


1Department of Dermatology, Division of Neurosciences, orthopedics and rehabilitation, University Hospital of North Norway, 2Department of Community Medicine, Faculty of Health Sciences, UiT The Arctic University of Norway, Tromsø, Norway, 3Division of Nutritional Sciences, Cornell University, Ithaca, USA, 4Department of Rheumatology, Dermatology and Infectious Diseases, The Olafia Clinic, Oslo University Hospital, 5Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, and 6Department of Microbiology and Infection Control, University Hospital of North Norway, Tromsø, Norway
Overweight is a proposed risk factor for psoriasis. However, evidence from prospective studies is limited. The aim of this study was to investigate the association between overweight, weight gain and risk of psoriasis, and potential synergism with smoking, within a population-based cohort including 8,752 individuals followed from 1994 up to 2008. There was a 32% increased odds of psoriasis from a body mass index (BMI) of 27 kg/m2, in multivariable logistic regression analysis, further increasing to 43% at BMI 28 kg/m2, and to 71% at BMI >30 kg/m2 in non-smokers. There was a dose-response association between weight gain from age 25 years, with up to 90% higher odds of psoriasis from middle age, independent of weight category. There was no indication of a synergism between overweight and smoking, and no interaction with sex. Overweight and weight gain represent modifiable risk factors that may be targets for primary prevention of psoriasis.
Key words: cohort; longitudinal; obesity; overweight; psoriasis; smoking.
Accepted Sep 7, 2016; Epub ahead of print Sep 7, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Anne-Sofie Furberg, Department of Community Medicine, Faculty of Health Sciences, UiT The Arctic University of Norway, NO-9037 Tromsø, Norway. E-mail: anne-sofie.furberg@uit.no
Psoriasis is a chronic inflammatory skin disease that is associated with substantial morbidity as well as several comorbid conditions, including diabetes and cardiovascular disease (1–5). Studies from different populations, including a recent report from Norway (6–9), suggest that the prevalence of psoriasis may have doubled over recent decades, now reaching a lifetime prevalence of 5.8–11% in Scandinavia (6, 8, 10). Psoriasis is a multifactorial disease developing in genetically susceptible individuals. However, the understanding of how lifestyle influences psoriasis risk remains limited (11). Overweight and obesity constitute a major lifestyle epidemic. Numerous cross-sectional and case-control studies have reported positive associations between overweight, obesity and psoriasis (12–14). However, only 3 longitudinal studies have investigated whether overweight predates psoriasis in adults. In a nested case-control study from the UK, overweight individuals had only a slightly increased risk of psoriasis (15), whereas data from a US cohort of women demonstrated a stronger association with overweight and a close to three-fold increased risk of psoriasis if severely obese (16, 17). Also, the cohort displayed increasing risk of psoriasis according to adult weight gain (16). To our knowledge, the long-term effect of weight gain on psoriasis risk has not been investigated in men. There are indications that there could be a difference in the aetiology of psoriasis of the late-onset (onset after age 40–50 years) vs. early-onset type, and it is hypothesized that late-onset psoriasis may be more related to modifiable environmental factors (i.e. overweight); however, the results are not conclusive (16, 18–20). Smoking is an established risk factor for psoriasis (21). A multiplicative effect of obesity and tobacco use was suggested in an Italian case-control study (22), but so far this possible synergism has not been investigated using prospective data.
Longitudinal investigations that may reveal possible relationships between changes in lifestyle factors and the observed doubling of psoriasis prevalence are needed (6). Thus, the primary aim of this study was to investigate the association between overweight, weight gain and the risk of psoriasis within a longitudinal population-based cohort; also considering variations according to sex and age, as well as potential synergism between overweight and smoking.
Data for the present analysis were generated from the multi-purpose population-based Tromsø Study, which includes 6 repeated health surveys (T1–T6) in the period 1974 to 2008; the design and cohort profile have been described in detail elsewhere (23, 24). Whole birth cohorts and random samples of the population in the municipality of Tromsø, Norway, 69°N, were invited based on the official population registry.
In the current prospective analysis of overweight and weight gain in relation to risk of psoriasis, T4 (1994 to 1995) was used as baseline and self-reported psoriasis status in follow-up surveys T5 (2001) or T6 (2007 to 2008) was used as outcome variable. In T4, all subjects born earlier than 1970 were invited, and 77% attended (23). A total of 26,957 participants with valid consent were available for the analysis. In this cohort, data on psoriasis status in T5 (7-year follow-up) and/or T6 (13-year follow-up) was available for 11,328 individuals. Further exclusion criteria were applied using baseline data in T4: age >70 years (n=547); missing data on self-reported psoriasis (n=1,106); self-reported psoriasis diagnosis (prevalent disease) (n=739); being pregnant (n=100); missing measured body mass index (BMI) (n=7); and missing smoking status T4 (n=8) or smoking only cigars and pipe (n=69). A total of 8,752 individuals aged 25–69 years were included in the analysis, with baseline BMI as main predictor. In the analysis of gain in BMI and weight from age 25 years, 26 individuals with age <?26 years at baseline were excluded to ensure that they did not have psoriasis within one year of study enrollment (i.e. reverse causation), and a further 384 individuals were excluded due to missing report of weight at 25 years, giving a study sample of 8,342 individuals. 26 years at baseline were excluded to ensure that they did not have psoriasis within one year of study enrollment (i.e. reverse causation), and a further 384 individuals were excluded due to missing report of weight at 25 years, giving a study sample of 8,342 individuals.
Clinical measurements. Trained health professionals made all clinical measurements according to standardized procedures (23, 24). Height (cm) and weight (kg) were measured with participants wearing light clothes and no shoes. Body mass index (BMI) was calculated as weight divided by height squared (kg/m2). In T4, blood pressure was recorded 3 times in a sitting position after 2 min rest, by an automatic blood pressure measurement device (Dinamap Vital Signs Monitor 1846, Critikon, GE Healthcare, Norway), and the mean of the 2 last readings was used. Non-fasting blood samples were collected from an antecubital vein and analysed at the accredited Department of Laboratory Medicine, University Hospital of North Norway, Tromsø, Norway (24). Serum total cholesterol and triglyceride analyses were performed by enzymatic colorimetric methods with commercial kits (CHOD-PAP for cholesterol and GPO-PAP for triglycerides; Boehringer–Mannheim, Mannheim, Germany). Serum high-density lipoprotein (HDL) cholesterol was measured after the precipitation of lower density lipoprotein with heparin and manganese chloride.
In T5 and T6, participants were asked; “Estimate your body weight when you were 25 years old (in kg)”. The first survey with available data was chosen. For validation purposes, we assessed the correlation between self-reported and measured weight among 532 women and 368 men who recalled their weight at age 25 years in T5 or T6 and had their actual weight at age 24–26 years measured in one of the former surveys, T2–T4. Pearson correlation coefficient (R) was 0.89 (women, R=0.80; men, R=0.79). Self-reported weight at age 25 years and measured height in T4 was used to estimate BMI at age 25 years, and adult change in weight and BMI was estimated as the difference from age 25 years until participation in the baseline survey, T4.
Questionnaire data – psoriasis and lifestyle variables. In all surveys, participants received an invitation letter, and a first questionnaire was enclosed with the invitation, while a second questionnaire was handed out at the screening centre. The second questionnaire was to be returned either at the survey site or through the post, and approximately 90–96% of attendees did so (23, 24). The questionnaires are available in English and Norwegian at the Tromsø study homepage (www.tromsostudy.com).
Life-time self-reported psoriasis was assessed in the second questionnaire using the following question; “Do you have or have you had psoriasis? (yes/no)” (T4 and T5), and “Do you have or have you ever had psoriasis? (yes/no)” (T6). From T6 the question; “Have you ever been diagnosed with psoriasis by a physician?” was added for validation purposes.
In the baseline survey, T4, participants indicated whether they were current daily smokers of cigarettes, cigars or pipe, and their smoking history including previous daily smoking, years since stopped smoking, total number of smoke-years, and mean daily number of cigarettes or weekly number of tobacco packs. Information on alcohol intake included number of units of wine, beer and spirits consumed within a representative 2-week period. Participants indicated their usual level of recreational physical activity as the mean weekly number of hours (0, <1, 1–2, 3+ h) spent doing light activities (not sweating or out of breath) and hard activities (sweating/out of breath) separately.
Due to the known differences in body weight distribution as well as smoking patterns between men and women, most analyses were presented both combined and stratified by sex. Descriptive characteristics at baseline (T4) were reported with means (standard deviation; SD) for continuous variables and numbers (proportions) for categorical variables within 2 BMI categories; BMI 28 and 28 kg/m2. BMI of 28 kg/m2 has been identified as an optimal cut-off value in assessing type 2 diabetes risk in Caucasians (25). p-values for differences between the categories of BMI were assessed using Student’s t-test for continuous variables and ?2 tests for categorical variables.
Smoking status was analysed as a categorical (never, past or current smoking) and as a dichotomous variable (never or past vs. current smokers), while pack-years smoked was analysed as a continuous variable (number of cigarettes per day×number of years smoked/20) and as a categorical variable (0, 1–9, 10–19, 20+ pack years). Education was dichotomized into high educational level (above high-school/A-level) vs. others. The physical activity score was calculated as the sum of hours of light and heavy physical activity in spare time per week, with heavy physical activity given double weighting (26). Mean daily (g/day) intake of alcohol was computed from the number of units of intake of wine (16.6 g/unit), beer (11.7 g/unit) and spirits (7.4 g/unit) within a representative 2-week period.
Incidence proportions of psoriasis were calculated as the number of incident cases in T5 and T6 divided by the total population without psoriasis at baseline. BMI at baseline was assessed both as a continuous, dichotomous, and categorical variable (modified according to WHO, where the 2 lowest categories 25 kg/m2 were combined) in both age-adjusted and multivariable logistic regression analysis including also sex, current smoking (yes/no), mean daily alcohol intake (g/day), and the recreational physical activity score.
Potential statistical interactions by sex, age and smoking status were explored by testing the significance of multiplicative terms added to the multivariable models. We also investigated “biological interaction” between overweight and smoking, as defined by Rothman (27). Biological interaction between overweight and smoking were analysed using the Synergy index score (27), defined as equal to [odds ratio (OR)11–1]/ [(OR01–1) + (OR10–1)], where OR11 is the OR for psoriasis associated with the exposures combined, whereas OR01 and OR10 are ORs for psoriasis associated with the single exposures (in absence of the other exposure). All ORs are calculated using those non-exposed to each of the single exposures as reference category. Thus, the Synergy index score indicates if the risk in double-exposed is higher than expected based on the assumption of an additive effect exerted by the single exposures. A score exceeding 1.0 indicates interaction and a score below 1.0 indicates an antagonistic effect.
All p-values were 2-sided using a 5% significance level. The analyses were performed with SAS 9.2 (SAS Institute Inc., Cary, NC, USA) and SPSS 21 (SPSS Inc., Chicago, IL, USA).
Each participant gave written informed consent prior to the examinations. The study was approved by the Norwegian Data Protection Authority and the Regional Committee for Medical and Health Research Ethics, North Norway.
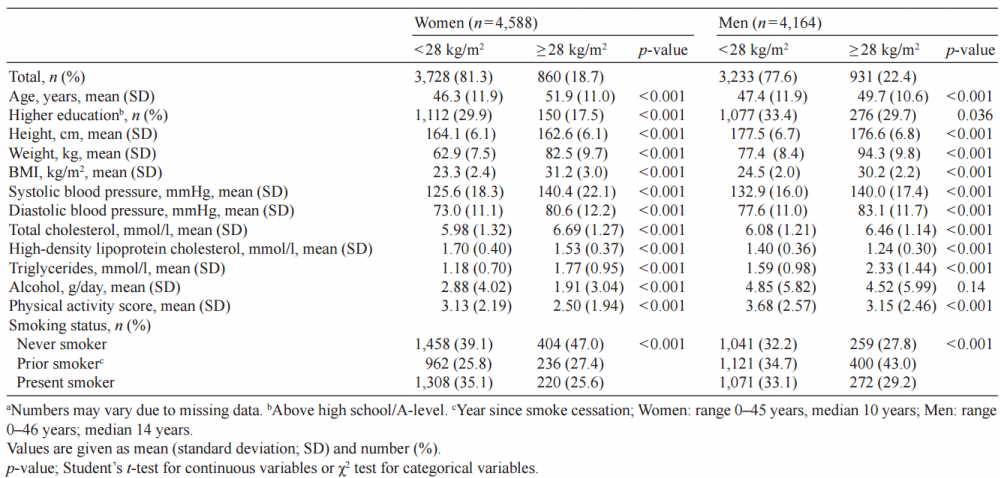
The distribution of all baseline characteristics, except alcohol intake in men, varied significantly across the BMI categories (Table I). Compared with individuals with BMI below 28 kg/m2 those with more overweight were older, had higher blood pressure, more abnormal lipid profiles, lower level of education, smoked less and were less physically active. In women, more overweight and obesity was associated with lower alcohol consumption.
Table I. Baseline characteristics according to body mass index (BMI, kg/m2) for women and men in Tromsø 4; n=8,752a
The incidence proportion of psoriasis during 7–13 years of follow-up was 4.7% in both women and men. We found a statistically significant relationship between BMI and risk of psoriasis for both sexes combined. For each 2.5 unit increase in BMI the odds for psoriasis increased by 8% (multivariable adjusted model, OR 1.08, 95% confidence interval (95% CI): 1.01, 1.16) (Table II). In multivariable analysis using WHO definitions of overweight (25–<30 kg/m2) and obesity (>30 kg/m2), obese women tended to have an increased risk of psoriasis compared with normal weight (BMI 25 kg/m2) women (OR 1.48, 95% CI: 0.94, 2.31), while for women and men combined the association was slightly attenuated. As there was no increase in risk of psoriasis associated with overweight when starting from BMI 25 kg/m2 in our data, we searched for a possible threshold at each higher level of BMI (per kg/m2). There was an association from BMI 27 kg/m2 in the total population (BMI above vs. below 27 kg/m2; multivariable model, OR 1.32, 95% CI: 1.06, 1.64), with a borderline significant association in women (OR 1.36, 95% CI: 0.99, 1.88). For both sexes combined, BMI above vs. below 28 kg/m2 was associated with a 43% increase in the risk of psoriasis (multivariable model, OR 1.43, 95% CI: 1.13, 1.81), and a similar association was seen in both women and men separately, with no age and sex interactions. When stratifying by smoking status to separate the effect of BMI and smoke, strengthening of the association between overweight and obesity and risk of psoriasis was observed in non-smokers; with BMI >30 kg/m2 OR was 1.71 (95% CI: 1.13, 2.56) for both sexes combined (P for interaction 0.14; Table SI). 30 kg/m2) and obesity (30 kg/m2), obese women tended to have an increased risk of psoriasis compared with normal weight (BMI < 25 kg/m2) women (OR 1.48, 95% CI: 0.94, 2.31), while for women and men combined the association was slightly attenuated. As there was no increase in risk of psoriasis associated with overweight when starting from BMI 25 kg/m2 in our data, we searched for a possible threshold at each higher level of BMI (per kg/m2). There was an association from BMI 27 kg/m2 in the total population (BMI above vs. below 27 kg/m2; multivariable model, OR 1.32, 95% CI: 1.06, 1.64), with a borderline significant association in women (OR 1.36, 95% CI: 0.99, 1.88). For both sexes combined, BMI above vs. below 28 kg/m2 was associated with a 43% increase in the risk of psoriasis (multivariable model, OR 1.43, 95% CI: 1.13, 1.81), and a similar association was seen in both women and men separately, with no age and sex interactions. When stratifying by smoking status to separate the effect of BMI and smoke, strengthening of the association between overweight and obesity and risk of psoriasis was observed in non-smokers; with BMI 30 kg/m2 OR was 1.71 (95% CI: 1.13, 2.56) for both sexes combined (P for interaction 0.14; Table SI1).
Table II. Incidence proportion (IP) and odds ratio (OR) for psoriasis by body mass index (BMI, kg/m2) at baseline. Tromsø 5 (2001) or Tromsø 6 (2007–2008) vs. Tromsø 4 (1994–1995). n = 8,752 in age-adjusted model and n = 8,387 in multivariable model
There was a dose-response relationship between BMI gain from age 25 years to baseline (T4) and psoriasis incidence in the age group 45 years and older at baseline (p for linear trend over quartiles=0.009), with an up to 70% increased odds in the top quartile compared with the bottom quartile (multivariable model, OR 1.70, 95% CI: 1.13, 2.55), while in the younger age group there was no association (p for interaction=0.03) (Table III). For both sexes and age groups bottom quartile equalled a less than 2 unit increase in BMI from age 25 years up to the baseline survey. Cut-offs for quartiles of BMI change within 5-years age groups are shown in Fig. S1. When using adult weight gain (weight change from age 25 years to baseline) as main predictor in the models, the association with risk of psoriasis was further strengthened from age 45 years, OR 1.90 (top vs. bottom quartile 95% CI 1.28, 2.82), p-trend=0.002, p for interaction=0.02. There were no statistically significant interactions with sex or smoking status. Sensitivity analysis limited to those with 13 years’ follow-up (T6) gave almost the same risk estimates, as did the inclusion of observations with missing psoriasis data in the baseline population.
Table III. Incidence proportion (IP) and odds ratio (OR) for psoriasis by change in body mass index (BMI, kg/m2) from age 25 years to baseline. Tromsø 5 (2001) or Tromsø 6 (2007 to 2008) vs. Tromsø 4 (1994 to 1995); n = 8,342 in age-adjusted model and n = 7,997 in multivariable model
Smokers presented with almost doubled incidence proportions of psoriasis compared with non-smokers; 6.7% vs. 3.7%, as also reflected in the 1.70–2.16-times increased odds for psoriasis in smokers estimated from the multivariable analysis (Table SII1). There was a significant dose-response relationship between pack-years smoked and risk of psoriasis in women (p <0.003) and for both sexes combined (p < 0.001). In multivariable analysis of combined exposure to overweight/obesity and smoking, there was no indication of a multiplicative association and biological interaction using SI-scores (Table II). The simultaneous exposure to smoking and overweight ?BMI 28 kg/m2 gave the highest incidence proportions of psoriasis, with 7.7 and 7.4% in women and men, respectively, vs. 3.1% and 3.5% in those not exposed to either, multivariable adjusted OR 2.48 (95% CI: 1.70, 3.63). Redefining those stopping smoking within the last 12 months before baseline as current smokers, did not influence the results.
The results of this large prospective study indicate that above a threshold of BMI 27–28 kg/m2 both women and men display more than 40% increased risk of psoriasis, which was further increased in obese non-smokers reaching 70%. Adult gain in BMI or weight was associated with a 70–90% increased risk of late-onset psoriasis for both sexes, independent of BMI or weight category. Smoking almost doubled the risk of psoriasis; however, there was no indication of a synergism between overweight and smoking on the risk of psoriasis.
There are both strengths and limitations to this study. Firstly, the selection of participants from a large population-based cohort with high attendance rates in repeated health surveys generally allows for a more truthful evaluation of the relationship between overweight, weight gain, smoking and risk of psoriasis. Also, the data include comprehensive assessment of lifestyle factors and clinical examinations using standardized and validated methods (24). Selection bias is usually more limited in general health surveys. Studies within the Tromsø study cohort indicate that there is a chance that obese individuals and smokers may be slightly under-represented in the cohort (6, 23, 24). The subjects who have declined participation tend to be younger or very old, male and single (23, 24).
Self-report of psoriasis is a widely used method in epidemiological studies (2, 6, 10, 28, 29). Approximately 90% of psoriasis cases are classical plaque phenotypes (30), which according to validation studies from comparable populations, are adequately diagnosed by trained general practitioners (31–33), who attend to the majority of patients with psoriasis in Norway. Among those with self-reported psoriasis in T6, approximately 90% of women and 84% of men confirmed a doctor’s diagnosis (6), and the reproducibility of self-reported psoriasis between the first 4 surveys and T6 was high (6). A recent Norwegian study from a similar cohort showed that self-report of psoriasis was a valid method with a positive predictive value (PPV) of 78% (10). Due to the relatively low sensitivity (i.e. high number of false negatives) the estimated true prevalence of psoriasis was 8% vs. 5.8% as reported in the cohort (10, 34). Data from the US Nurses’ Health Study showed that 92% of reported psoriasis cases were definite cases of psoriasis (17). Also, prior studies suggest that up to half of mild psoriasis cases may go undiagnosed by a doctor (28, 35, 36), which could potentially attenuate the effect estimates.
In line with others, we also found that persons with skin disease tend to not seek medical attention (28, 37–39), and that there may be a sex difference in the degree that they seek medical consultation (6, 37). The validity of self-reported prior weight was acceptable in a former US study (40). This is in line with data in the Tromsø study. Prior studies from the Norwegian population have also shown acceptable validity of self-reported smoking (41–43).
The approximate 6-year time laps between the surveys gives some uncertainty as to when in the time period their psoriasis, BMI or smoking status may have changed. However, the degree of tracking in weight is high in the Tromsø cohort (44). In general, women have become overweight in the time period after the baseline survey in 1994 to 1995 (6). Thus, the association between change in BMI and incident psoriasis in women might be more difficult to disentangle in our data. An earlier study supported that short-term weight gain does not seem to be an important risk factor for incident psoriasis (45). Ideally, we would have had more detailed information on body composition, including abdominal adiposity (e.g. waist circumference), at baseline.
It is possible that the association of BMI with incident psoriasis could be confounded or modified by other factors. There may be residual confounding from factors either unknown or not included in our analysis, for example genetic susceptibility. A possible confounder is dietary composition, including high salt intake, which has been associated both with diets composed of highly processed foods and with autoimmune disease (46, 47). Tromsø has subarctic climate conditions with more than 5 months of negligible ultraviolet radiation exposure, making inhabitants vulnerable to vitamin D deficiency. Vitamin D has been inversely linked to severity of psoriasis (48). As increasing BMI leads to decreased levels of circulating vitamin D, it is possible that the obesity epidemic may be especially important to health in the Tromsø cohort (48).
Our results are in line with findings from comparable studies showing a relationship between overweight, obesity and incident psoriasis (15–17). In the women in the US Nurses’ Health Study, increasing risk of psoriasis within increasing BMI categories was reported, with relative risk (RR) 1.40 in the overweight, 1.48 in the obese, and 2.69 in the severely obese category (16), as further supported by a later study (17). A study including both sexes from the UK General Practice Research Database also found that overweight and obesity represent risk factors for psoriasis, with an 11% and 33% increase in odds, respectively (15). Also, in a recent nationwide Danish study, diagnosis of gall stone as a proxy for obesity was associated with an 18% higher odds of psoriasis using a cross-sectional analysis and a 10% increased risk of psoriasis when using a prospective design (49). Our stratified analysis of smoking status, performed in order to further adjust for tobacco as a confounder, allowed us to demonstrate a 70% increased odds of psoriasis among obese individuals. Even though a linear association was observed between BMI and odds of psoriasis, data show that this was explained merely by the increased risk above the found threshold. We did not have a sufficient number of severely obese cases to further investigate this association.
To our knowledge this is the first prospective study investigating weight gain as a risk factor for psoriasis onset in men; belonging to the upper quartile of BMI or weight gain led to a 70–90% increased odds of psoriasis among persons from middle-age, with a dose-response relationship for both BMI and weight gain. In the US Nurses’ Health Study cohort, the RR of psoriasis in women in the highest weight gain category was up to 1.88, and a positive trend was also observed here (16).
Our results suggest that adult weight gain may be a more important risk factor for psoriasis among late-onset cases, as supported by a recent study in which patients with late-onset psoriasis had a higher proportion of obesity and elevated waist circumference than the early-onset group (18). Setty et al. did not report any interaction between age and overweight as a risk factor for psoriasis (16). However, the investigated women were mainly more representative of the late-onset psoriasis group. Furthermore, as the obesity epidemic in the US is more established, their mean BMI may have already been increased at a younger age. The association between BMI and late-onset cases could be due to the prolonged and cumulative negatively influencing inflammation due to overweight/obesity, which can no longer be compensated for by the individual. Moreover, it can be related to interactions with weakly predisposing genetic or epigenetic factors.
Smoking was a strong risk factor for psoriasis in our data, as also indicated by others (22, 50, 51). A US cohort study found current smoking to be a strong predictor of psoriasis development, with a dose-dependent increasing risk between 1.8 and 2.7 (521). Although there was no statistically significant sex interaction in our data, smoking seemed to be a stronger risk factor for psoriasis among women, demonstrating dose-dependency between pack-years smoked and odds of psoriasis, as also indicated by others (22, 50). While a multiplicative effect of overweight and smoking was suggested in an Italian case-control study (22), this synergism could not be confirmed by our data. However, in our cohort, overweight smokers had the highest incidence of psoriasis, suggesting an additive effect.
Our findings are supported by known biological mechanisms. Obesity is in itself characterized by low-level inflammation (53), and basic research indicates that adipocytes and activated inflammatory macrophages can play a role in both psoriasis and overweight/obesity (13). Adipose tissue produces several hormones, adipokines, and pro-inflammatory cytokines important in psoriasis, among these interleukin (IL)-1, IL-6 and tumour necrosis factor alpha (TNF-α) (13, 54–57). Increased production of pro-inflammatory cytokines is also seen in chronic smoking due to oxidative stress and effects on both the innate and adaptive immune system (51, 58–60). Thus, it is biologically plausible that overweight and smoking may fuel the development of psoriasis in genetically predisposed individuals (54).
There may be shared genetic variants that increase susceptibility to both obesity and psoriasis (61). However, in a meta-analysis of 4 psoriasis genome wide association study cohorts there was no differences between psoriasis cases and controls in a weighted gene risk score investigating single nucleotide polymorphisms associated with increased BMI (62). Epigenetic mechanisms have recently emerged as a putative link between genetic and environmental factors in psoriasis, meaning that environmental factors can lead to activation or deactivation of specific genes of importance for disease development (63–65).
The longitudinal study design allows us to determine that obesity precedes psoriasis and is a risk factor for psoriasis development. The relatively strong effect estimates, dose-response relationship, biological plausibility, as well as consistency with other studies support that this may be a causal relationship. Overweight and smoking represent modifiable risk factors that may be targets for both primary prevention as well as supportive treatment of psoriasis. Interestingly, 2 recent randomized controlled trials showed clinical improvement of psoriasis through a low-energy diet (66, 67). Furthermore, the association between overweight and psoriasis is of great importance in relation to potential comorbid conditions, as abdominal adiposity is the hallmark component of the metabolic syndrome, a major risk factor for cardiovascular disease and diabetes. More studies investigating the effect of weight loss and smoking cessation on psoriasis severity and treatment response are warranted.
The authors wish to thank all participants and personnel in the Tromsø Study.
KD has been an invited speaker and consultant for Abbott/Abbvie, Janssen, and Galderma. The other authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize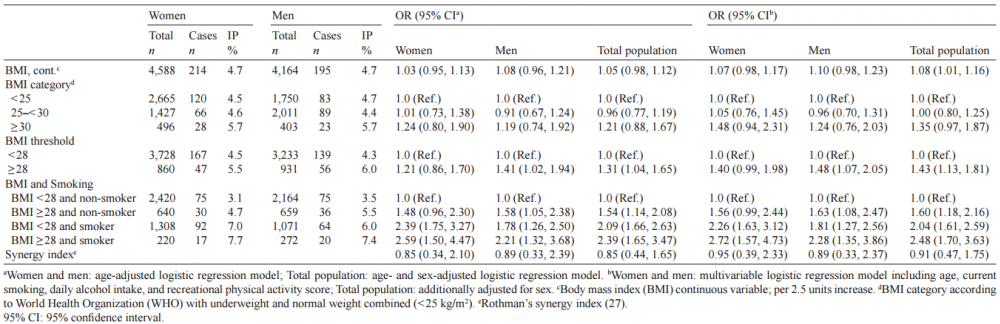 Click to show fullsize
Click to show fullsize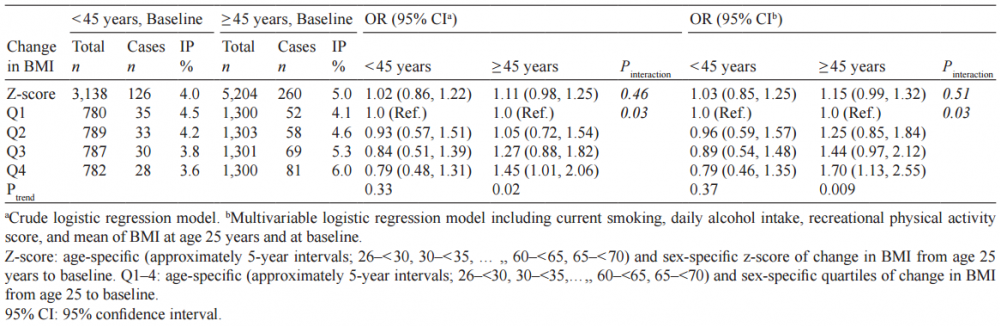 Click to show fullsize
Click to show fullsize