


1Department of Dermatology, Rambam Health Care Campus and 2School of Public Health, Faculty of Social Welfare and Health Sciences, University of Haifa, 3Rappaport Faculty of Medicine, Technion-Israel Institute of Technology, Haifa, Israel
All-cause and cause-specific mortality among patients with pemphigus compared with the general population is yet to be established. This study investigated overall mortality and cause-specific mortality in a large immunopathologically validated cohort of patients with pemphigus. Mortality of patients with pemphigus was compared with age- and gender-matched control subjects in the general population. All-cause and cause-specific standardized mortality ratios (SMRs) were estimated. The study cohort included 245 patients newly-diagnosed with pemphigus between January 1990 and June 2016, contributing 2,679.4 person-years of follow-up. Overall, 48 deaths were observed during a mean follow-up period of 10.9 ± 8.1 years, which was more than twice the number expected (SMR 2.4; 95% confidence interval (95% CI) 1.82–3.20). The SMRs for death due to infections (22.6; 95% CI 13.6–35.3), namely pneumonia (25.7; 95% CI 11.7–48.8) and septicaemia (8.6; 95% CI 1.7–25.0), and due to cardiovascular diseases (2.8; 95% CI 1.0–6.0) were significantly higher than expected. Overall mortality among patients with pemphigus is 2.4-times greater than for the general population, mainly due to infections.
Key words: mortality; prognosis; survival; cause of death; pemphigus, Israel.
Accepted Jan 12, 2017; Epub ahead of print Jan 17, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Khalaf Kridin, Department of Dermatology, Rambam Health Care Campus, POB 9602, Haifa 31096, Israel. E-mail: dr_kridin@hotmail.com
P
emphigus is a rare, chronic, potentially life-threatening, autoimmune blistering disease of the skin and mucous membranes. There are 2 major subtypes of pemphigus: pemphigus vulgaris (PV) and pemphigus foliaceus (PF). The aetiopathogenesis of pemphigus is characterized by acantholysis and intraepidermal blister formation, resulting from IgG autoantibodies directed against desmoglein (Dsg) 3 (PV) and/or Dsg 1 (PF), 2 transmembrane desmosomal glycoproteins (1, 2).
Mortality from pemphigus was dramatically reduced, from 75% to 30%, due to the use of corticosteroids in the early 1950s (3). The adjuvant use of immunosuppressants in the 1980s probably contributed to the further decrease in mortality from the disease itself to below 5% in study populations and 0.021 per 100,000 inhabitants in the USA (3–5). In 2 recent population-based studies using computerized databases and lacking immunopathological validation, the age- and gender-adjusted mortality was estimated to be 2- to 3-fold higher than for the general population (6, 7). Infections, in particular pneumonia and septicaemia, were the most frequent causes of death in different study populations (7–9). Cardiovascular diseases and peptic ulcer disease were also significant causes of death compared with the control population (7).
The aim of this study was to determine the overall and cause-specific mortality of patients with pemphigus in relation to an age- and gender-matched population in Israel. The data obtained represent the first analysis of mortality in patients with pemphigus compared with the general population, tracking an immunopathologically validated cohort. Due to the remarkable differences we observed in the incidence rate and age of onset between pemphigus patients of Jewish and Arab ancestry (10), we sought to compare the prognosis of patients from these ethnic populations.
The study population comprised all consecutive patients who received a new diagnosis of pemphigus between 1 January 1990 and 30 June 2016 in Rambam Health Care Campus, Haifa, Israel. The study cohort also included 16 (6.5%) patients who were diagnosed between 1985 and 1989, but followed up intensively during the study period. Of note, 229 of our patients were described previously to investigate differences in mortality between patients with PV and those with PF (Kridin K, unpublished data).
Pemphigus was diagnosed as a blistering disease of the skin or mucous membranes, in conjunction with characteristic histopatho-logy showing intraepidermal blisters and acantholytic keratinocytes, and with at least one positive test out of the following:
Survival status, date of death, and cause of death among patients with pemphigus was ascertained by linking the study cohort with the National Registry of Deaths Database of Haifa district. The underlying cause of death on the death certificate was coded according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9 CM) in data files. All patients were followed up from the onset of pemphigus until 30 June 2016, exiting the study earlier if they died during the observation period. The study had approval from the institutional ethics committee of our medical centre.
The observed survival curve from the onset of pemphigus was estimated using the Kaplan–Meier method. The expected survival curve of the study cohort was computed according to Hakulinen’s method (14), using gender-, age- (1-year classes), and calendar year-specific (1-year classes) mortality rates for the population of Israel (Israel Central Bureau of Statistics). To compare the observed and expected survival rates, we calculated standardized mortality ratios (SMRs), the ratio of the observed to the expected number of deaths, with 95% Poisson confidence intervals (CI). The expected number of deaths was calculated by multiplying person-years of each gender-, age (1-year classes)-, and calendar year-specific stratum of the study cohort by the corresponding mortality rate of the Israel population and then summed up across all strata. Cause-specific SMRs were also calculated based on gender-, age (5-year classes)- and calendar year-specific mortality rates for specific causes of death (if available) for the Israeli population (Israel Central Bureau of Statistics). All analyses were performed using STATA statistical software version 8.2 (StataCorp, College Station, TX, USA).
A total of 245 patients with pemphigus were included in the study. Of the patients, 151 (61.6%) were female and 94 (38.4%) were male. Mean ± SD age at diagnosis was 53.3 ± 16.3 years, median 54 (range 0–90) years. Male patients were significantly younger than female patients (49.9 ± 16.6 vs. 55.4 ± 15.8 years, respectively, p = 0.0154). The majority of patients were of Ashkenazi Jewish origin (58.8%), followed by Sephardic Jews (23.7%) and Arabs (17.1%). In one patient, the ethnic descent could not be determined. Overall, 245 patients were followed, contributing 2,679.4 person-years. The mean ± SD length of follow-up was 10.9 ± 8.1 (median 10.1) years.
In all, 48 (19.7%) patients died during the follow-up period, both in the inpatient and outpatient settings, of whom 20 were male and 28 were female. Of these, 10 (20.8%) died within one year of being diagnosed with pemphigus. Patients who survived less than one year were significantly older at the time of diagnosis than those who survived at least one year but died later (77.1 ± 8.5 vs. 60.5 ± 12.6 years, respectively, p = 0.0003). Furthermore, 21 (43.8%) of those who died during the study period died within 10 years of initial presentation. Similarly, patients who survived less than 10 years were significantly older at the time of diagnosis than those who survived at least 10 years and died later (70.8 ± 11.8 vs. 58.7 ± 12.7 years, respectively, p = 0.0015).
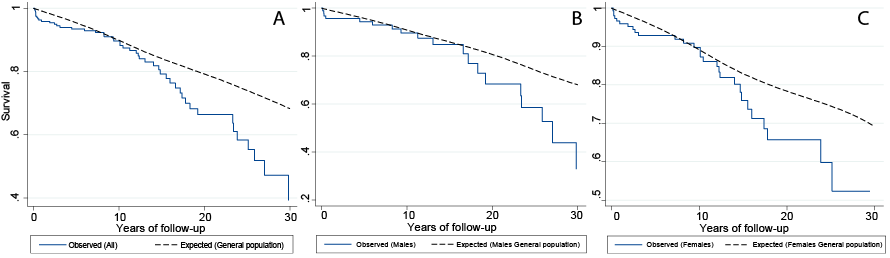
The 1-, 5-, 10-, 15- and 20-year overall survival rates were 95.8%, 93.4%, 89.7%, 79.2% and 66.3%, respectively, in the entire population of patients with pemphigus. No significant differences in survival rates were noted between genders (p = 0.86) and between Jews and Arabs (p = 0.56). The median overall survival period among patients who eventually died was 10.9 (range 0.2–35.5) years.
Kaplan–Meier survival curves for the pemphigus cohort were lower than expected in the age-matched general populations, in both genders, especially with increasing years of follow-up (Fig. 1). Relative to expected age- and gender-specific overall death rates in the general population in Israel, there was a greater than 2.4-fold excess of mortality among patients with pemphigus with a SMR of 2.4 (95% CI 1.8–3.2). In gender-specific analysis, the SMRs for patients with pemphigus were significantly higher for both men (SMR 2.7; 95% CI 1.8–4.2) and women (SMR 2.2; 95% CI 1.5–3.2). In ethnicity-specific analysis, the SMRs were significantly higher for both Jews (SMR 2.4; 95% CI 1.7–3.2) and Arabs (SMR 2.9; 95% CI 1.3–6.6).
Fig. 1. (A) Survival among all patients diagnosed with pemphigus throughout 1990 to 2016 compared with expected survival. Survival stratified by gender (B: males and C: females).
Table I presents the results of calculated SMRs further stratified by gender, ethnicity and age group at diagnosis. Most of the deaths and the highest mortality rates (49.0 and 52.1/1000 person-years for men and women, respectively) were observed amongst patients with onset of pemphigus at 65 years and older. Compared with the expected deaths in the general population, the highest SMRs were found in patients with pemphigus onset who were younger than 45 years of age, with a value of 4.7 (95% CI 1.8–12.5) for men and 3.5 (95% CI 0.5–24.5) for women.
Table I. Observed and expected deaths and standard mortality ratios (SMR) in patients with pemphigus stratified by gender, ethnicity and age at diagnosis
Table II illustrates deaths in patients with pemphigus by cause. Infectious diseases were the most commonly certified cause of death (n = 19, 39.6%), particularly pneumonia (n = 9, 18.8%), skin infections (n = 4, 8.3%) and septicaemia (n = 3, 6.3%). Other causes of death were, malignancy (n = 10, 20.8%), cardiovascular diseases (n = 6, 12.5%) and cerebrovascular diseases (n = 3, 6.3%).
Table II. Distribution of causes of death in pemphigus patients diagnosed January 1990 to June 2016
Compared with the age- and gender-matched population of Israel, patients with pemphigus showed statistically significant increased likelihood of death as a consequence of infections (SMR 23.2; 95% CI 13.9–36.2), pneumonia (SMR 26.5; 95% CI 12.1–50.3), septicaemia (SMR 8.9; 95% CI 1.8–25.8) and cardiovascular diseases (SMR 2.8; 95% CI 1.0–6.2) (Table III).
Table III. Observed and expected deaths and standardized mortality ratios (SMR) of specific causes of death
This study represents the first immunopathologically validated cohort of patients with pemphigus evaluated for all-cause and cause-specific mortality in relation to the general population. The results demonstrated that survival in patients with pemphigus was significantly lower than expected for the general population. Although we were not able to adjust for specific comorbidities, patients with pemphigus had a 2.4-fold increase in age- and gender-adjusted mortality compared with the general population.
Pemphigus is associated with a relatively high mortality rate after diagnosis, ranging in the literature from 5% to 30% during various lengths of follow-up. For example, Uzun et al. (4) reported a mortality rate of 4.8% in 148 patients with pemphigus in Turkey, during a mean follow-up period of 25 months. The study by Shamsadini et al. (15) of Iranian patients found mortality rates of 7.3%, 13.2% and 39.5% at 2, 6 and 8 years, respectively, following the diagnosis of pemphigus. Mimouni et al. (16) in analysing the course of pemphigus in 155 Israeli patients during 1976 to 2004, reported a 10% mortality. In an earlier Israeli study, Seidenbaum et al. (17) followed 115 Israeli pemphigus patients for 4–24 years, demonstrating a mortality of 22%. One study conducted in a medical centre in Northern Taiwan observed 15 deaths among 58 patients with pemphigus (25.9%) during a mean follow-up period of 9.2 years (18). Another study of 159 patients with PV admitted to a hospital in Croatia during 1980 to 1998, documented a mortality rate of 8.8% in the course of hospital treatment (19). In a recent study from the USA, patients with a secondary diagnosis of pemphigus had significantly higher inpatient mortality (3.2%) than those with a primary (1.6%) or no (1.8%) diagnosis of pemphigus (20). Prior studies mainly assessed small hospital-based samples without estimating the risk of mortality amongst patients with pemphigus relative to the general population, and some studies failed to elucidate the precise length of follow-up. The survival rate found in the current study is comparable with reports from Croatia (19) and Turkey (4), and better than reports from Iran (15) and Taiwan (18).
A population-based study conducted in the UK found that the age- and gender-adjusted mortality rate among 138 patients with PV was 3 times higher than for controls (6). In another population-based study from Taiwan, the overall mortality among 853 patients with pemphigus was 2.36-fold greater than for the general population (7). The last 2 studies were based on computerized databases without immunopathological validation, and on relatively short durations of follow-up. Nevertheless, their results were generally parallel with the SMRs calculated in our cohort.
Our data revealed that patients with pemphigus who were older than 65 years at diagnosis had much higher mortality rates than those whose disease onset was before 65 years of age, both amongst men and women. This finding is in accordance with previous reports that elderly patients with pemphigus have worse prognosis and poorer survival rates compared with younger patients (6, 7, 15). Nevertheless, the SMR was greatest for patients with onset of pemphigus before 45 years of age, because the background mortality in this age category in the general population is very low. Although men showed slightly higher SMRs, the difference between the genders was not of statistical significance (p=0.58). Despite remarkable ethnic variations in incidence rate and age of presentation (10), no significant differences were noted in mortality between Jews and Arabs (p = 0.56).
In the analysis of specific causes of death, only one patient was certified as having died directly from pemphigus; A 63-years-old PV patients died 53 days subsequent to his diagnosis due to electrolyte imbalance and severe catabolic state. In this patient, no history of chronic kidney disease was known, and a thorough work-up did not find a clue for an infection or malignancy. Thus, his death was attributed to his recalcitrant mucocutaneous disease.
Our finding contrasts with previous observations from a large-scale study from Taiwan, where 20% of deaths were directly attributed to pemphigus (7). On the other hand, our results are in line with the findings of a recent large-scale epidemiological study, which revealed that patients with secondary diagnosis of pemphigus, who are usually admitted for comorbidity, had substantially higher inpatient mortality than patients with a primary admission with the diagnosis of pemphigus (20, 21). Our study indicates that patients with pemphigus rarely die from the disease during the first year of diagnosis, as only 4.1% died in this time-period. This may be due to the improved modes of immunosuppressive therapies, leading to disease control in most patients.
Although malignancy was a major cause of death, its SMR was not significantly higher than expected. The SMRs for infectious disease, mainly pneumonia and septicaemia, and for cardiovascular diseases were all significantly higher than expected in the age- and gender-matched population. Interestingly, our results are parallel with the solitary population-based study that examined cause-specific mortality for pemphigus compared with the general population (7). The predominant mortality due to infections is ascribed mainly to steroidal and immunosuppressive therapies rendering patients more susceptible to infections (22). Regarding cardiovascular mortality, it can be expected that patents placed on high-dose steroidal therapy for long durations have an increased risk of cardiovascular mortality (23), as was demonstrated previously in rheumatoid arthritis (24), systemic lupus erythematous (25), and inflammatory polyarthritis (26). Moreover, we assume that the presence of chronic inflammatory background may represent a link between pemphigus, cardiovascular diseases and a lower survival rate, due to the direct involvement of various cytokines, such as tumour necrosis factor alpha (TNF-alpha) and interleukin (IL)-6. Both molecules were directly involved in the pathogenesis of pemphigus (27, 28), as well as atherosclerosis and coronary heart disease (29). Skin and soft tissue infections were a substantial cause of death (8.3%), but we were unable to calculate its SMR due to absence of this cause-specific mortality rate in the general population.
It has been reported, in case series and selective hospital-based cohorts, that side-effects from prolonged corticosteroid and adjuvant immunosuppressive therapy (e.g. systemic infection, pneumonia, diabetes, arterial hypertension, cardiorespiratory diseases, and peptic ulceration) were the most common complications and events leading to death in patients with pemphigus (19, 30). Our study contributes an epidemiological figure of all-cause and cause-specific mortalities compared with the general population, tracking cases with very high level of immunopathological validation.
Our study has a prominent limitation; due to the fact that it was held in a tertiary healthcare centre, we may have missed mild cases of pemphigus managed by the community dermatologist. However, pemphigus is uncommonly seen in general practice, and general practitioners and community dermatologists are highly unlikely to manage patients with pemphigus without referring to secondary or tertiary care. The 16 non-consecutive patients diagnosed between 1985-1989 did not constitute a selection bias, because their 10-years survival rate and comorbidities profile were not statistically different from the remainder 229 patients.
In conclusion, this retrospective cohort study indicates that the risk of all-cause mortality among patients with pemphigus is 2 times greater than expected for the general population. In particular, patients with pemphigus in Israel have a higher risk of mortality from infections, especially septicaemia and pneumonia, as well as cardiovascular, diseases compared with the general population. Overall, mortality was rarely directly related to pemphigus, but secondary to the systemic treatments, and overall by having an autoimmune disease
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize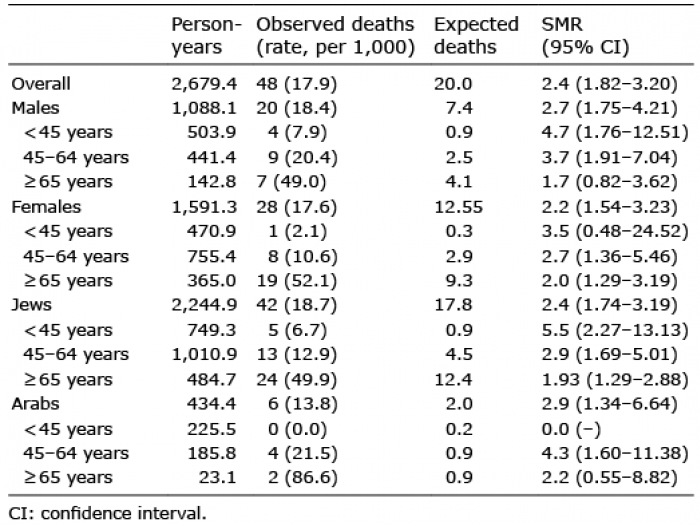 Click to show fullsize
Click to show fullsize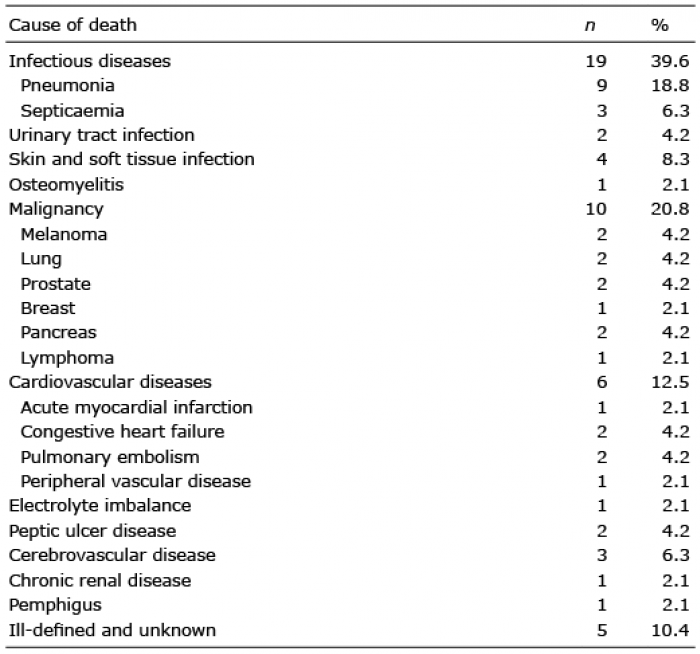 Click to show fullsize
Click to show fullsize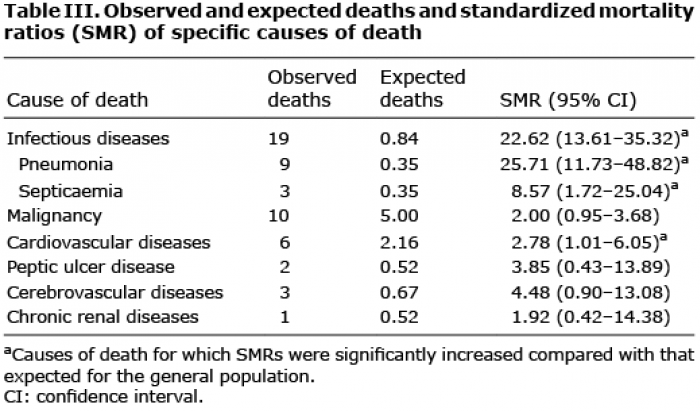 Click to show fullsize
Click to show fullsize