 300 mg monthly, for 2 months. In addition, she had been treated with azathioprine, 50 mg daily, for 140 days and with cyclosporine A, 25–100 mg daily, for 110 days. On examination, she was afebrile and her general condition was well. A 4-cm, square, slightly indurated, tender erythema was seen on her left leg. A few 1-cm erythematous eruptions were also seen on her lower extremities. She was prescribed clobetasol propionate ointment. One week later, her erythema enlarged and the induration expanded. Erythema nodosum or Sweet’s disease was suspected, and a skin biopsy was taken from her left leg (Fig. 1A). Two weeks after the initial visit, the erythema became elevated, and multiple subcutaneous nodules appeared on her extremities. An enlarged lymph node was palpable in her left groin.
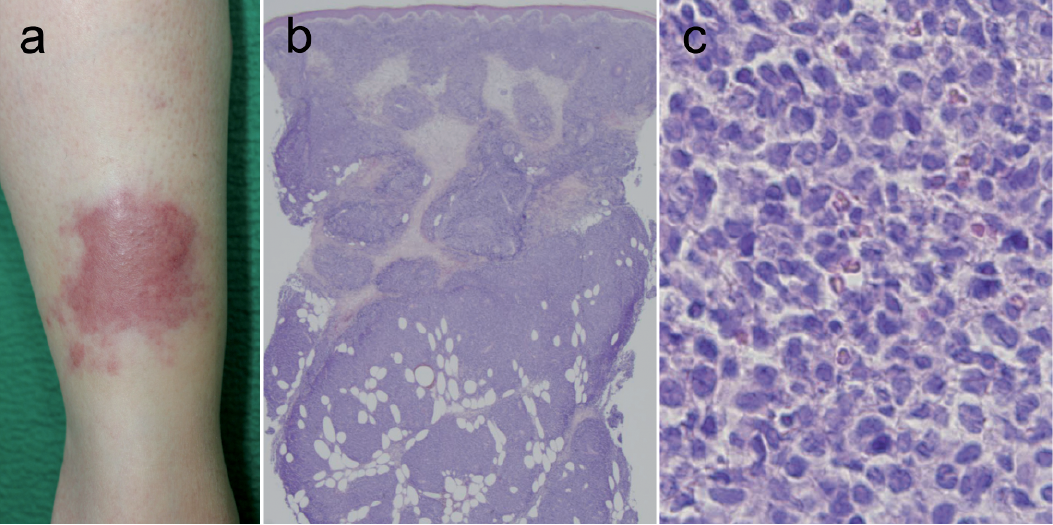
Fig. 1. (A) Patient’s left leg one week after the initial visit. The erythema is tender and mildly indurated. (B) Skin biopsy specimen. At low magnification, dense, lobular infiltration of lymphoid cells is seen in the dermis and the subcutaneous tissue (hematoxylin-eosin (HE) ×20). (C) The infiltrating tumour cells consist of intermediate-sized to large atypical lymphoid cells (HE ×400).
The biopsy specimen revealed dense dermal and subcutaneous infiltration of intermediate-sized to large atypical lymphoid cells (Fig. 1B, C) that were CD3/30+, Granzyme B+/–, EBER-ISH+, CD4/5/8/20/56–, TIA–, Perforin–, TCRβ–, TCRγ–, and TCRδ+/–. Plain computed tomography (CT) and positron emission tomography – computed tomography (PET-CT) scans showed multiple subcutaneous and intramuscular lesions, and left inguinal lymph node swelling. No lesion was found in the upper aerodigestive tract. Bone marrow biopsy found 4% of atypical cells and a few haemophagocytic cells. Her peripheral blood had a high concentration of EBV DNA: 120,725 IU/ml. She was diagnosed with ENKTL. Infliximab was discontinued and an L-asparaginase-based regimen was started, but it was discontinued because of adverse reactions. She died of the disease 4 months after the diagnosis.
Due to the significant immunosuppressive effects of anti-TNF and thiopurine therapy, there have been serious concerns about the increased risk of lymphoma in patients with inflammatory bowel disease (IBD) receiving anti-TNF and thiopurine therapy (3–6). Thiopurines were clearly shown to be associated with increased risk of lymphoma in IBD patients in a prospective observational cohort study (7) and a meta-analysis (8). However, it is somewhat controversial as to whether anti-TNF therapy increases the risk of lymphoma in IBD patients. Some studies have suggested increased lymphoma risk from anti-TNF therapy and others have not (3–5). At least, we can say that the use of anti-TNF with thiopurine, as in the present patient, is thought to be associated with increased risk of lymphoma in patients with IBD (3).
In the present case, the tumour cells were positive for CD3 and negative for CD56. Normal NK cells and most NK cell neoplasms are CD3-negative and CD56-positive. However, EBV-positive NK/T-cell lymphomas showing typical clinical features and morphological characteristics with cytotoxic granule protein expression, as in the present case, can be diagnosed as such even if the tumour cells deviate from the classical immunophenotype, for example, the CD3 positivity and CD56 negativity seen in our case (9, 10). In fact, CD3-positive extranodal cytotoxic lymphomas of true T-cell lineage are a well-recognized subset of extranodal NK/T-cell lymphoma, nasal type and some cases of them are negative for CD56 (9).
NK/T-cell lymphoma is thought to be rare in the subcategory of WHO classification “other iatrogenic immunodeficiency-associated lymphoproliferative disorders.” Nevertheless, we found 2 reports in the English literature of EBV-associated NK/T-cell lymphoma associated with anti-TNF therapy. Deneau et al. (11) reported an 11-year-old boy who had 12 months of infliximab treatment due to IBD of an undetermined type before he was diagnosed with EBV-associated EN-NK/T-NT. Summers et al. (12) reported a 15-year-old white male with atypical IBD and history of suspected hydroa vacciniforme. He had been treated with infliximab for 25 months before he developed painful subcutaneous nodules and plaques that were eventually diagnosed as EBV-associated ENKTL and aggressive-NK-cell lym-phoma overlap. Both patients died within one month after the diagnosis. Interestingly, both patients had a history of periodic fever, aphthous stomatitis, pharyngitis, and adenitis (PFAPA). The present patient had a history of oral aphtha, but none of the other PFAPA symptoms of PFAPA. Notably, shortly before the anti-TNF therapy, she had leukocytosis accompanied by disseminated intravascular coagulation that spontaneously remitted. At the time, however, the lymphoma was not detected by bone marrow biopsy or PET-CT.
The present case and our review of previous reports suggest that EBV-associated NK/T-cell lymphoma may be a rare, but life-threatening complication in patients with atypical IBD who receive anti-TNF therapy. Ery-thematous eruptions or subcutaneous nodules could be the first signs of this rapidly progressing disease. When such symptoms are found, immediate further investigation is recommended.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize