


Dermatology Service, Hospital Universitario Fundación Alcorcón, ES-28922 Madrid, Spain. E-mail: Jllopez@fhalcorcon.es
Accepted Jan 12, 2017; Epub ahead of print Jan 17, 2017
Actinic keratoses (AK) commonly occur in elderly patients as a result of chronic exposure to ultraviolet radiation (1). While isolated AK lesions are usually treated with liquid nitrogen cryosurgery, subclinical lesions occurring in photo-damaged areas are treated by photodynamic therapy and topical agents (imiquimod, 5-fluoruracil, diclofenac, and ingenol mebutate) (2). The advantages of these treatments are that they are non-invasive, self-administered and effective against both clinical and subclinical lesions, but most of them require a long course of treatment and are associated with a high frequency of local skin reactions (LSRs). The most recently approved agent, ingenol mebutate (IM), needs to be applied for only 2 or 3 days, it has a shorter duration of LSRs, and improved adherence (3–5).
Dermoscopy and reflectance confocal microscopy (RCM) are a help in diagnosis of AK and subsequent monitoring of treatments (6–8). A correlation between these techniques and histopathological examination has been demonstrated (6, 9). RCM offers the possibility of detecting morphological changes in clinical and subclinical AK at the treated area (10) and has been used to follow AK in response to different topical treatments (11). Two recent studies reported successful monitoring of morphological changes in AKs treated with IM using a dermoscopy, optical coherence tomography and RCM (7, 12). The aim of this case series report was to evaluate the response to IM gel in AK treatment on the face or scalp using RCM and clinical assessment.
A total of 17 patients were enrolled in a prospective study of case series. All patients were over 50 years of age, with a clinical diagnosis of AK on the head and face, and indication for ingenol mebutate (IM) treatment. The study was approved by the local ethics committee and written informed consent was obtained from each participant before evaluation.
All patients were treated with IM 0.015% gel (Picato®, LEO Pharma, Ballerup, Denmark) applied once daily for 3 consecutive days in the affected area, covering both clinical AK and the area surrounding the lesions (field of cancerization), and area of approximately 25 cm2.
AK in the target area were examined clinically to evaluate the treatment response at baseline and at the 8th week follow-up visit, while RCM imaging was performed before treatment and at weeks 4 and 8. Images were obtained using a digital camera (Canon PowerShot G12, Canon USA Inc., New York, USA). Lesions were rated as complete response (CR; complete disappearance of the lesions in the treatment area), partial response (PR; reduction of ≥ 50% in the number of clinically visible AK) or non-response.
RCM images of the areas selected at baseline were captured with a commercially available hand-held device (VivaScope 1500; Lucid-Tech, Inc., Henrietta, NY, USA). RCM images 6 × 6 mm were obtained horizontally from the lesion using the VivaBlock function modality. Vertical mapping using the VivaStack was performed at intervals of 5 μm up to a depth of 200 μm, beginning with the stratum corneum (SC) through the entire epidermis and into the superficial dermis. Based on previous AK diagnostic criteria, the study areas were evaluated for the presence or absence of the following RCM features of AK: hyperkeratosis, parakeratosis, disruption of the SC (irregular cornea), overall architectural disruption (atypical honeycomb pattern, architectural disarray, and irregular epidermal pattern), blood vessel dilatation, inflammatory infiltrate, and solar elastosis.
Of the 17 patients initially recruited into the study, 15 had follow-up data until week 4, and 12 patients finalized the study with evaluation at week 8. Demographic and clinical characteristics of patients, including AK clinical severity (Olsen grade) and RCM parameters at baseline are summarized in Table SI.
The therapeutic outcome at week 8 was evaluated clinically as CR in 7/12 (58%) patients and PR in 4/12 patients (33%). Only one patient was classified as a non-responder.
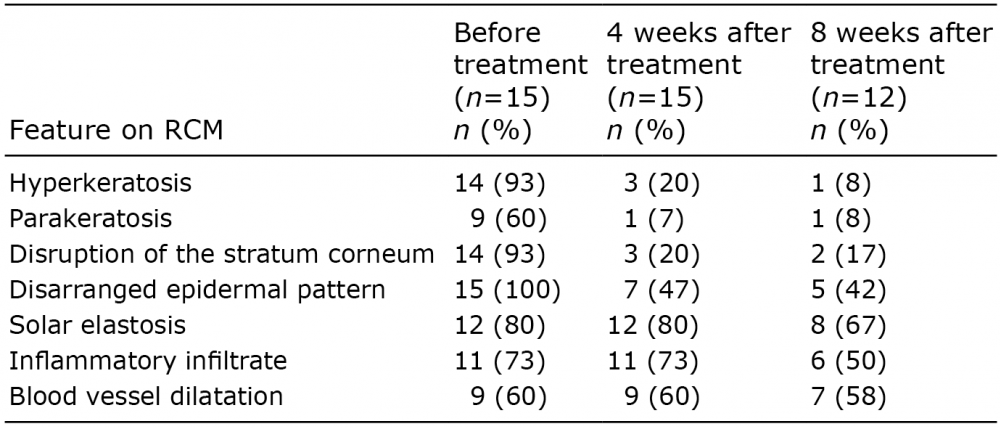
To detect morphological changes following topical applications of IM, RCM evaluations of AK were performed at baseline and at weeks 4 and 8 after treatment. Disarranged epidermal pattern was identified in all patients before initiation of treatment. Disruption of SC and hyperkeratosis were seen in 14/15 patients. A decreasing frequency of these abnormal features and parakeratosis was observed at week 4, especially in the number of patients with hyperkeratosis and disruption of the SC (identified in only 3 patients, respectively). Overall, these results were maintained at week 8 of follow-up. On the other hand, solar elastosis, inflammatory infiltrate and blood vessel dilatation were found in the same number of patients at baseline and at week 4 after treatment, although there was a slight reduction in frequency at week 8. Values for various RCM parameters are shown in Table I at each time-point. RCM images before and after IM treatment are shown in Figs 1 and 2.
Table I. Reflectance confocal microscopy (RCM) findings before treatment, and 4 and 8 weeks after treatment
Fig. 1. Reflectance confocal microscopy image of actinic keratosis before treatment. (A) Areas with bright and nucleated cells (parakeratosis) at the stratum corneum (SC) (arrows). (B) Disruption of the SC (arrow), with hyperkeratosis (asterisk) (mosaic 4 × 4 mm). (C) Disarranged epidermal pattern (atypical honeycomb patterns) and presence of atypical keratinocytes with irregular size and shape (square) (0.5 × 0.5 mm).
Fig. 2. Reflectance confocal microscopy image of actinic keratosis at 8 weeks after treatment. (A) Normalization of honeycomb pattern. (B) Solar elastosis that persisted after treatment (asterisks). (C) Blood vessel dilatation that persisted after treatment (arrows) (0.5 × 0.5 mm).
All patients presented local skin reactions to IM, consisting of skin irritation with erythema and scaling, the majority of which were mild (8 patients, 57%); 3 patients (25%) showed moderate irritant reactions and one patient had a severe reaction requiring treatment with prednisone.
IM is a diterpene ester currently approved for non-hyperkeratotic and non-hypertrophic AK treatment. In this report, we present a case series of 15 patients with AK on the face or scalp, who received topical treatment with IM 0.015% for 3 consecutive days. Before treatment, RCM images showed disruption in the SC, hyperkeratosis, and an atypical honeycomb pattern of the epidermis with atypical keratinocytes. Architectural disarray at the level of the spinous layer and keratinocytic pleomorphism were found to be the best discriminatory features of AK, as described previously (8). At week 4 after the end of treatment the variation in the confocal parameters observed with RCM showed a reduction in these abnormal features, followed by a reduction in parakeratosis, as a sign of progressive normalization of keratinocytes maturation. The improvements persisted at the end of the study after 8 weeks. No variation was observed in the microscopic signs of inflammation at the first weeks after completing treatment, probably due to the complex inflammatory response to the treatment (13).
In previous studies (7, 12), RCM has proven to be an excellent tool to monitor the response to IM. The RCM evaluation 8 weeks after completing the treatment revealed improvement in the atypical honeycomb pattern and hyperkeratosis, as previously described with other therapies effective on the field of cancerization (8, 12, 14, 15).
The detection of dermal RCM features of AK may be limited by the presence of significant hyperkeratosis. However, our findings support the utility of RCM, not only in the diagnosis, but also in the monitoring of the response of AK to treatment. The main limitation of our study was the small number of cases reported. Further studies will be useful to validate these preliminary findings, and to consider RCM as a valuable tool on the routine management of new treatments for AK.
Conflicts of interest: JLLE has participated as an speaker and advisor for LEO, Meda, Almirall and Galderma.


 Click to show fullsize
Click to show fullsize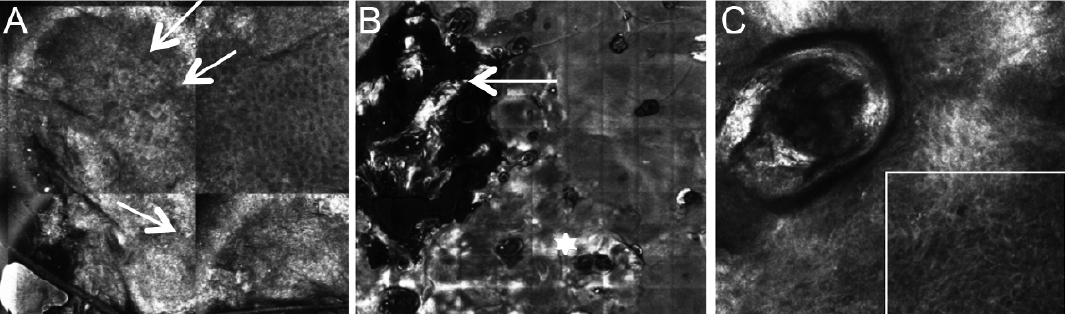 Click to show fullsize
Click to show fullsize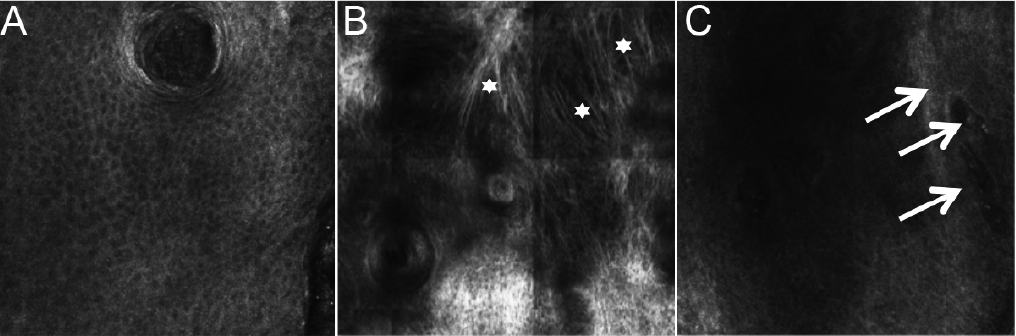 Click to show fullsize
Click to show fullsize