


1Department of Dermatology, Bispebjerg Hospital, University of Copenhagen, Bispebjerg Copenhagen, and 2Clinic of Dermatology, Broenderslev, Denmark
The efficacy of photodynamic therapy (PDT) with methyl aminolevulinate is reduced when treating actinic keratosis (AK) on the extremities in comparison with the face and scalp. Studies indicate that PDT efficacy can be improved by combining PDT with other treatment modalities. This randomized intra-individual study investigated whether pretreatment with topical 5% 5-fluorouracil (5-FU) enhanced the treatment efficacy of daylight-mediated PDT in 24 patients with AKs on the hands. One hand of each patient was given 7 days of pretreatment with 5-FU twice daily before daylight-PDT, whereas the other hand was treated with daylight-PDT alone. At 3-month follow-up the overall lesion response rate was significantly higher for the combination of 5-FU and daylight-PDT (62.7%) than for daylight-PDT alone (51.8%) (p = 0.001). Furthermore, pain and erythema in relation to treatment were similar in the 2 groups (p = 1.0 and p = 0.2, respectively). Combination therapy is a safe and effective method to improve daylight-PDT for acral AKs.
Key words: 5-fluorouracil; actinic keratosis; daylight-PDT; photodynamic therapy; pretreatment.
Accepted Jan 12, 2017; Epub ahead of print Jan 17, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Christoffer V. Nissen, Department of Dermatology D92, Bispebjerg Hospital, University of Copenhagen, Bispebjerg Bakke 23, DK-2400 Copenhagen NV, Denmark. E-mail: christoffer.valdemar.nissen@regionh.dk
Photodynamic therapy (PDT) is an established and effective treatment modality for actinic keratosis (AK) (1). In PDT, a topical prodrug is enzymatically converted into the photosensitive molecule protoporphyrin IX (PpIX) within epidermal cells. Subsequent activation of PpIX with light of appropriate wavelengths leads to necrosis and apoptosis of the affected cells (2, 3).
PDT efficacy is high when treating AKs on the face and scalp (4), but studies report efficacy rates to be approximately 20% lower on the extremities (5–8). This discrepancy in response rates was believed to be caused by insufficient PpIX accumulation in acral skin regions due to lower skin temperatures and a limited number of pilosebaceous glands (5, 8). However, in a recent study we found no improvement in PDT efficacy for AK on the hands after successfully increasing PpIX accumulation markedly (9).
Consequently, different strategies are needed to improve PDT treatment of AKs on the extremities. A promising new approach is to use PDT in combination with other treatment modalities (10). Combination therapy
has the advantage of attacking a disease through different mechanisms of action, which could produce an additive effect that exceeds the results achieved via monotherapy (11). Research is sparse, but the topical therapeutics imiquimod (12, 13), diclofenac (14), ingenol mebutate (15) and 5-fluorouracil (5-FU) (16–18) have all been combined with PDT in small studies or case reports with promising results.
For combination therapy with PDT to be attractive to both patients and physicians the treatment duration should be short, the economic burden must be low, the number of consultations should be kept to a minimum and adverse events should not exceed those of monotherapy. This makes short-term topical treatment with 5-FU an obvious candidate to combine with PDT. Consequently, we investigated whether sequential treatment with 5% 5-FU cream for 7 days could improve the efficacy of daylight-PDT with methyl aminolevulinate (MAL) when treating AKs on the hands. Furthermore, we assessed adverse events, daylight illuminance, 5-FU consumption and PpIX accumulation in relation to treatment.
Patients older than 18 years with multiple AKs on the dorsal side of both hands were recruited for this randomized controlled study with open evaluation. Exclusion criteria were: porphyrias, known allergy to the study medication, organ transplant recipients, concurrent treatment with oral immunosuppressive drugs, pregnancy, and lactation. All patients had chronic photo-damaged skin and had previously been treated with a wide range of treatment modalities for AKs on different body sites. However, no patients had been treated on the hands within the 3 months prior to inclusion.
The study was conducted from August 2015 to January 2016 at 2 dermatology clinics in Denmark and was approved by the Danish Health and Medicines Authority (EudraCT 2015-003003-29) and the ethics committee of Region Hovedstaden (H-15009690). Signed informed consent was obtained from all patients prior to study start.
AKs on the dorsal side of both hands were mapped on a template and graded according to Olsen et al. (19). Subsequently, each hand was randomly allocated to receive either daylight-mediated PDT (D-PDT) as monotherapy or sequential treatment with 5-FU and daylight-mediated PDT (5FU-D-PDT). The randomization procedure was computer-generated in block sizes of 6 and allocations were kept in opaque, sequentially numbered envelopes. Patients were then given a 20 g tube of 5% 5-FU cream (Efudix®; MEDA AS, Alleroed, Denmark) and instructed to apply a thick layer of the cream to the appropriate hand twice daily for 7 days. Because patients used the hand that was randomized to D-PDT to apply 5-FU cream to the contralateral hand, they were strictly informed to wash the D-PDT hand immediately after application to avoid cross-contamination. The tube was weighed before and after pretreatment to quantify the amount of cream the patient applied. On day 8, patients returned for daylight-PDT of both hands. A sunscreen with a sun-protection factor of 20 was applied on all sun-exposed skin areas including the hands (P20®; Riemann A/S, Hilleroed, Denmark). Approximately 15 min later, scales and hyperkeratoses were removed and the skin surfaces on the hands were roughened using a disposable curette (Acu-Dispo-Curette®; Acuderm Inc., Fort Lauderdale, USA). Subsequently, 16% MAL cream (Metvix®; Galderma Nordic AB, Uppsala, Sweden) was applied to both hands without occlusion. Patients stayed indoors for 30 min before going outside for 2 h of daylight exposure, after which residual MAL cream was wiped off with a wet towel.
Treatment efficacy was evaluated 3 months after PDT using the baseline template. The primary endpoint was complete lesion response. The complete lesion response rate was defined as the number of completely responding lesions divided by the number of lesions treated within the individual patient. Complete lesion response was classified as complete disappearance of the lesion both visually and palpably (mild erythema might remain). AKs with incomplete response were graded and any new AKs were registered.
Erythema was visually evaluated by the investigator one day after treatment using a 4-point scale: 0, no redness; 1, just perceptible redness; 2, redness with well-defined border; 3, bright red and indurated reaction.
Patients scored the pain in the treatment areas before and immediately after daylight exposure as well as after the first 45 and 90 min during exposure. Pain was assessed using a numerical rating scale (NRS) ranging from 0 to 10, in which 0 = no pain and 10 = worst imaginable pain.
PpIX fluorescence was measured using a hand-held fluorescence photometer (FluoDerm; Dia-Medico, Gentofte, Denmark) before application of MAL (background fluorescence) and just before daylight exposure (20). This made it possible to calculate PpIX accumulation after 30 min of MAL application. PpIX fluorescence was measured in arbitrary Fluoderm Units (FDU).
Daylight illuminance in lux was measured at the beginning and end of illumination using a lux meter (Luxmeter 540, Testo AG, Lenzkirch, Germany).
Sample size requirement was based on a previous study investigating lesion response rates to PDT (21). The standard deviation (SD) of total lesion response rate in that study was 17.6. Aiming for a significance level of 5% and a power of 80%, based on the assumption that the smallest clinically relevant mean difference in lesion response is 15%, we calculated that at least 22 patients needed to be included in the study.
Statistical analysis was performed in IBM SPSS statistics version 22.0.0 (IBM, Armonk, NY, USA). Parametric tests were used because data were normally distributed. Lesion response rates for AKs and PpIX fluorescence were calculated for the treatment areas of each patient and compared using the paired t-test. Pain and erythema in the treatment groups were compared using Pearson’s χ2 test. The correlation between overall lesion response rate and 5-FU consumption was calculated using the Pearson correlation test, whereas linear regression was used to analyse the association between illuminance and lesion response rates. p-values < 0.05 were considered significant.
A total of 24 patients (16 men, 8 women) with a mean age of 73.3 (range 52–87) years were included and completed the study. The patients had a total of 799 AKs, and lesion characteristics were similar in the 2 treatment groups in terms of number and severity grade (Table I).
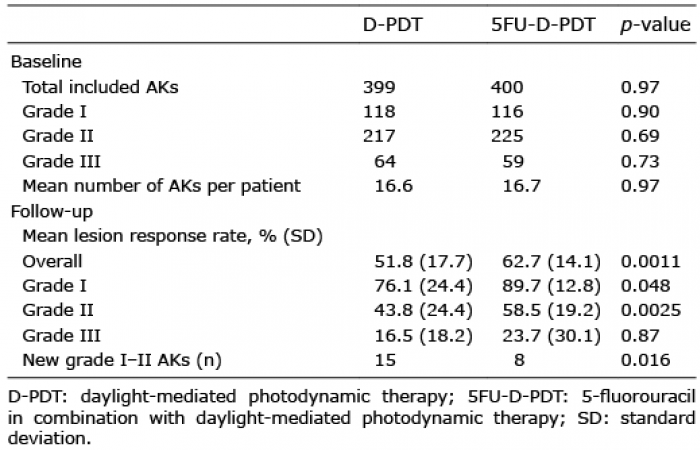
Table I. Baseline characteristics of the included actinic keratoses (AKs) and relevant outcome measures at 3-month follow-up
Complete lesion response rate was defined as the proportion of lesions with complete response for each patient. Mean complete response rates at 3-month follow-up are shown in Table I. Specific response rates for grade I and grade II AKs were significantly in favour of sequential treatment (p = 0.048 and p = 0.0025, respectively). Like-wise, overall mean lesion response was significantly higher for 5FU-D-PDT (62.7%) than for D-PDT (51.8%) (p = 0.0011) (Table I). For grade III AKs the response rate was higher for 5FU-D-PDT (23.7%) than for D-PDT (16.5%), but this difference was not significant (p = 0.87). At follow-up significantly more new grade I–II AKs had developed after D-PDT than after 5FU-D-PDT (p = 0.016).
No difference was found in the degree of erythema one day after PDT between the 2 treatment groups (p = 0.27) (Table II) and the median maximum pain score during PDT was 0 for both treatment regimens (p = 1.0). Furthermore, mean PpIX accumulation after 30 min MAL incubation was similar for D-PDT (0.74 FDU) and 5FU-D-PDT (0.87 FDU) (p = 0.61). Patients did not report pain or discomfort during the 7-day pretreatment period with 5-FU. Moreover, no unexpected adverse events occurred in the patients during the trial period.
Table II. Adverse events in relation to photodynamic therapy
Mean daylight illuminance during treatment was 36,477 lux (range 1,322–94,234 lux). Overall lesion response rates for 5FU-D-PDT and D-PDT were independent of illuminance (p = 0.52 and p = 0.93, respectively) (Fig. 1). During the 7 days of pretreatment mean consumption of 5-FU cream was 6.5 g (range 2.1–14.3), corresponding to 0.46 g per application. 5-FU consumption was not correlated with overall response rate (p = 0.27).
Fig. 1. Correlation between daylight illuminance and overall lesion response rates for daylight-mediated photodynamic therapy (D-PDT) and combination treatment with 5-fluorouracil and daylight-mediated photodynamic therapy (5FU-D-PDT). Overall lesion response rates were independent of daylight illuminance for both regimens (p = 0.93 and p = 0.52, respectively).
This study clearly shows that sequential treatment with 5% 5-FU and daylight-PDT is superior to daylight-PDT alone. Thus, overall clearance rates, as well as specific response rates, for grade I–II AKs were significantly higher after combination therapy (Table I). In fact, combination therapy yielded clearance rates for grade I (89.7%) and grade II AKs (58.5%) that are equal or superior to those found in daylight-PDT studies for AKs on the face and scalp. In 3 daylight-PDT studies with similar study design to ours lesion response rates for grade I AKs ranged from 75.9% to 89.2% (22–24), whereas response rates for grade II AKs were reported to be 36.0% (22) and 61.2% (24), respectively. In view of these findings our results are encouraging because an improvement in PDT efficacy on the extremities is much needed. Until now no prospective studies have investigated the efficacy of daylight-PDT for AKs on the extremities in immunocompetent patients, but studies with conventional MAL-PDT report markedly lower response rates in acral skin regions than for the face and scalp (5, 8). Our results suggest that pretreatment with 5-FU for 7 days can narrow or even close this gap in efficacy.
For over 50 years topical application of 5-FU has been used in dermatology primarily for treating AK, Bowen’s disease and basal cell carcinoma (25, 26). Topical 5-FU inhibits the enzyme thymidylate synthetase, which is integral in DNA and RNA synthesis (27). This leads to decreased cell proliferation and apoptosis, particularly in dysplastic cells (28). The efficacy of 5-FU treatment of AKs is high, and recently 5% 5-FU cream was ranked as the treatment of choice in a network meta-analysis that analysed 8 interventions for AK (29). However, adverse events, such as inflammation, oozing and crusting, are drawbacks when utilizing the standard regimen of 2 daily applications for 3–4 weeks. This led researchers to combine short-term application of 5-FU with PDT in hope of achieving an additive effect as well as fewer adverse events (16–18). Thus, Tanghetti et al. (18) and Gilbert (16) applied 5% 5-FU for 5–7 days before performing 5-aminolevulinic acid (ALA)-PDT in treatment of facial AKs, whereas Martin (17) used 0.5% 5-FU cream for 7–10 days prior to ALA-PDT in 3 patients with multiple AKs. Interestingly, all studies reported that sequential treatment enhanced PDT efficacy for AKs. The reasons for this are unknown, but Gilbert proposed that pretreatment with 5-FU could enhance ALA absorption and/or increase blood flow to the AK tissue, making more oxygen available for conversion into cytotoxic singlet oxygen during PDT (16). We did not find evidence of increased MAL absorption, as PpIX accumulation before daylight exposure was similar in the 2 treatment groups. However, this is probably because MAL was only applied for 30 min before we measured PpIX accumulation and we cannot exclude the possibility that MAL absorption could be enhanced with longer application times. Unfortunately, it is difficult to compare our lesion response rates with the above-mentioned studies because we used MAL as photosensitizer and treated AKs on the hands, whereas they used ALA and treated AKs on the face or in locations that were not further specified.
For a combination regimen to be successful it is critical that adverse events are limited and that the treatment protocol is easy to adhere to. Our sequential treatment regimen was well tolerated and neither pain during PDT nor post-treatment erythema was worse with combination therapy (Table II). Regrettably, we did not assess erythema before illumination, but we found that pretreatment with 5-FU only caused minimal erythema in a few patients. Moreover, patients generally stated that the short treatment duration of 5-FU for 7 days was easy to follow. The fact that neither cream consumption nor mean illuminance during PDT correlated with treatment efficacy further suggests that this regimen is stable and should be easy to implement.
The increasing incidence of non-melanoma skin cancer and AKs places effective treatment modalities in high demand (30, 31). Our study builds on the growing evidence that combination therapy may be an effective way to enhance the effect of PDT for AK. In recent years researchers have successfully combined PDT with imiquimod (12, 13), diclofenac (14), ingenol mebutate (15), and fractional laser therapy (32). Studies like these are vital for the future development of PDT. Most current PDT studies focus on treating thin AKs on the face and scalp where efficacy is high, but we believe that more emphasis should be placed on improving treatment for grade II–III AKs and/or nodular basal cell carcinoma, for which response rates are inferior.
It is a limitation of the present study that our efficacy evaluation was not blinded. Furthermore, the study would have benefited from having standard monotherapy with 5% 5-FU regimen as third comparator in order to estimate the true effect of combination therapy. However, a previous randomized paired comparison between ALA-PDT and standard 5% 5-FU treatment of AKs on the hands showed that treatment efficacy was similar in the 2 groups (6).
Sequential treatment with 5-FU cream and daylight-PDT was significantly superior to daylight-PDT alone for treating AKs on the hands. The treatment protocol was easy for the patients to adhere to and did not increase adverse events. Combination therapy is a promising method to improve treatment of AKs on the extremities, which are notoriously difficult to treat.
Conflicts of interest. HCW, SRW and CSM have received speaker honoraria from Galderma. CVN and IMH have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize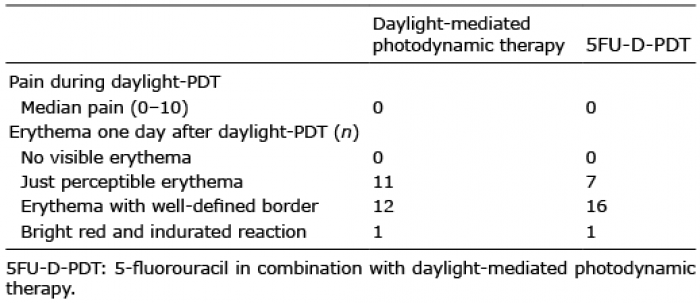 Click to show fullsize
Click to show fullsize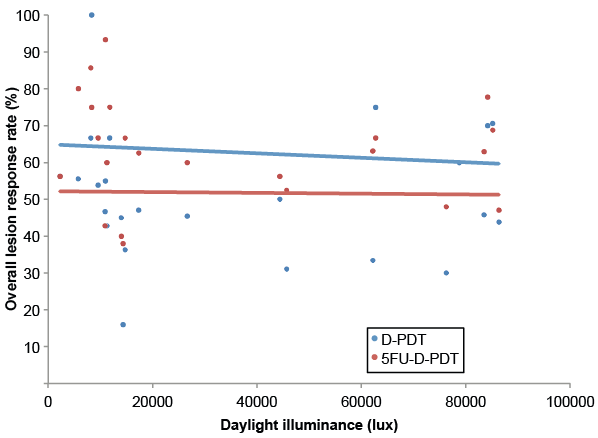 Click to show fullsize
Click to show fullsize