


1Jockey Club School of Public Health and Primary Care, The Chinese University of Hong Kong and the Prince of Wales Hospital, Shatin, Hong Kong, 2Dermatologie, Venerologie und Allergologie, and 5Institut für Infektionsmedizin, Christian-Albrechts-Universität zu Kiel und Universitätsklinikum Schleswig-Holstein, Campus Kiel, Kiel, Germany, 3Histologische Diagnostik, and Department of Dermatology, University Hospital Zürich, Zürich, Switzerland, and 4Department of Dermatology, Godavari Foundation Medical College and Research Center, DUPMCJ, Nashik, India
Eruptive pseudoangiomatosis is a distinct exanthem thought to be caused by viruses. The usual rash configu-ration is erythematous papules and macules. An association with echovirus infection has been reported. We present here one adult and one child with this exan-them, supported by clinical, histopathological, and immunohistochemical findings. Both patients presented with prodromal symptoms, widespread angioma-like macules in annular configuration, blanchable telangiectasia, followed by spontaneous remission in 6–8 weeks. Lesional histopathology of the adult patient revealed dilated dermal blood vessels and lymphohistiocytic infiltrates predominated by CD4+ lymphocytes with a 5:1 ratio of CD4:CD8 lymphocytes. No B cells or CD56+ natural killer cells were found. Serology of both patients revealed evidence of active infections by adenoviruses, and a range of other viruses were excluded. We believe that these 2 patients manifested annular eruptive pseudoangio-matosis, a novel variant of the rash with a probable adenovirus association that has not yet been reported.
Key words: annular rash; cell-medicated immunity; eruptive hypomelanosis; Gianotti–Crosti syndrome; pityriasis rosea; viral infection.
Accepted Oct 3, 2016; Epub ahead of print Oct 4, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Antonio Chuh, Shops 5 and 6, The Imperial Terrace, 356 Queen’s Road West, G/F, Hong Kong. E-mail: antonio.chuh@yahoo.com.hk
Eruptive pseudoangiomatosis (EP) was first described by Cherry et al. in 1969 (1). In 1993, Prose et al. (2) described 3 children with angioma-like papules during viral illnesses. As the skin lesions appeared suddenly, “like an explosion”, it qualifies as eruptive. As the macro-scopic appearance is akin to cherry angiomas, with the histopathological changes not incorporating vascular proliferation, it qualifies as pseudoangiomatosis. EP was thus termed as such by Prose et al. in 1993 (2), some 24 years after the initial description of this exanthem (1).
Owing to its clinical course, with spontaneous remission, infectious causes are suspected. EP is one of several loosely categorized skin diseases known as paraviral exanthems, denoting that the disease is suspected to be related to infectious, usually viral, causes, but without an established single microbe-disease aetiology (3, 4).
The inclusion of diseases in this category is debated, but is generally taken to be pityriasis rosea, pityriasis lichenoides, Gianotti–Crosti syndrome, asymmetric periflexural exanthem/unilateral laterothoracic exanthem, papular-purpuric gloves and socks syndrome, EP, and eruptive hypomelanosis (3–5).
In this family of diseases, EP is probably one of the least common. We present here reports of one adult and one child with eruptions for which the clinical features and laboratory findings strongly substantiated a diagnosis of EP, and suggest a novel aetiology and a novel morphological variant of this exanthema.
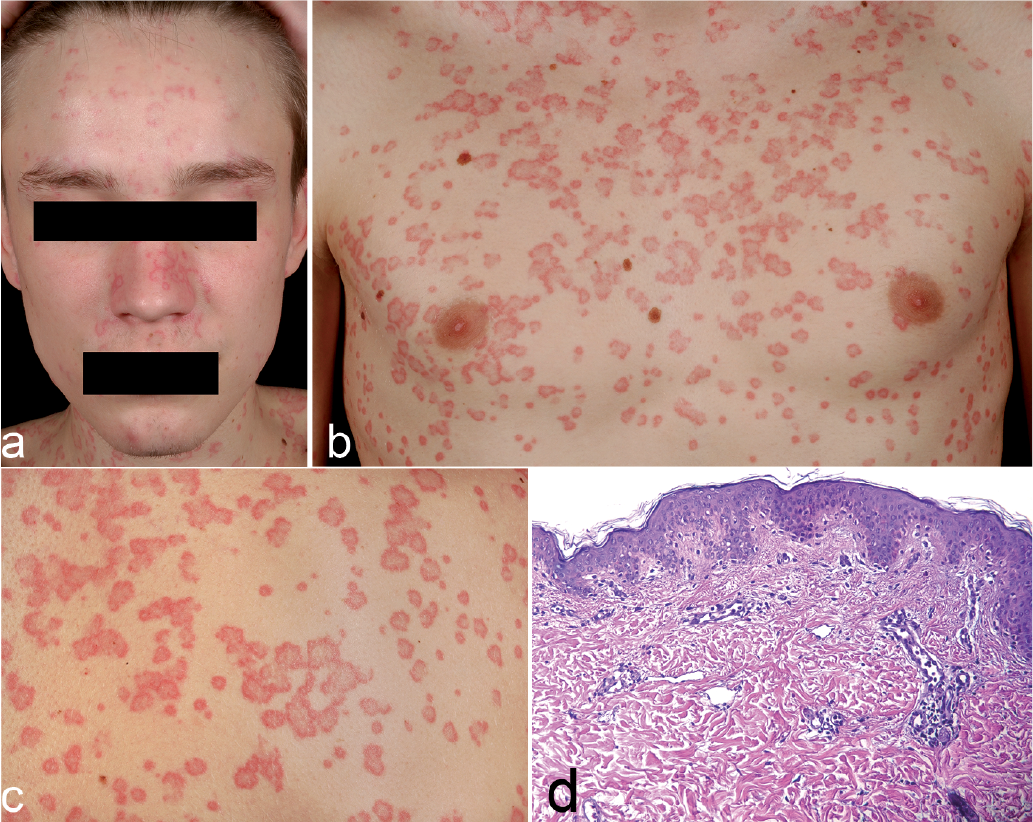
Patient 1. A 19-year-old male presented with a 2-day history of a mildly pruritic skin rash, characterized by annular erythema with dark-red plaques. Some of the annular lesions were closed, while others were open-ended (arcs). The lesions were identifiable as blanchable telangiectasia on the trunk, arms and face (Fig. 1a–c). The patient had diarrhoea, which started one week before onset of the rash.
Fig. 1. Patient 1. (a) Annular erythematous plaques on the face (b) Multiple flat annular erythematous plaques on the trunk of patient 1. Some of the annular lesions were closed, while others were open-ended as arcs. (c) Telangiectasia on the edge of the annular plaques noted on closer view 1. Diascopy confirmed blanchability. (d) Lesional histopathological examination revealed slightly ectatic vessels in the upper dermis with prominent hobnail-like endothelia, accompanied by a sparse lymphocytic infiltrate. (haematoxylin and eosin stain, ×200). Permission is given to publish these photos.
A lesional skin biopsy was performed for histopatho-logical and immunohistochemical analyses (Fig. 1d). Beneath an epidermis with focally increased basal pigmentation, there were slightly ectatic capillary vessels with prominent hobnail-like endothelia, and perivascular lympho-histiocytic infiltrates with admixture of melanophages. Immunohistochemical staining showed predominantly CD4+ lymphocytes with a ratio of CD4:CD8 lymphocytes of approximately 5:1. There was no admixture of B cells, CD56+ natural killer cells, or natural killer T cells. In addition, CD123+ plasmacytoid dendritic cells were absent.
Serological investigations on the active serum revealed elevated titres of IgG and IgA against the adenoviruses (IgG: 33.6 U/ml, reference: < 14 U/ml; IgA: 29.8 U/ml, reference: < 11 U/ml). IgM and IgG against capsid antigens of Epstein-Barr virus, and IgG against its nuclear antigens were negative. IgM, IgG and IgA against enteroviruses were also not detectable. Serological findings also excluded active infections with cytomegalovirus, human herpesviruses types 6 and 7, herpes simplex viruses, parainfluenza viruses, hepatitis A virus, hepatitis B virus, and hepatitis C virus. For bacteria and parasites, serological investigations negated infections by Mycoplasma pneumoniae, Treponema pallidum, echinococcus, and plasmodium.
We did not put the patient on active therapy, but followed him weekly. Complete rash resolution was noted 2 months after onset.
Patient 2. A 5-year-old boy in otherwise good health presented with 4-day history of an erythematous maculopapular rash on the face, hands, feet, and retroauricular, gluteal, and genital regions (Fig. 2). Close examination revealed telangiectasia that were blanchable upon digital pressure. Most of the lesions were of annular configuration, with some being completely closed and some being open arcs. No target lesions were seen. His mother reported that he had had pertussis shortly before onset of the rash.
Fig. 2. Patient 2. (a) Erythematous papules and macules on the face. (b) Annular erythematous plaques on the arm of. Permission is given to publish these photos.
Due to the age of the patient and the almost identical rash morphology we had seen some weeks before (in patient 1) we decided not to proceed with an invasive lesional biopsy. The acute serum was found to be positive for IgG and IgA against adenoviruses, substantiating active infection with these viruses. Serological investigations negated active infection with enteroviruses, human herpesvirus type 6, parvovirus B19, Epstein-Barr virus, parainfluenza viruses, and cytomegalovirus.
We did not commence any active intervention. The rash remitted spontaneously one week later, spontaneously reappeared 2 weeks later, and finally completely resolved after a further 2 weeks.
Based on the clinical and histopathological features, we believe that the most appropriate diagnostic label for our 2 patients was EP. For the clinical features, both patients reported a prodrome, which is characteristic of paraviral exanthems. The lesions in EP have been reported as monomorphous erythematous papules of approximately 2–5 mm diameter, on the face, trunk and extremities (6). The telangiectasia would be blanch-able (6). These features were exemplified by our 2 patients. Spontaneous remission with no need for active intervention was displayed by both patients. Lastly, differential diagnoses of EP, including spider angiomas, cherry angiomas, multiple pyogenic granulomas, bacillary angiomatosis, viral or other paraviral exanthema, and drug rash (7), were highly unlikely.
Urticaria multiforme (UM) could be a differential diagnosis for patient 2. However, target lesions in UM with ecchymotic centres, middle rings of pallor and oedema, and outer rings of erythema or blisters (8, 9) were not seen in patient 2. Moreover, individual lesions in UM erupts and remits in less than 24 h, while individual lesions in patient 2 erupted and remitted within weeks. The absence of classical target lesions or iris lesions also rendered erythema multiforme unlikely for both patients.
For the histopathological findings, the lesional histopathological features of EP are generally considered to be non-specific, and cannot solidly confirm an EP diagnosis. However, dilated blood vessels with plump hobnail-shaped endothelial cells have been reported to be quite specific, though not pathognomonic, of EP (6, 10). The number (density under the microscope) of vessels would not be increased, as distinct from this feature in true angiomas (6, 11). Perivascular lymphocytic infiltrates would also be seen.
In the lesional biopsy from patient 1, non-specific histopathological changes, such as perivascular lymphocytic infiltrates, were seen. The fairly specific features of ectatic capillary vessels in the superficial dermis and prominent hobnail-like endothelia were present. No increase was seen in the number or density of the blood vessels. Melanophages were noted in the lymphohistiocytic infiltrates. Melanophages have been reported to be associated with inflammatory diseases and post-inflammatory hyperpigmentation (12). These offer some substantiation for the diagnosis of EP.
For the immunohistochemical findings, the predominance of CD4+ lymphocytes with a CD4:CD8 ratio of approximately 5:1 were compatible with a viral infection. We believe that these clinical and histopathological features support a diagnosis of EP as most appropriate for patient 1.
Our report incorporates novel rash morphology and a novel association with adenovirus infection. For rash morphology, we noted annular configurations of individual lesions for both patients. Previous reports on EP described the lesions as papules (9 patients by Guillot & Dandurand (6), 3 patients by Neri et al. (13); 3 patients by Yang et al. (14); and 32 patients by Kim et al. (15)) or macules (7 patients by Pérez-Barrio et al. (16)). To our best knowledge, annular EP has not been reported previously, and is thus a novel variant of this exanthem. However, we failed to postulate a mechanism for the central clearance in these lesions.
For the virus association, we reported evidence of active adenovirus infections for both patients. The significantly elevated IgA titre against adenoviruses supported the mucosal infection route. It has been reported that patients with acute adenovirus infections, as confirmed by viral DNA detection by PCR and detection of transcripts by reverse-transcriptase PCR, have detectable IgG (17). Detectable IgG against adenoviruses might have been due to previous exposure, and would not exclude currently active infection (18). We postulate that recent adenovirus infections might have provoked specific, mainly cell-mediated, immunological responses in our 2 patients. Such responses could then trigger a final common immunopathogenetic pathway, leading to the eruption of EP.
To our knowledge, an association of adenovirus infection and EP has not been reported previously. It is important to note adenoviruses as potential causes of EP, as these viruses can cause severe complications on their own, such as keratoconjunctivitis, gastroenteritis (19), diarrhoea, cystitis, and lower respiratory tract infections (20). These clinical manifestations and complications could be independent of the apparently harmless and self-limiting cutaneous manifestations such as EP.
EP has also been reported to be associated with hospitalization (6), treatment of cancer (6), and immunosuppression (7, 21), which substantiates infectious causes for EP. However, for our 2 patients, there were no medical history or family history of congenital or acquired immunodeficiencies.
A limitation of our report was that lesional biopsy was not performed on patient 2. We did not collect specimens from multiple body sites for the detection of viral DNA by PCR or transcripts by reverse-transcriptase PCR. More-over, we did not collect convalescent sera to be investigated with the acute sera in parallel for documentation of seroconversions or significant rises in the antibody titres. However, we believe that the present serological results rendered active infection by adenoviruses the most likely cause of the exanthem in the 2 patients reported here.
We have, thus, reported an adult and a child with EP, substantiated by clinical, histopathological, and immunohistochemical features. We have reported annular EP as a novel variant, and adenovirus infection as a novel association, of this paraviral exanthem.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize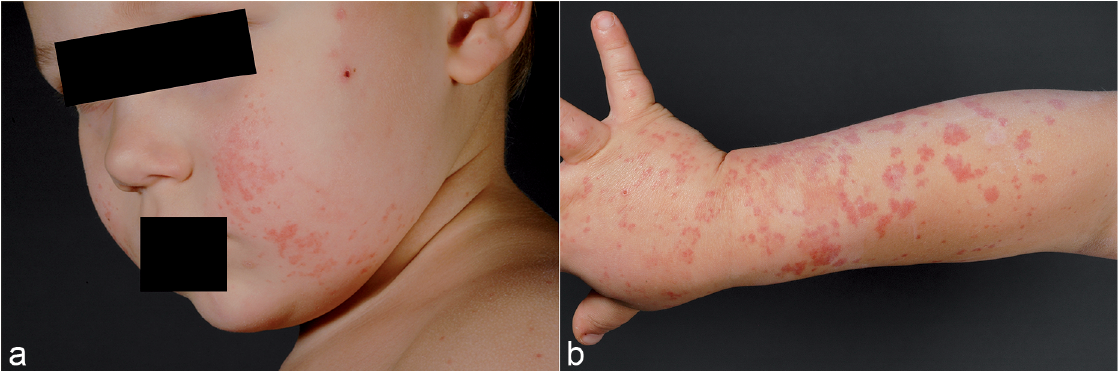 Click to show fullsize
Click to show fullsize