


1Division of Dermatology, Department of Medicine of Sensory and Motor Organs and 2Division of Clinical Laboratory Medicine, Department of Pathophysiological and Therapeutic Science, Tottori University Faculty of Medicine, 86 Nishi-cho, Yonago 683-8504, Japan. *E-mail: sugita@med.tottori-u.ac.jp
Accepted Oct 26, 2016; Epub ahead of print Oct 27, 2016
Adult T-cell leukaemia/lymphoma (ATLL), a malignancy of CD4+ T cells with poor prognosis, is caused by human T-cell lymphotropic virus type 1 (HTLV-1). Based on the organ involvement and severity, ATLL is divided into 4 clinical categories: acute, chronic, lymphoma and smouldering types (1). ATLL neo-plastic cells are usually present with the phenotype of CD4+CD25+CCR4+ cells (2, 3). CCR4 is a 7-transmembrane domain, G-protein-coupled receptor that is specific for the CC chemokines CCL17 and CCL22. Among the various T-cell subsets, CCR4 is also expressed on activated Th2 cells and regulatory T cells (Treg) (4–7). A novel defucosylated humanized anti-CCR4 monoclonal antibody, mogamulizumab, has been approved for treatment of ATLL in Japan (8). Mogamulizumab exerts highly cytotoxic for ATLL cells via antibody-dependent cellular cytotoxicity. Here, we show that vacuolar type of interface dermatitis induced by CD8+ T cells may occur in association with the elevated immunity after mogamulizumab treatment.
An 85-year-old Japanese man with chronic heart failure was diagnosed with acute-type ATLL. Peripheral blood examination showed an elevated leukocyte count of 24,300/μl with 79% abnormal lymphocytes; approxi-mately 94% of the lymphocytes were positive for CD4, CD25 and CCR4. The level of soluble interleukin-2 receptor was 4,811 IU/ml. At that time, he did not report having any skin symptoms. Since there was strong expression of CCR4 on ATLL cells in peripheral blood, he was treated with mogamulizumab. One month after the completion of treatment with 8 doses of mogamulizumab, a skin lesion appeared and he was referred to our department. Prior to the development of the eruption, he had been treated for hypertension, prostatomegaly, arrhythmia, bronchitis, and hypokalaemia with spironolactone, tamsulosin, bisoprolol fumarate, carbocisteine, and potassium chloride, respectively.
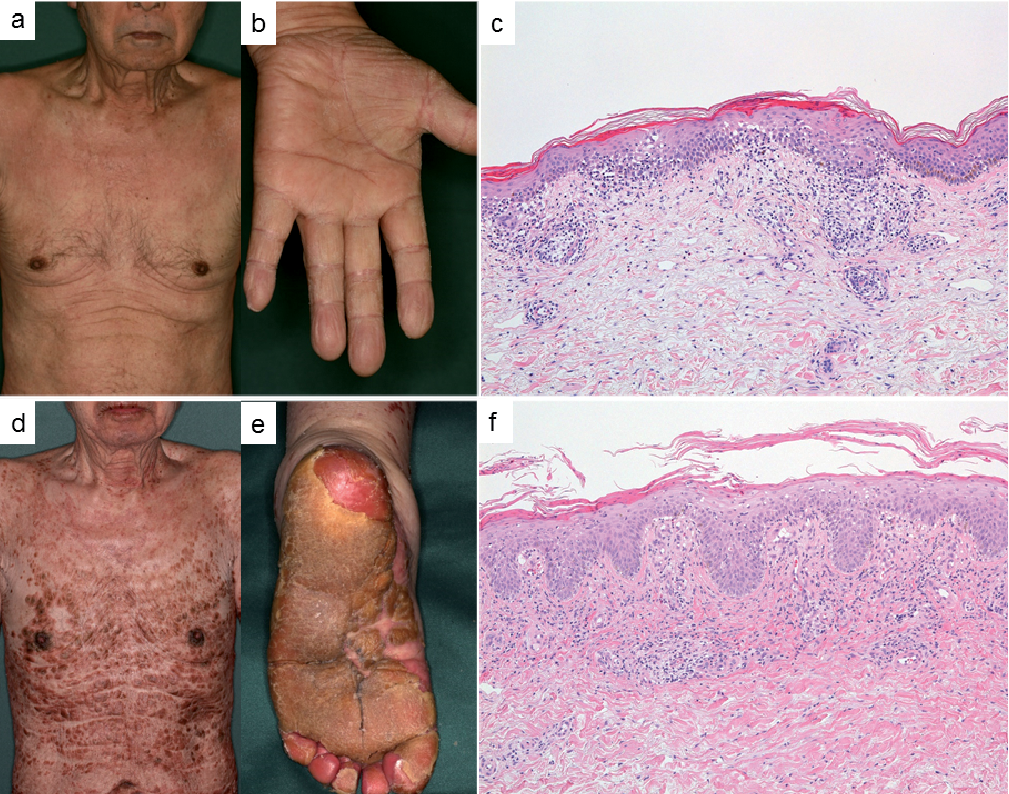
Physical examination revealed widespread erythema with papules predominantly on the trunk and extremities (Fig. 1a, b). A skin biopsy specimen from the left forearm showed vacuolar interface dermatitis with exocytosis of lymphocytes and perivascular infiltration of lymphocytes in the dermis (Fig. 1c). These lymphocytes did not exhibit significant atypia. A lymphocyte stimulation test was negative for spironolactone, tamsulosin, bisoprolol fumarate, carbocisteine and potassium chloride. Thus, we suspected drug reaction due to mogamulizumab. He was treated with topical application of 0.05% clobetasol propionate and oral levocetirizine hydrochloride (5 mg) every day for 2 months, resulting in partial clinical improvement.
Fig. 1. Clinical pictures at (a, b) the first and (d, e) the second eruption phases, and histology at (c) the first and (f) the second eruption phases. (Haematoxylin-eosin, original magnification ×100).
Three months after the skin lesion first appeared, despite the discontinuation of mogamulizumab administration, the erythematous eruptions deteriorated. Physical examination revealed widespread erythema with solid papules predominantly on the trunk and extremities and palmoplantar hyperkeratosis (Fig. 1d, e). A skin biopsy from the right lower leg disclosed hyperkeratosis with exocytosis of small lymphocytes without any atypia, vacuolar alteration in the junctional zone and marked perivascular lymphocytic infiltrates in the dermis (Fig. 1f). A peripheral blood sample showed no reactivation of varicella zoster virus, cytomegalovirus, Epstein-Barr virus or human herpes virus 6. Anti-nuclear (× 40, normal < 40), anti-double-stranded DNA (< 0.5, 10 IU/ml) and anti-phospholipid (< 8, normal < 10 U/ml) antibodies were negative and complement levels of C3 (88 mg/dl, normal 86–160 mg/dl) C4 (24.6 mg/dl, normal 17–45 mg/dl) and CH50 (55.9 U/ml, normal 31–58 U/ml) were within normal limits.
Immunohistochemically, lymphocytes infiltrating the dermis in both the first and second eruptions were positive for CD3, CD4 and CD8, but negative for CD20 and CD79 (Fig. S1a–c). Intriguingly, there was exocytosis of CD8+ T cells as well as granzyme B+ cells (Fig. S1d). Based on these findings, we diagnosed the skin lesions as vacuolar type of interface dermatitis after depletion of CCR4+ cells by mogamulizumab. We treated the patient with prednisolone (30 mg daily) for one week. This treatment resulted in a response, and the skin lesions were controlled by prednisolone alone (5–15 mg daily) for the next 4 months with no recurrence of ATLL.
Mogamulizumab was initially investigated for its therapeutic potential to target ATLL cells expressing CCR4, and it is also expected as a drug with a novel strategy to treat ATLL through stimulation of immune cells resulting from regulatory T cells (Treg) depletion (9). Reduction of Tregs by mogamulizumab also poses risks of Stevens-Johnson syndrome (SJS) that is inversely correlated with the presence of Tregs in the skin (10, 11). However, SJS can be excluded by the absence of target lesions, the absence of a significant number of eosinophils, and the absence of numerous necrotic keratinocytes in the present case. In addition, because of the impaired suppressive function of Tregs in lupus erythematosus (LE), depletion of Tregs may also lead to LE in our case (12). While histological features of cutaneous LE can exhibit vacuolar interface dermatitis, as was true in our case (13), the lack of a thickened basement membrane, of mucin deposition, of fibrinoid degeneration of collagen bundles, of nodular lymphocytic infiltration in the dermis, and negative autoantibodies in the present case do not support this possibility.
Although there was no dense band-like inflammatory infiltration in the papillary dermis in either of the episodes in this patient, the presence of HTLV-1-associated lichenoid dermatitis caused by CD8+ T cells can be seen in association with elevated immunity towards HTLV-1 infected CD4+ T cells (14, 15). Therefore, skin reaction by mogamulizumab in our patient may provide evidence that CD8+ T cells are promoted by the reduction of Tregs because CCR4 is expressed on the surface of Tregs as well as ATLL cells.


 Click to show fullsize
Click to show fullsize