


1Department of Dermatology and Allergology, Ludwig-Maximilian University, Munich, Germany, 2Department of Dermatology, Ankara 29 May?s Government Hospital, Ankara, Turkey, 3Department of Dermatology, Allergology, and Venereology and 4Lübeck Institute of Experimental Dermatology (LIED), University of Lübeck, Lübeck, Germany
Linear IgG deposits along the basement membrane of adnexa has been proposed to be useful in the diagnosis of bullous pemphigoid (BP), but no controlled studies have been performed. This study evaluated linear IgG fluorescence of the basement membrane of sweat gland ducts (SGD) and other adnexa in perilesional biopsies from patients with BP (n = 64) and controls (n = 82), using direct immunofluorescence microscopy. Fluorescence intensity was graded semi-quantitatively.
Positive SGDs were found in 58 (90.6%) patients with BP and 44 (53.7%) controls, a statistically significant difference (p < 0.0001). The sensitivity of positive SGDs for BP was high (90.6%), but the specificity was low (46.3%). Only strong fluorescence intensity was associated with high specificity. In conclusion, positive
SGDs in direct immunofluorescence microscopy are highly sensitive for BP; however, only strong fluorescence has acceptable specificity. Weak positivity of SGDs
without linear fluorescence of the epidermal basement membrane may not be sufficiently specific for BP.
Key words: bullous pemphigoid; sweat gland ducts; immuno-fluorescence; diagnostics.
Accepted Jan 12, 2017; Epub ahead of print Jan 17, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: In Sinem Ba?c?, Department of Dermatology and Allergology, Ludwig-Maximilian University, Frauenlobstr. 9–11, DE-80337 Munich, Germany. E-mail: Bagci.Isin_Sinem@med.uni-muenchen.de
Bullous pemphigoid (BP) is the most common auto-immune blistering disease of the skin. Diagnosis of BP relies on histopathological examination, including direct immunofluorescence microscopy (DIF) on perilesional skin biopsy specimens, in addition to detection of circulating autoantibodies by indirect immunofluorescence microscopy and enzyme-linked immunoassays (ELISAs) (1, 2).
DIF is a specific, and the most sensitive, diagnostic test for BP (3, 4). It reveals linear IgG and/or complement C3 deposition at the dermal–epidermal junction. Besides the classical examination of the epidermal basement membrane (BM), recent reports have shown that the immunofluorescence of the BM of sweat glands and hair follicles might have a diagnostic relevance in autoimmune blistering diseases (5, 6).
However, previous studies have not analysed the operating characteristics of adnexal fluorescence.
The objectives of this study were to evaluate the immunofluorescence pattern and intensity of the sweat gland ducts (SGD) and other adnexal structures in BP and to compare them with a control group in order to assess their diagnostic performance.
A single-centre, case-control study was conducted on biopsy samples from 64 BP and 82 control patients at the Department of Dermatology and Allergology, Ludwig-Maximilian University, Munich, Germany. This type of non-interventional study on laboratory samples that were produced for routine diagnostic purposes does not require ethical approval in Germany.
Archived frozen cutaneous biopsy specimens of 51 patients with BP who had been diagnosed in 2015 were re-cut and re-stained; in addition, 13 further patients who were diagnosed during the course of the study (January–April 2016) were included in the BP group. The diagnosis was based on the integration of clinical, histological, immunopathological and serological findings. Inclusion criteria were a clearly visible, continuous, linear IgG fluorescence along the epidermal basement membrane, the presence of SGDs in the sections, and the evident diagnosis of BP (4). Control DIF sections were obtained from 82 patients with various other skin disorders diagnosed in 2016, in which BP could be clearly ruled out. Patients lacking a definite diagnosis or SGDs in the sections were excluded.
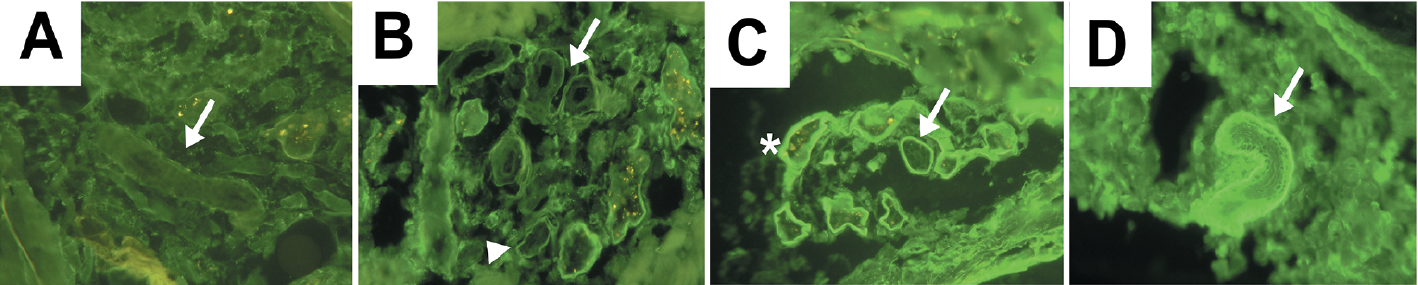
The in vivo bound IgG autoantibodies were detected by DIF in the patients’ skin. All sections were stained with fluorescein isothiocyanate (FITC)-labelled goat anti-human IgG (#F1641, Sigma-Aldrich, St Louis, MO, USA) diluted 1:30 in phosphate-buffered saline (PBS) for 30 min at room temperature in a dark, humid chamber. No blocking was used. Each section was examined by the first author for the fluorescence pattern and intensity of IgG in the epidermis, SGDs, hair follicles, and sebaceous glands, and then reviewed by the last author. SGDs in papillary, mid and deep dermis were assessed separately. The intensity of the fluorescence was semi-quantitatively graded between 0 and 4 (0, no fluorescence; 4, strongest fluorescence). Examples of each intensity grade are shown in Fig. 1.
Fig. 1. Semi-quantitative grading of the fluorescence intensity of the sweat gland ducts (SGDs). (A) Intensity 0 SGD without fluorescence of the basement membrane (BM) (arrow). (B) Linear staining along the BM of intensity 1 (arrow) and 2 (arrow head) SGDs. (C) More prominent fluorescence of the BM of intensity 3 SGDs (arrow) next to the sweat glands (asterisk). (D) Strongest fluorescence of the BM of intensity 4 SGD (arrow).
Some skin sections from patients with BP were selected randomly and stained with anti-BP180 and anti-BP230 monoclonal antibodies (HD18 described elsewhere (7) and Cosmo Bio, CAC-NU-01-BP1, respectively) to demonstrate the presence of BP180 and BP230 proteins in the adnexal BM. The monoclonal antibodies were diluted 1:1 and 1:10 in PBS, respectively, and incubated for 60 min at room temperature on the sections. After washing, bound antibodies were detected by FITC-labelled polyclonal antibodies directed against mouse IgG (#sc-3699 Santa Cruz Biotechnology, Dallas, TX, USA).
For comparison of intensities, Mann–Whitney’s non-parametric, unpaired, 2-tailed test was performed. GraphPad Prism version 4.03 for Windows (GraphPad Software, San Diego, CA, USA) was used for calculations.
Sections from 64 patients with BP (30 females, 34 males; mean age 78, range 8–96 years) were examined and compared with 82 control patients (43 females, 39 males, mean age 63, range 18–90 years). Linear IgG fluorescence along the BM of SGDs and other adnexa was assessed in both groups. As an example positive, negative and false positive immunofluorescence of SGDs are shown in Fig. 2.
Fig. 2. Assessment of linear IgG fluorescence along the basement membrane (BM) of sweat gland ducts (SGDs) in bullous pemphigoid (BP) and control sections. (A) Negative SGDs (arrows) in a control section. (B) Positive SGD (arrows) with strong fluorescence in a BP section. (C) False–positive SGD (arrow) with weak fluorescence in a control section.
Sections stained with anti-BP180 and anti-BP230 monoclonal antibodies showed linear fluorescence along the BM of the epidermis, SGDs, sweat glands and hair follicles. As an example BP180 and 230 immunofluorescence of SGDs and sweat glands are shown in Fig. 3.
Fig. 3. Anti-BP180 and anti-BP230 staining of bullous pemphigoid (BP) sections. Linear staining along the basement membrane of sweat gland ducts (asterisk) and sweat glands (arrows) with (A) anti-BP180 and (B) anti-BP230.
In the whole dermis. As mentioned above, all BP samples showed linear IgG fluorescence along the epidermal BM, whereas control skin samples did not. SGDs were observed as round, oval or tubular structures in all layers of dermis. They were lined by 2 layers of monomorphic cuboidal cells, surrounding a narrow lumen. In contrast, sweat glands occurred only in the deep dermis, were composed of a single cell layer around a wider lumen and were differentiated from the ducts by the lipofuscin granules inside the lumina (Fig. 4).
Fig. 4. Differentiation of sweat gland ducts (SGDs) and sweat glands. (A) Appearance of SGDs (asterisks) and sweat glands (arrows) in haematoxylin-eosin- stained sections. (B) SGDs appear as round or oval structures lined by monomorphous keratinocytes around a narrow lumen in direct immunofluorescence (DIF) (asterisks). Sweat glands are differentiated from the SGDs by the lipofuscin granules, which are seen as orange-colored bright spots inside their lumina (arrows).
Fifty-eight (90.6%) patients with BP and 44 (53.7%) controls showed linear deposition of IgG along the BM of the SGDs. Fluorescence intensity of SGDs in DIF was significantly higher in patients with BP than in controls (p < 0.0001) (Fig. 5A).
Fig. 5. Comparison of the fluorescence intensity of sweat gland ducts (SGDs) between bullous pemphigoid (BP) and control patients. (A) The fluorescence intensity of the basement membrane (BM)of SGDs was significantly higher in BP patients compared with the controls in the whole dermis, (B) papillary dermis, (C) mid-dermis, (D) and deep dermis. BP patients also had a significantly higher fluorescence along the BM of (E) hair follicles and (F) sebaceous glands comparing to the controls. ***Significant difference, p < 0.001.
The sensitivity and specificity of positive SGDs for BP was 90.6% and 46.3%, respectively. With increasing intensity of the fluorescence, the sensitivity decreased, whereas the specificity increased. Positive SGDs with intensity grades 3 and 4 showed the lowest sensitivity (31.2%) and the highest specificity (97.5%) (Fig. 6). Fluorescence intensity of SGDs did not correlate significantly with the patients’ circulating BP180 and BP230 autoantibody titres.
Fig. 6. Sensitivity (A) and specificity (B) of sweat gland ducts (in whole, papillary, mid- and deep dermis), hair follicles and sebaceous glands for diagnosis of bullous pemphigoid (BP) (64 BP and 82 control patients).
In the papillary dermis. Within the papillary dermis, 34 (53.1%) patients with BP and 51 (62.2%) controls had SGDs. Among patients with BP, 5 (14.7%) showed no fluorescence of the ductal BM, whereas 29 (85.3%) specimens showed linear fluorescence with intensity grades 1, 2 and 3 in 22 (64.7%), 6 (17.6%), and 1 (2.9%) cases, respectively. Among control subjects, 39 (76.5%) showed no fluorescence in the ductal BM, whereas 12 (23.5%) specimens showed linear fluorescence with intensity grades 1 and 2 in 11 (21.5%) and 1 (2%) cases, respectively. The fluorescence intensities of SGDs in papillary dermis were significantly different between patients with BP and controls (p < 0.0001) (Fig. 5B). Positive SGDs in the papillary dermis with any intensity of fluorescence showed the highest sensitivity (89.2%) and those with intensities 3 and 4 the highest specificity (100%) to detect BP (Fig. 6).
In the mid-dermis. Within the mid-dermis, 48 (75%) patients with BP and 57 (69.5%) controls had SGDs. Eight (16.7%) BP specimens displayed no fluorescence, whereas 40 (83.3%) patients showed linear fluorescence of the ductal BM with intensity grades 1, 2, 3 and 4 in 27 (56.3%), 7 (14.6%), 3 (6.2%), and 3 (6.2%) cases, respectively. Among control subjects, 43 (75.4%) patients displayed no fluorescence, whereas 14 (24.6%) specimens showed linear fluorescence of the ductal BM with intensity grades 1, 2, 3 in 9 (15.8%), 4 (7%) and 1 (1.8) cases, respectively. The fluorescence intensities of SGDs in mid-dermis were significantly different between patients with BP and controls (p < 0.0001) (Fig. 5C). The sensitivity and specificity of the positive SGDs in mid-dermis with any intensity of fluorescence were 83.3% and 75.9%, respectively. SGDs with intensities 3 and 4 had 98.3% specificity in mid-dermis; however, the sensitivity was 12.5% (Fig. 6).
In the deep dermis. Within the deep dermis, 47 (73.4%) patients with BP and 65 (79.2%) controls had SGDs. Among patients with BP, 8 (17%) showed no fluorescence, whereas 39 (83%) patients showed linear fluorescence of the ductal BM with intensity grades 1, 2, 3 and 4 in 10 (21.3%), 12 (25.5%), 13 (27.7%) and 4 (8.5%) cases, respectively. Among control subjects, 29 (44.6%) showed no fluorescence, whereas 36 (55.4%) patients showed positive fluorescence with intensity grades 1, 2 and 3 in 25 (38.5%), 10 (15.4%) and 1 (1.5%) cases, respectively. The fluorescence intensities of SGDs in the deep dermis were significantly different between patients with BP and controls (p < 0.0001) (Fig. 5D). Positive SGDs in the deep dermis with any intensity of fluorescence had 83% sensitivity. The specificity was lower (43.9%) than SGDs in other levels of the dermis, but it increased with stronger fluorescence and SGDs with intensities 3 and 4 showed 98.5% specificity to detect BP (Fig. 6).
Twenty (31.2%) BP samples contained hair follicles in the sections with intensity grades 0, 1, 2, 3 and 4 in 5 (25%), 4 (20%), 8 (40%), 1 (5%) and 2 (10%) cases, respectively. On the other hand, 33 (40.2%) controls had hair follicles with intensity grades 0, 1, and 2 in 29 (87.9%), 3 (9.1%) and 1 (3%) cases, respectively. The fluorescence intensities of hair follicles were significantly different between patients with BP and controls (p < 0.0001) (Fig. 5E). The sensitivity and specificity of the positive hair follicles with any intensity of fluorescence were 75% and 87.9%, respectively. The sensitivity decreased in hair follicles with intensities 3 and 4 (15%), but they showed the highest specificity (100%) (Fig. 6).
Fourteen (21.8%) patients with BP had sebaceous glands in the sections with intensity grades 0, 1, 2, 3 and 4 in 2 (14.3%), 7 (50%), 3 (21.4%), 1 (7.1%) and 1 (7.1%) cases, respectively. On the other hand, 19 (23.2%) controls had sebaceous glands with intensity grades 0, 1, 2, and 3 in 13 (68.4%), 4 (21.1%), 1 (5.3%) and 1 (5.3%) cases, respectively. The fluorescence intensities of sebaceous glands were significantly different between patients with BP and controls (p = 0.0045) (Fig. 5F). Positive sebaceous glands with any intensity of fluorescence had 85.7% sensitivity and 68.4% specificity. The specificity reached 94.7% in sebaceous glands with intensities 3 and 4 (Fig. 6).
A few reports have already demonstrated the immunoreactivity of hair follicles, sweat glands and ducts in dermatitis herpetiformis (8), pemphigus, and BP (9, 10). In addition, recent studies have indicated that the immunofluorescence of SGDs and other adnexal structures might have a diagnostic importance in autoimmune bullous diseases. For instance, Lehman & Camilleri (5) reported that folliculosebaceous units and sweat apparatus (sweat glands and ducts) show high sensitivity in various immunobullous disorders. Lehman et al. suggested that the immunofluorescence pattern of adnexal structures might have a diagnostic value in the absence of interpretable findings in the epidermis or dermal–epidermal junction. Similarly, a recently published study by Zhou et al. (6) reported that sensitivity of immunofluorescence of eccrine apparatus (eccrine sweat glands and ducts) is similar to that of the epidermis and hair follicles in both pemphigus vulgaris and BP. However, to our knowledge, no studies have been performed regarding the operating characteristics of SGD fluorescence in autoimmune blistering diseases, and no samples from control patients were examined in previous studies.
In our study, BM positivity of SGDs was significantly more common in each level of dermis in BP compared with the controls, especially within the mid and deep dermis. In addition, BM of hair follicles and sebaceous glands were more commonly positive in patients with BP than controls. These findings support the results of previous studies (5, 6).
Unlike previous studies, we also examined the fluorescence intensities and the localization of SGDs. IgG fluorescence of the BM of SGDs in each level of dermis, hair follicles, and sebaceous glands were significantly different between patients with BP and controls. IgG deposits along the BM of SGDs in the papillary dermis showed higher sensitivity compared with those in the mid and deep dermis. Although positive SGDs in papillary dermis showed a higher specificity than those in other levels of dermis, only fluorescence of strong intensity could reach an acceptable specificity. As false-positive SGDs, hair follicles, and sebaceous glands occurred commonly in control patients, but the intensity of false-positive signal was relatively low, we can conclude that linear BM fluorescence of solely the adnexal BM is relevant only if the intensity of the fluorescence reaches at least grade 3.
We observed that DIF evaluation of SGDs is more useful than that of sweat glands, since sweat glands frequently display positive fluorescence of strong intensity in most of the sections regardless of the diagnosis. We re-stained 5 randomly selected sections with a different secondary antibody, FITC-labelled rabbit anti-human IgG antibody (γ chain) (Dako-Biozol, Eching, Germany), in order to assess whether the distinct fluorescence patterns of sweat glands were related to the reagent we used in the study, but found no difference between the 2 different antibodies. A recent report supported our observation, demonstrating the non-specific autofluorescence of haematoxylin-eosin stained eccrine sweat glands under the fluorescence microscope. Autofluorescence of SGDs was not observed (11). Thus, neither the presence of positive sweat glands, nor their intensity of fluorescence has a diagnostic value for BP. Therefore, evaluation of the SGDs with their localization and fluorescence intensity is recommended for the diagnosis of BP instead of evaluation of the whole sweat gland apparatus (sweat glands and ducts).
Although IgG deposits in the BM of SGDs show a high sensitivity for BP, there is no evidence to suggest that either sweat glands, ducts or sweat are involved in the pathogenesis of BP. Dai et al. (12) reported a strong in situ expression of IL-31 in the SGDs and a weaker expression in the sweat glands in normal skin. Furthermore, it has been demonstrated that eccrine sweat contains IL-1α, IL-1β, IL-8, and IL-31, and these proinflammatory cytokines are involved in the activation of epidermal keratinocytes (12, 13) indicating that sweat apparatus is not only important in thermoregulation but also has a role in cutaneous inflammation.
Although the aetiology remains unknown, BP has been reported to be induced by some drugs, virus infections or physical factors (14). Excretion of drugs into eccrine sweat is a known phenomenon, which may result in several drug-related eccrine disorders (15). Eccrine acrosyringium has been shown to express class II major histocompatibility complex antigens which may play an immunological role against external agents (16). Therefore, an immunological interaction between the drugs and sweat apparatus is possible. We demonstrated that BP180 and BP230 molecules are present in the adnexal BMs. This finding supports the hypothesis that loss of immune tolerance against BP180 could originate from the sweat glands or SGDs, where certain drugs or other haptens excreted by sweat would be able to bind to BP180 and induce autoimmune reaction.
A previous report (6) and our clinical experience show that some patients with BP can display only positive linear fluorescence along the BM of SGDs without the diagnostic linear staining of the epidermal BM; however, it is not yet understood whether isolated SGD positivity is an early diagnostic predictor of BP and whether it can be a reliable diagnostic sign for BP.
In conclusion, linear deposits of IgG along the BM of SGDs are highly sensitive for BP in each level of dermis; however, only strong fluorescence has acceptable specificity. SGD positivity in the upper dermis was found to be more BP-specific than in the lower dermis. Thus, evaluation of the localization and the intensity of adnexal IgG fluorescence is important, and SGD immunoreactivity may have diagnostic relevance in BP. However, further controlled studies are necessary to recommend SGD fluorescence as the basis for diagnosis of BP, even with strong signal intensity.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize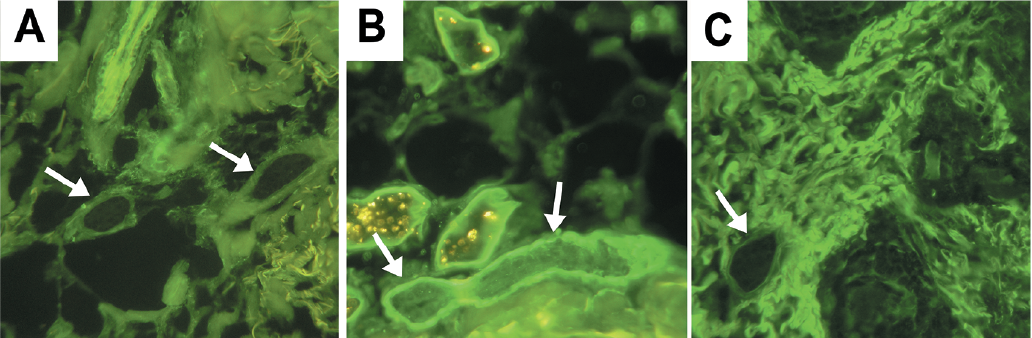 Click to show fullsize
Click to show fullsize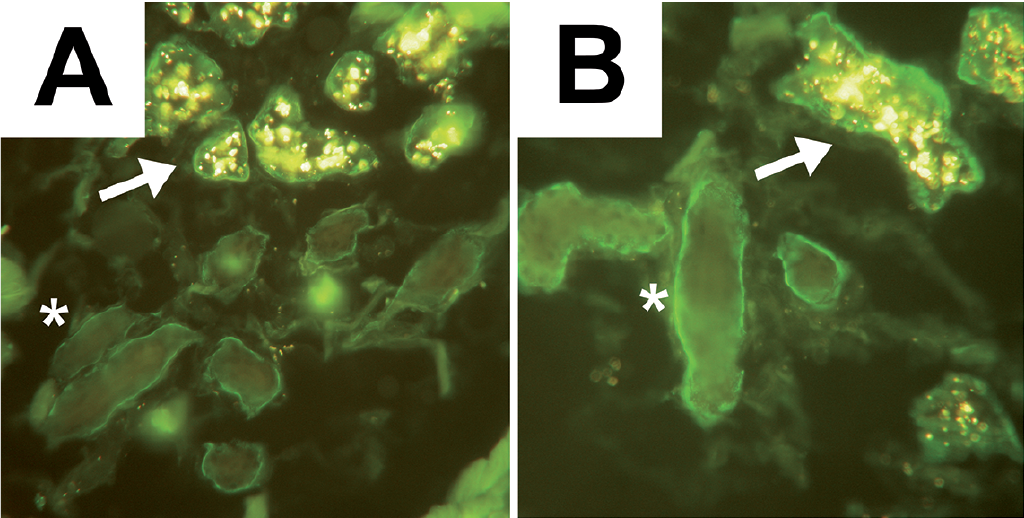 Click to show fullsize
Click to show fullsize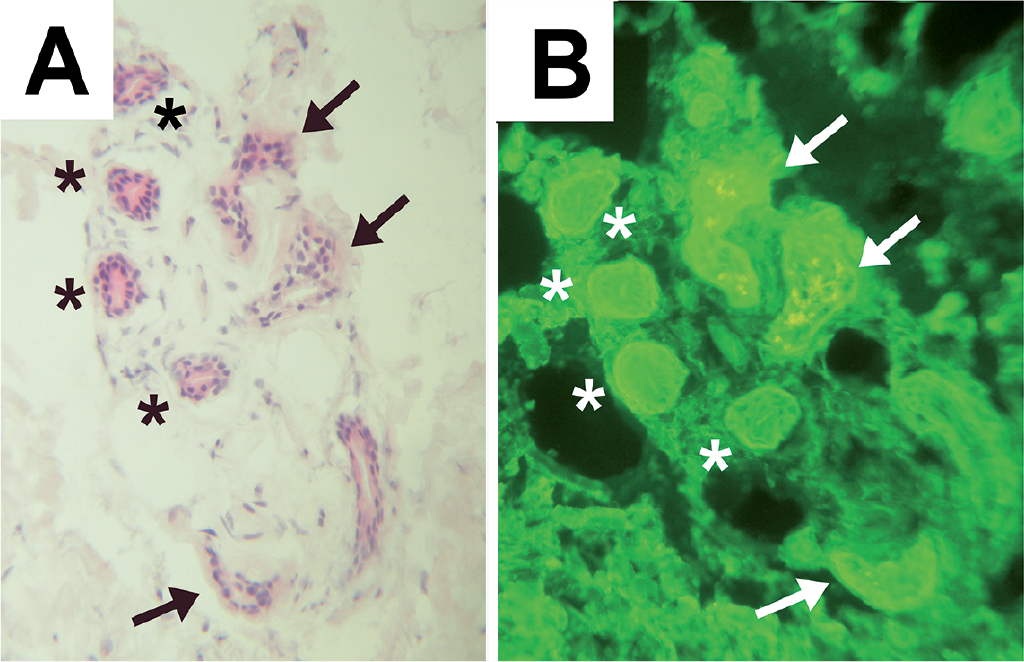 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize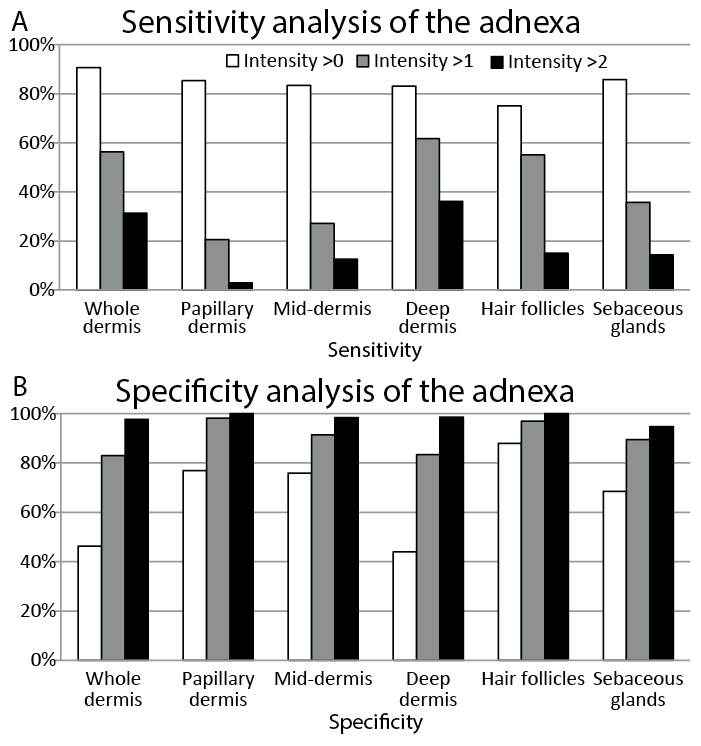 Click to show fullsize
Click to show fullsize