


Department of Dermato-Allergology, Herlev and Gentofte Hospital, University of Copenhagen, DK-2900 Hellerup, Denmark. E-mail: Nannie.bangsgaard@regionh.dk
Accepted Nov 10, 2016; Epub ahead of print Nov 14, 2016
Chronic spontaneous urticaria (CSU) is defined by the spontaneous appearance of wheals with or without oedema that persist for more than 6 weeks (1). The disease affects up to 1% of the general population at some time in life (2) and can be very distressing, with severe reduction in quality of life (3). Little is known about the pathophysiology of CSU.
First-line treatment for CSU is based on non-sedating, second-generation H1-antihistamine, given, if necessary, in 4-fold licensed doses (1). A significant proportion of patients with CSU remain poorly controlled on this treatment and alternative therapeutic approaches have to be considered. Several immune modulatory treatments have been used with varying effect; prednisolone, azathioprine, mycophenolate mofetil, cyclosporine, sulfasalazine and methotrexate (4).
Omalizumab, an anti-IgE monoclonal antibody (anti-IgE mAb), has been approved recently by the US Food and Drug Administration (FDA) and European Medicines Agency (EMA) for the treatment of CSU, with promising results (5).
Tumour necrosis factor alpha (TNF-α) is upregulated in both skin and serum in patients with urticaria (6, 7), and treatment with anti-TNF-α is hence expected to have an effect on chronic urticaria. There is limited data on the effect of anti-TNF-α treatment of urticaria. Wilson et al. (8) reported the effect in 6 patients with recalcitrant chronic urticaria treated with different TNF-α inhibitors, and Magerl et al. (9) describe remission of delayed pressure urticaria in one patient treated with etanercept.
The aim of this study was to investigate the effect of adalimumab on antihistamine refractory CSU.
This proof-of-concept study was performed at the Department of Dermato-Allergology, Herlev and Gentofte Hospital in accordance with the Declaration of Helsinki. The study was approved by the local ethics committee (NO. H-3-2010-109) and The Danish Medicines Agency (EUDRACT NO. 2010-022705-18). All subjects gave written, informed consent prior to enrolment.
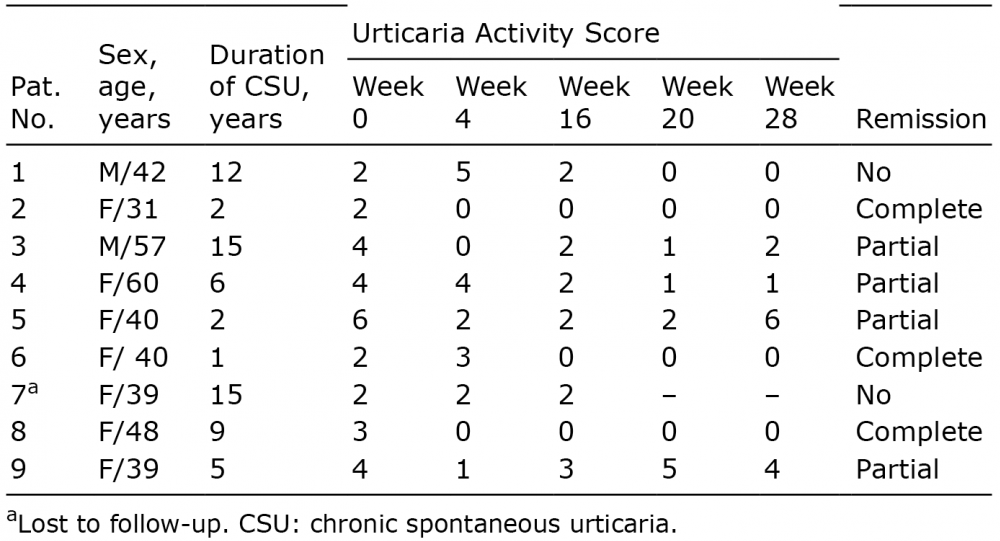
Nine patients with CSU refractory to H1-antihistamine in 4-fold licensed doses were included in the study. Baseline data for enrolled patients are shown in Table I. Prior to enrollment patients were screened for infectious diseases, including hepatitis, HIV and tuberculosis. The protocol for adalimumab treatment of psoriasis was followed.
Table I. Baseline data and results of Urticaria Activity
Score, the past week, in 9 included patients
The patients were treated subcutaneously with a loading dose of 80 mg adalimumab (Humira®; R&D systems, Abington, UK), followed by 40 mg every other week for 16 weeks. Patients were evaluated at baseline, during the treatment at week 4, 9 and 16, and after treatment discontinuation at week 18, 20 and 28. The patients were evaluated using a visual analogue score (VAS), the Urticaria Activity Score (UAS) (10), Dermatology Life Quality Index (DLQI), as well as questions from validated Danish versions of the Structured Itch Questionnaire, Becks Depression Inventory, Pittsburgh Sleep Quality Index, Brief Symptom Inventory and Somatosensory Amplification Scale. Patients reported symptoms for the previous week. The primary endpoint was change in UAS at week 16. TNF-α levels were measured at baseline and week 9 using Quantikine HS enzyme-linked immunoassay (ELISA).
Nine patients completed the study. The results of UAS at baseline, week 4, 16, 20 and 28 are shown in Table I. Patients 2, 6 and 8 achieved complete remission, defined as a UAS of 0 at week 16. The effect lasted throughout the follow-up period. Patients 3, 4, 5 and 9 experienced improvement in symptoms, with a reduction in UAS, as well as DLQI and VAS scores at week 16. Two patients had no effect, measured with UAS, but did report improvement in DLQI and VAS at week 16.
The mean ± SD level of serum TNF-α at baseline was 1.19 ± 0.455 pg/ml and the mean reduction in TNF-α level week 9 was 10.8 ± 11.37% (not significant).
No patients reported any adverse effect during the study and all screening blood tests during the study were normal.
CSU is a disease with a significant reduction in quality of life that needs to be treated (3). There has been a strong demand for treatment options, which, with the introduction of omalizumab, has largely been met (5). There are, however, patients who do not respond to omalizumab or, due to side-effects, cannot be treated with this product.
TNF-α is upregulated in both skin and serum of patients with urticaria, and TNF-α inhibitor is theoretically expected to have an effect on CSU, but this has only previously been investigated in two small studies (8, 9). In this small study we show an effect of TNF-α inhibitors on CSU. The effect is not as good as that seen with omalizumab, and we do not suggest TNF-α-inhibitors as an alternative to omalizumab treatment; however, TNF-α-inhibitors are worth considering as a treatment option for antihistamine refractory CSU in patients who do not respond to omalizumab or who, although rare, due to side-effects cannot be treated with this product.
Interestingly, two-thirds of patients who experienced complete remission already had UAS 0 at week 4 and in these, as in all of the patients who experienced an effect, the effect lasted throughout the follow-up period, for 12 weeks after medication was discontinued. This lasting effect was also seen in the 6 patients reported by Wilson et al. (8). The mechanism for this is unclear. Trials with omalizumab have demonstrated a mean of 10 weeks before symptoms return and re-administration is needed. The optimal duration of therapy and dosing interval for TNF-α-inhibitors have not been studied, but we suggest using the regimen known from psoriasis treatment, i.e. a 80 mg subcutaneously loading dose followed by 40 mg subcutaneously every other week.
In summary, this study shows an effect of adalimumab in patients with CSU, and thus should be considered for use in patients refractory to omalizumab. The study is limited by the small number of patients, but the results add to those of 2 other small studies published previously (8, 9).
Conflict of interest. Abbvie sponsored the medicine used in this study, but was not involved in the design of the study, interpretation of data or preparation of the manuscript.


 Click to show fullsize
Click to show fullsize