


1Unit of Psychooncology and Health Psychology, Department of Oncology, Aarhus University Hospital, 2Department of Psychology and Behavioural Science, Aarhus University, Aarhus, 3Department of Dermatology and Allergy, Gentofte Hospital, University of Copenhagen, Hellerup, and 4LEO Pharma, Ballerup, Denmark
Studies demonstrating the negative impact of paediatric psoriasis on health-related quality of life (HRQOL) are accumulating, but little is known about moderators of HRQOL. The objectives of this review were to summarize studies on HRQOL in paediatric psoriasis and to explore the potential moderating influences of demographic and clinical variables. Searches were conducted by 2 independent researchers in PubMed, Embase, CINAHL, PsycINFO, and Scopus for papers published between 1995 (the date the first dermatology-specific HRQOL-instrument for children was introduced) and 2016. Eligible studies were required to report HRQOL data for children and/or adolescents with psoriasis (4–18 years) using validated HRQOL questionnaires. Seven-teen eligible studies (number of patients = 1,185) were identified. Moderation analyses revealed that study samples with a higher percentage of girls were associated with better HRQOL (β = 0.19), while a higher mean age of onset (β = 0.83) and study quality (β = 0.28) were associated with lower HRQOL (all p<0.05). Several papers did not provide the information necessary for exploring between-study differences, thus the moderation analysis results should be interpreted with caution. In conclusion, children and adolescents with psoriasis experience moderate impairment of HRQOL. Certain demographic characteristics (e.g. sex) and clinical characteristics (e.g. age at onset) appear to moderate this impact.
Key words: psoriasis; health-related quality of life; children; adolescents; systematic review; meta-analysis.
Accepted Dec 15, 2016; Epub ahead of print Dec 16, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Hilde Randa, Department of Psychology and Behavioural Science, Aarhus University, Bartholins Allè 9, DK-8000 Aarhus C, Denmark. E-mail: hilderanda@psy.au.dk
Psoriasis is a common chronic inflammatory skin disease with a prevalence of 2–3% in Western countries (1–3). It is estimated that 0.7–1.2% of all children suffer from psoriasis (3, 4), with one-third of patients being diagnosed by the age of 20 years (2). Although psoriasis may take various clinical forms, the majority of children present with either plaque psoriasis (71%) or guttate psoriasis (26%) (5).
A European consensus report suggests that patients with psoriasis are both undertreated and underserved (6). Increased emphasis on patients’ overall evaluation of disease impact was identified as a major step towards better treatment for patients. Reviews of studies on functioning in adult psoriasis have shown increased rates of comorbid mental disorders, especially anxiety and depression, in addition to a range of psychosocial problems, such as poor self-esteem, social stigmatization, physical limitations, sexual dysfunction, and suicidal ideations (7, 8). Although paediatric patients have received far less research attention, a large study comparing paediatric patients with psoriasis (n = 7,404) with psoriasis-free control subjects (n = 37,020), also found a higher prevalence of depression and anxiety in paediatric patients (9). Identifying the optimal treatment for psoriasis can be a lengthy process, and the treatments can be burdensome, time-consuming, and associated with considerable side-effects (10, 11). This may further challenge patients’ well-being, especially in children who might lack a thorough understanding of the importance of treatment. Qualitative studies have also identified a number of psychosocial challenges in the daily lives of children with psoriasis (12, 13).
In recent decades, studies have shed light on patients’ subjective experiences of medical diseases and their impact on patient’s life, as captured by the construct of health-related quality of life (HRQOL) (14). Although operational definitions vary, HRQOL is generally conceptualized as a multidimensional construct reflecting patients’ physical, psychological, and social well-being (15–17). HRQOL can be measured using generic or disease-specific questionnaires. Generic instruments have been constructed to apply to healthy individuals as well as people with medical issues, whereas disease-specific instruments are tailored to specific populations with a given disease or symptom and thus tend to be more sensitive (15). Research on the association between psoriasis-related HRQOL and clinical measures of disease severity, e.g. the Psoriasis Area and Severity Index (PASI) (18), generally show modest correlations (19), indicating that the traditional measures of disease severity do not fully capture the impact of psoriasis on well-being. It is thus widely accepted that psoriasis treat-ment should aim not only at minimizing the extent and severity of psoriasis, but also at reducing the negative impact on patients’ HRQOL (6, 20, 21).
In 2004, de Korte et al. (22) published a systematic review of 17 studies on HRQOL in patients with psoriasis (mean age 47 years). Authors reported that patients experienced physical discomfort, impaired emotional functioning, negative body- and self-image, and limitations in daily activities, social contacts, (skin-exposing) activities, and work. However, they noted that the studies were highly heterogeneous, making between-study comparison difficult. Recently, Olsen et al. (23) published a systematic review and meta-analysis of HRQOL studies using the Children’s Dermatology Life Quality Index (CDLQI) across a broad range of paediatric skin diseases. Based on data from 67 studies, the authors concluded that the overall mean effect of skin disease on HRQOL in children is small. Comparative analyses showed that patients in the psoriasis subgroup (5 studies, comprising 279 patients) experienced small-to-moderate impairment of HRQOL, although results for this subgroup should be interpreted with caution due to wide confidence intervals.
To the best of our knowledge, no systematic review evaluating HRQOL in paediatric psoriasis based on the full range of available HRQOL instruments has yet been published. Furthermore, little is known about the possible associations between HRQOL and demographic and clinical variables. To aid clinical decision-making, we conducted a systematic review and meta-analysis with the aim of evaluating the impact of psoriasis on HRQOL in patients aged between 4 and 18 years, and to explore the relationship between demographic and clinical variables and HRQOL in this population.
The present study was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting systematic reviews (24). The literature search, study selection, and data extraction were guided by an a priori-developed study protocol and conducted by 2 independent reviewers. Details are given in Appendix S1 (25–45).
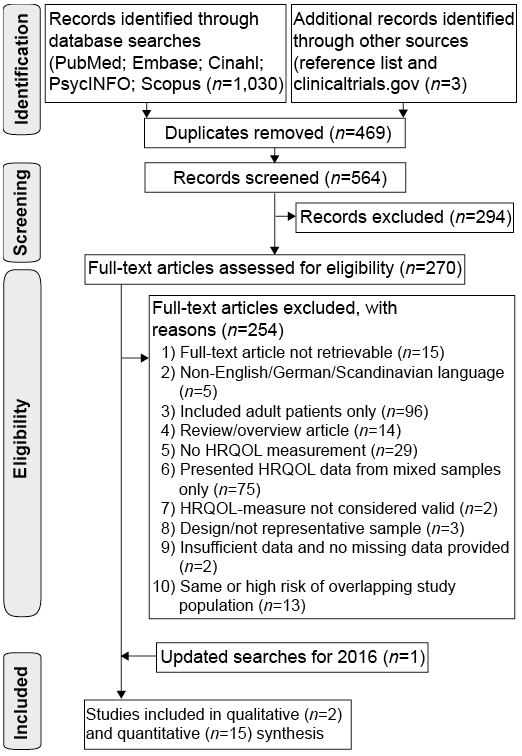
The study selection process is shown in Fig. 1. In a first screening, 2 reviewers (HR, TT) independently removed duplicates and reviewed titles and abstracts, resulting in 270 studies eligible for full-text screening.
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the study selection procedure.
This included one additional study identified from the reference list of an existing systematic review and meta-analysis (23), and 2 studies from reference lists of the included articles. Initially, the raters were uncertain or disagreed on 6 (2.2%) papers (inter-rater agreement: 0.93; kappa statistic). After negotiation, 2 of these were included, along with one additional study identified in updated searches for 2016. The search and selection process resulted in a total of 17 papers, describing data for 20 groups of patients that could be subjected to meta-analysis, and 2 study samples that could only be reviewed qualitatively (46, 47).
Fifteen authors of publications presenting results of mixed study populations (i.e. children and adults, and multiple skin diseases) or papers failing to provide the necessary values for effect size estimation were contacted. This resulted in the inclusion of 2 studies that had originally been excluded (33, 48). Furthermore, 10 authors of the included publications were contacted, requesting additional demographic and clinical information about study participants to be used in the moderator analyses. This was provided by 3 authors (33, 49, 50). Eleven papers (comprising data from 7 studies) were based on the same patient registry database and described potentially overlapping samples (49, 51–60). When contacted, the research group responsible for these studies was unable to specify the amount of overlap across studies. All but the most inclusive study (49) and a second study investigating patients of older age than in the remaining studies (60) were therefore excluded. The main reasons for exclusion were that papers only presented HRQOL data on pooled data from children and adults or from patients with various types of skin disease, that they included adult patients only, or that they did not include HRQOL assessment (see Appendix S2).
The characteristics of the included studies are shown in Table SI. The 17 studies investigated a total of 1,185 children and adolescents between the age of 4 and 18 years (mean age 12.8 years), with a majority of girls (57.9%). The included studies were conducted in 10 different countries, with 16 papers being published in English and one in German. Two studies collected data from randomly selected patients from general population databases (46, 61). All the remaining studies recruited patients from dermatology outpatient clinics. Seven studies reported clinical disease severity, as assessed with the Psoriasis Area and Severity Index (PASI). In these studies, mean disease severity ranged from 2.7 to 21.1, and the mean PASI score across studies was 11.5, indicating moderate to severe psoriasis. With the exception of 4 studies including only patients with plaque psoriasis (34, 35, 48, 62), most studies either did not specify or included the full range of clinical subtypes.
Three studies were intervention studies and the remaining 14 used observational designs. Of these, half of the studies focused on patients with psoriasis only (k (number of studies) = 7), while the remaining studies included comparative data from patients with other diseases (k = 5) or healthy controls (k = 2). The primary objectives in the observational studies were: (i) to assess HRQOL in paediatric psoriasis and/or examine the relationship between demographic, clinical or psychological variables and HRQOL; (ii) to test the psychometric performance of HRQOL instruments; and (iii) to compare HRQOL across different dermatological or chronic diseases.
HRQOL assessment was based on 4 validated questionnaires that were either generic or dermatology-specific. The majority of studies (k = 12) were based on the Children’s Dermatological Life Quality Index (CDLQI) (25, 49, 50, 60–66) or the Dermatology Life Quality Index (DLQI) (48, 67) questionnaires, and one study utilized the Pediatric Quality of Life Inventory (PedsQL) (33). In addition, 2 studies included data from both CDLQI and PedsQL (34, 35). Lastly, Skindex-Teen (47) and KINDL-R (46) were used in one study each.
The CDLQI and DLQI are child (4–16 years) and adult (>16 years) versions of the Dermatology Life Quality Index (25, 68). Both versions are the currently most used instruments measuring dermatology-related quality of life in their age group (68, 69). The CDLQI consists of 10 items, and is designed for children between 4 and 16 years. It measures HRQOL across 6 subdomains; symptoms and feelings, leisure, school or holidays, personal relationships, sleep, and treatment. The total score on the CDLQI and DLQI range from 0 to 30, with higher scores indicating greater HRQOL impairment. The CDLQI has been translated and validated in more than 40 languages, with evidence of high internal consistency, test–retest reliability, responsiveness to change, and significant correlations with other subjective and objective measures in paediatric dermatology samples (70). Although the majority of studies were based on the CDLQI, 2 studies used the adult parallel version (DLQI) (48, 67). Furthermore, 7 studies used the CDLQI in older adolescents (16–17-year-olds) for which the instrument has not been formally validated.
PedsQL, the second most utilized questionnaire, is a generic instrument. The PedsQL was originally developed to study quality of life in children with cancer, and has subsequently been developed into a 23-item generic HRQOL-measure (71). The PedsQL measures patient’s perceptions of HRQOL, as defined in terms of the impact of disease and treatment the individual’s physical, psychological, social functioning, and by disease/treatment-specific symptoms. The PedsQL ranges from 0 to 100, with higher scores indicating better HRQOL. The inventory includes age-appropriate versions for children aged 5–7, 8–12, and 13–18 in addition to a parent proxy version. The PedsQL core generic self-report scale has been translated into over 60 languages. It has demonstrated sufficient reliability, validity, sensitivity and responsiveness (72), but has not been specifically validated in patients with skin disease or psoriasis.
The Skindex-Teen and the KINDL-R were each used in one study. Skindex-Teen has been validated for use in adolescents (12–17 years) with skin disease (47). Its total score ranges from 0 to 84, with higher scores indicating greater HRQOL impairment. KINDL-R is a generic instrument with a total score ranging from 0 to 100, with higher scores denoting better HRQOL. The psychometric properties of KINDL-R have been established in a general population of children and adolescents (73).
Table SII summarizes the methodological quality of the included studies. The 2 raters agreed on 235 (92.2%) of the 255 individual study quality ratings, and the between-rater total score correlation was 0.96 (p < 0.001). The mean total quality rating was 12.3 (standard deviation (SD) 3.3; range: 7–18). The majority of studies were characterized by small sample sizes, and only a few studies reported response rates (k = 7) or whether patients were in active treatment (k = 5). Additional metho-dological concerns were that clinical disease severity was only reported in approximately two-thirds of studies (k = 10), and that several studies failed to report any clinical characteristics of their study population (k = 8). Six studies used HRQOL instruments or versions that distinguished between children and adolescents, and 4 studies divided their sample into different age groups and compared HRQOL across these groups, providing information about possible effects of age.
The extracted data enabled 2 separate random-effects analyses to be conducted; one based on dermatology-specific (CDLQI and DLQI) and one on generic (PedsQL) instruments. Results of the main analyses are shown in Fig. 2. Mean dermatology-specific HRQOL impairment was based on 14 studies (including 15 independent groups), yielding an aggregated sample of 1,012 patients.
Fig. 2. Forest plot of weighted means health-related quality of life (HRQOL) in paediatric psoriasis by instrument.
Results showed a weighted mean CDLQI/DLQI score across studies of 7.7 (95% confidence interval (95% CI) 6.67–8.73), indicating moderate HRQOL impairment (36), with a 95% prediction interval from 3.6 to 11.8. Study heterogeneity was large (I2 = 88.4). The PedsQL instrument was used in 3 studies (including 5 independent groups) and a total of 370 patients. The weighted mean PedsQL score was 74.5 (95% CI 72.82–76.25), with the prediction interval ranging from 71.8 to 77.3. There were no indications of heterogeneity of results (I2) for the studies using the PedsQL. Possible publication bias was inspected visually by means of funnel plots, and statistically using Eggers’ test. Neither analysis suggested publication bias, as estimates appeared symmetrically distributed in the funnel plot, and Eggers’ tests did not reach statistical significance. The Skindex-Teen and KINDL-R were only used in one study each, and hence meta-analysis was not possible for these instruments (see Table SI for mean scores).
As seen in Table I, meta-regression revealed several moderating effects of various study characteristics on the impact of psoriasis on HRQOL. As preliminary analyses revealed high correlations (r > 0.70) between some of the demographic and clinical variables to be explored, we adjusted for these variables by entering them as covariates in the relevant regression models. Due to the limited statistical power of these preliminary analyses, we adjusted for such relationships regardless of whether the correlation reached statistical significance.
Table I. Results of meta-regression analyses
In searching for possible moderating influences of demographic variables, meta-regression analyses revealed that the percentage of girls in the study samples (adjusted for region, as r: –0.93; p < 0.001) was the only statistically significant moderator of HRQOL, with study samples with a higher proportion of girls having lower (better) mean total scores on the CDLQI/DLQI. Age was not a statistically significant moderator of HRQOL. Regarding the clinical variables, age at onset (adjusted for disease severity, r: 0.71, p = 0.178) statistically significantly moderated HRQOL, with higher age at onset being associated with higher (worse) CDLQI/DLQI scores. In addition, psoriasis severity (adjusted for age at onset) emerged as a near-significant moderator of HRQOL, while duration of psoriasis did not. Finally, study quality also statistically significantly moderated the results, with higher study quality scores being associated with greater HRQOL impairment. For studies using the PedsQL instrument, the meta-regression analyses did not reveal any significant determinants of HRQOL. All moderator analyses regarding PedsQL data were based on either 4 or 5 studies, and hence suffered from low statistical power.
This systematic review and meta-analysis provides an overview of HRQOL in 1,185 children and adolescents with psoriasis from 10 different countries. The results of the meta-analyses revealed weighted mean total scores of 7.7 (95% CI 6.67–8.73) for studies using CLDQI and DLQI, and 74.5 (95% CI 72.82–76.25) for PedsQL, indicating a moderate effect on HRQOL (36). A sensitivity analysis excluding the two DLQI-studies from the CDLQI/DLQI analysis, revealed an unchanged weighted mean score. The PedsQL is a generic instrument, and, while published data from normative samples are available online, there are currently no data on the interpretability of PedsQL scores in paediatric psoriasis.
Our main result regarding the impact of paediatric psoriasis on HRQOL as measured by the CDLQI/DLQI is consistent with findings from a previously published meta-analysis (23), which combined data from 6 studies on 279 patients with psoriasis. However, the authors noted that the confidence intervals were particularly wide for the psoriasis subgroup, and that the estimate might be too conservative. They suggested that psoriasis-related HRQOL might be similar, or even worse, than the moderate impairment reported by the atopic eczema subgroup. In the present study, to assist the interpretation of results, prediction intervals were calculated, showing that mean CDLQI/DLQI scores in paediatric psoriasis populations are expected to fall within the range between 3.6 and 11.8. In clinical terms, this relatively broad interval ranges from a small to moderate effect on HRQOL, and thus does not support Olsen et al.’s interpretation that psoriasis might be associated with greater HRQOL impairment than atopic eczema (23).
To our knowledge, the present meta-analysis is the first to summarize findings on HRQOL across studies in paediatric psoriasis, taking the influence of demographic and clinical variables into account. The relevance of searching for potential moderators was highlighted by the large heterogeneity of studies using the CDLQI/DLQI. Our moderator analyses revealed statistically significant effects of sex, age at onset, and study quality, but not of age, psoriasis duration, or geographical region. Clinical disease severity (PASI) was a near-significant moderator of HRQOL. However, because several of the included studies failed to report important demographic and clinical characteristics of their study participants, these results should be interpreted with caution.
Although not directly comparable to our systematic review, due to the sample consisting mainly of adult patients (mean age in studies ranged from 43 to 56 years), de Korte et al.’s (22) systematic review examined relationships between background variables and HRQOL in psoriasis. Based on findings from 8 studies, the authors concluded that HRQOL seemed to be unrelated to sex, and that there was a tendency for higher age to be associated with slightly higher levels of overall quality of life. Furthermore, more severe psoriasis appeared to be associated with more impaired HRQOL. However, the authors noted that the included studies were characterized by a high degree of heterogeneity. A number of methodological shortcomings furthermore complicated the synthesis of study results, which was possible only for age, sex and disease severity (22). In contrast to de Korte et al.’s findings, we did not find any effects of age or disease duration on HRQOL, but only of age at onset. Several interpretations of our findings appear relevant.
First, the majority of studies included in our review relied on data from the CDLQI, which is designed for use in children aged between 4 and 16 years. However, many studies used this instrument in adolescents up to 18 years, or used the adult version in adolescents younger than 16 years. Considering the differences in context and social life of children, adolescents, and adults (13, 74), data from a questionnaire used with both immature 5-year-olds and maturing adolescents 15–17 years old would, perhaps, be less likely to reveal age effects.
In contrast, age at onset was statistically significantly associated with HRQOL, with paediatric patients diagnosed at an older age experiencing higher HRQOL impairment than children with early debut. This finding could possibly be explained by developmental factors. Compared with younger children, adolescents spend a considerable proportion of their time with friends, gaining independence from their families, and feeling accepted by peers is especially important (74). Coping with a newly developed skin disease and its significant cosmetic impact could be particularly difficult in a period of life when social and cultural pressures stress homogeneity in appearance as desirable. In line with this interpretation, Perrott et al.’s (75) study on stigmatization and quality of life in psoriasis, led the authors to advocate the need for clinicians to pay particular attention to children and adolescents who develop psoriasis during the critical periods of peer comparison and identity formation.
As adolescents with newly developed psoriasis may not have had sufficient time to adapt to their altered appearance, this could cause impairments in a broad range of aspects of HRQOL. Indeed, previous qualitative research has documented disrupted body image, decrease in self-confidence, social isolation, and other adverse effects on psychosocial functioning in adolescent psoriasis (12, 13). Hence, a possible explanation for our findings could be that the CDLQI instrument is not sufficiently age-sensitive, as it does not include important adolescent-specific aspects of HRQOL, such as sexual or intimacy difficulties or concerns relating to finding romantic partners and future aspirations in general (13). Our results could indicate that the difficulties associated with adolescent onset of psoriasis are so profound that even instruments with poor sensitivity towards adolescent-specific issues are able to detect some of these issues, leading to a significant effect of age at onset, but not of age per se.
If one ignores the possibility that HRQOL in psoriasis may be qualitatively different in children and adolescents, it seems reasonable to assume that longer disease duration would lead to improved coping skills and adaption to the disease over time. Based on this assumption, our finding that disease duration did not moderate HRQOL could appear surprising. It should be noted, however, that the moderator analyses of duration and age at onset may have been insufficiently powered (k = 6 and 7, respectively), and thus may be less robust than the non-significant age effects (k = 11). The explanation that the instrument is not sufficiently age-sensitive to detect age-related differences thus appears most convincing.
Sex was also identified as a moderator of HRQOL, with a higher percentage of girls in the samples being associated with less impairment. This was a relatively surprising finding, as the general literature on HRQOL in chronic disease often suggests either mixed findings (29) or greater impairment in female patients (76, 77). One explanation could be that the CDLQI/CLDQI-instruments are more sensitive to difficulties experienced by boys than those experienced by girls. To the best of our knowledge, the CDLQI has not yet been psychometrically evaluated with regard to differential item functioning (DIF), which tests for the possibility of items being biased towards certain subgroups, e.g. girls and boys (78). Although the items in the CDLQI and the adult version (DLQI) are not identical, it is interesting that item-response analysis of the DLQI caused authors to caution the use of this instrument to detect sex differences, due to violation of this assumption (79). Alternatively, other methodological issues may be responsible for our findings. Although we attempted to adjust for possible confounding variables in the meta-regression analyses, several studies failed to report numerical values concerning clinical disease severity in patients. In fact, 2 of the 3 studies with the greatest proportion of girls did not include the information necessary to be included in the preliminary correlation analysis testing for possible confounders. As clinical disease severity was established as a near-significant moderator of HRQOL, the lack of these data could be a possible explanation for our finding that samples with higher numbers of girls had less impaired HRQOL. Further studies are needed to evaluate sex differences in paediatric psoriasis HRQOL.
Although based on a relatively poorly powered moderation analysis (k = 5), our results also revealed a near-significant effect of clinical disease severity on HRQOL. This result is in line with the above-cited findings of de Korte et al. (22) that more severe psoriasis was associated with greater impairment in HRQOL. Furthermore, research within adult patients has shown positive correlations between PASI and DLQI scores in patients with moderate-to-severe psoriasis undergoing treatment (80). While only 3 studies in our systematic review included pre- and post-treatment assessments, their results all indicated reduced disease severity combined with positive change-scores on the CDLQI across different treatment regimens (34, 49, 62). As the assumption that this relationship is not necessarily linear has been broadly advocated (6), further research is needed to establish the association between clinical disease severity and HRQOL.
When exploring associations with methodological quality, we found greater HRQOL impairment in studies of higher quality. All intervention studies scored relatively high on study quality. As these studies included only patients within the moderate-to-severe psoriasis range, and disease severity was a near-significant moderator of HRQOL, this could explain the moderating effect of study quality as an indirect effect of variation in study designs. When exploring differences between studies conducted in Western vs. other countries, we found no moderating effect.
This is the first study to summarize the impact of paediatric psoriasis on HRQOL and to explore the moderating effects of demographic and clinical variables. Our study has several strengths. First, it was based on a comprehensive search and conducted in accordance with recommended guidelines (24). Secondly, to limit the influence of publication bias, we also searched for material from the “grey literature”, e.g. conference abstracts and unpublished studies. Thirdly, because of the scarcity of published data on patients with paediatric psoriasis, we made a great effort to collect non-published data from the identified studies.
Some study limitations should also be mentioned. First, we found high heterogeneity of studies using the CDLQI/DLQI, suggesting systematic between-study variance rather than variation due to random sampling error. Statistical heterogeneity should not necessarily be interpreted as a limitation or flaw, either in the individual studies or in the meta-analytic process, but indicates that the weighted mean should be viewed as an estimate of the mean expected HRQOL impairment across a wide range of different groups and settings.
A second limitation could be that, due to the limited number of studies, we included studies using the CDLQI in adolescents of 16–17 years of age, as well as studies using the DLQI in adolescents. However, neither the CDLQI nor the DLQI instrument is designed specifically for 16- and 17-year-olds with skin disease (60), and studies of patients with psoriasis who were younger than 18 years usually combine data from children and adolescents. Van Geel et al. (60) compared scores on the child (CDLQI) and adult (DLQI) version of the instrument in 16–17-year-old patients with psoriasis. Although a high correlation (r = 0.90) was found between total scores on the 2 instruments, the mean total score on the DLQI was statistically significantly lower than the mean CDLQI score. The difference between scores across the versions was driven primarily by adolescents scoring lower on the DLQI-item concerning sexual difficulties (“Over the last week, how much has your skin caused any sexual difficulties?”), and higher on the corresponding item addressing sleep problems in the CDLQI-version. The wording of the question in the DLQI-version refers to sexual difficulties over the previous week only, and does not appear to be particularly appropriate for adolescents. Previously mentioned research indicate that they might have qualitatively different experiences than adults when it comes to sexuality and intimate relationships (13, 74), and also less frequent sexual experiences.
Thirdly, as most studies report no sex difference in the prevalence of paediatric psoriasis (81), our results could have been influenced by the finding that girls were over-represented in the studies included in both random-effects models. However, when comparing the un-weighted mean values for CDLQI/DLQI (7.77) and PedsQL (74.43) with the random effects weighted averages (7.70 and 74.53, respectively), the results differed only marginally, indicating that the sex skewness is unlikely to pose a problem for our interpretation of results.
Fourthly, most studies in our systematic review investigated patients recruited from secondary care settings, and hence the samples might not be representative of the general population of paediatric patients with psoriasis. HRQOL in children and adolescents not seeking help for their psoriasis-related skin problem may be different from the HRQOL of patients undergoing treatment.
Lastly, the studies included in our meta-analyses used generic and dermatology-specific instruments only. Since disease-specific measures, e.g. psoriasis-specific instruments, are acknowledged to be more sensitive towards disease-specific aspects, this may have resulted in failure to detect potentially true effects.
The present meta-analysis suggests that children and adolescents with psoriasis experience a moderate impairment in HRQOL. The wide prediction interval for studies using the CDLQI/DLQI instrument, combined with the results of our moderation analyses, highlight the importance of measuring HRQOL to inform treatment planning, and the need for future studies to explore potential determinants of HRQOL.
To improve our knowledge about psoriasis-related HRQOL in children and adolescents, future studies should: (i) take care to provide separate data for different age- and disease-groups; (ii) collect and report relevant demographic (age; sex) and clinical (disease severity; subtype; age at onset; duration; treatment status) information on study participants, and (iii) include validated measures of HRQOL in intervention studies.
Furthermore, we were unable to identify any psoriasis-specific HRQOL instrument for children and adolescents, except for 1 questionnaire designed for paediatric patients with scalp psoriasis (57). Moreover, closer examination of the included instruments revealed that patients with psoriasis were often highly underrepresented or absent in the validation studies of the HRQOL instruments utilized for this population (25, 47). This raises further concerns about the applicability of existing HRQOL instruments in paediatric psoriasis.
The authors would like to express their thanks to the researchers who provided valuable additional data on their studies.
Conflicts of interest and funding: HR is an industrial PhD student situated at the Department of Psychology and Behavioural Science, Aarhus University, Aarhus C, Denmark. Her work is financed by LEO Pharma A/S, Ballerup, Denmark, and the Innovation Fund Denmark. LSL is employed by LEO Pharma A/S. The remaining authors declare no conflicts of interest. The funding source had no influence on data collection, and no influence on the decision to submit.


 Click to show fullsize
Click to show fullsize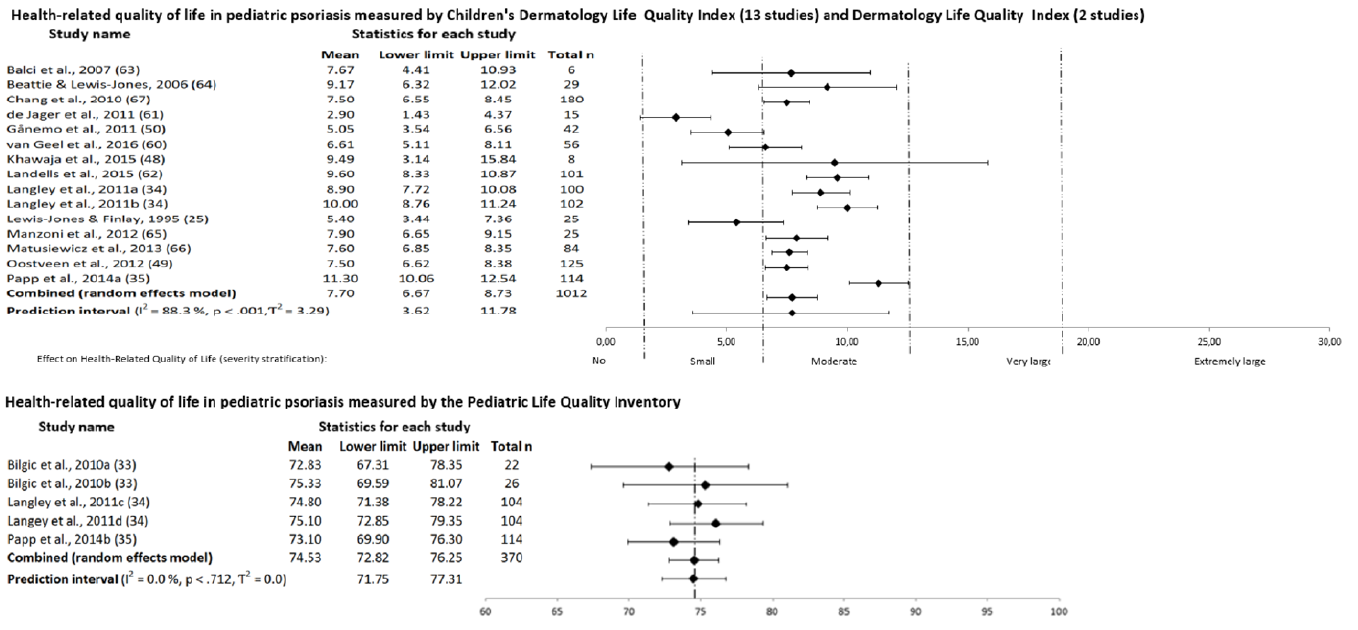 Click to show fullsize
Click to show fullsize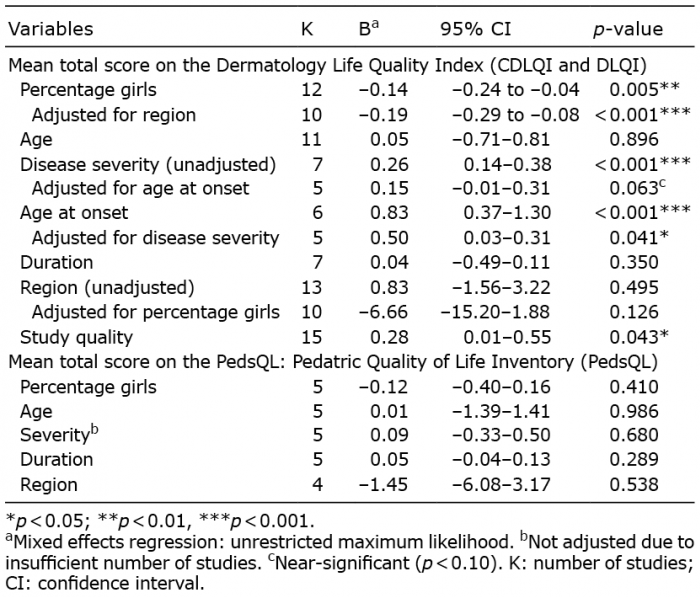 Click to show fullsize
Click to show fullsize