


1Department of Dermatology, Venereology and Allergology, University Medical Center Mannheim, Heidelberg University, Mannheim, 2Dermatological Practice Dr. Krekel, Speyer, 3Department of Dermatology and Venereology, University Medical Center, Hamburg-Eppendorf, and 4Department of Dermatology and Phlebology, Vivantes Klinikum im Friedrichshain, Landsberger Allee 49, DE-10249 Berlin, Germany. *E-mail: wiebke.ludwig-peitsch@vivantes.de
Accepted Jan 24, 2017; Epub ahead of print Jan 25, 2017
Lupus miliaris disseminatus faciei (LMDF), synonymously termed acne agminata (1), is an uncommon granulomatous inflammatory disease usually affecting the central face and the eyelids (1–3). Rare extrafacial manifestations have been reported (1, 3–7). We present here a case of LMDF with involvement of the face, scalp and axillae and provide a summary on the characteristics of the disease and treatment options.
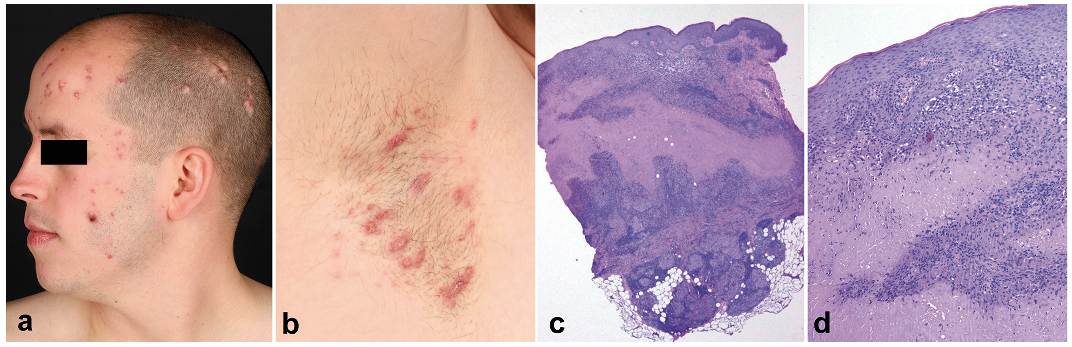
A 28-year-old man presented with a 3-month history of asymptomatic papules, nodules and pustules, which had initially appeared on his eyelids and in the axillae and subsequently spread over his face. Treatment with different topical agents, including antibiotics, nystatin, aciclovir and glucocorticoids, as well as oral doxycycline and oral valaciclovir, had been ineffective. The patient had no systemic symptoms or concomitant diseases and did not take any medications. He did not have any history of acne or rosacea, and denied use of aluminium-containing antiperspirants. Clinical examination showed multiple distinct red-brown, sometimes yellowish, papules and nodules, sized 2–10 mm, on the scalp, forehead, glabella, upper and lower eyelids, cheeks and chin (Fig. 1a) as well as in both axillae (Fig. 1b) with a light brown-yellowish infiltrate on diascopy. Diffuse erythema and telangiectasia were absent. Histopathological examination revealed dermal epithelioid cell granulomas with central caseating necrosis (Fig. 1c, d). Microscopy for pathogens with periodic acid–Schiff (PAS), Grocott and Ziehl-Neelsen stains, as well as cultures for Mycobacterium tuberculosis and atypical mycobacteria were negative. A bacterial swab yielded Pseudomonas aeruginosa. Laboratory examinations including serum levels of angiotensin-converting enzyme and tuberculosis test with interferon gamma release assay (QuantiFERON-TB test, QIAGEN, Hilden, Germany) were unremarkable. Based on clinical and histopathological findings a diagnosis of LMDF with axillary involvement was established. Compatible with the results of antimicrobial susceptibility testing, a treatment attempt was made with ciprofloxacin 500 mg twice daily for 2 weeks, but without success. Subsequently isotretinoin 30 mg/day (0.4 mg/kg) was initiated and continued for one year with regular laboratory monitoring. This resulted in clearing of the lesions on the face and scalp with some residual scars, but the axillary lesions remained.
Fig. 1. Clinical and histopathological findings. (a, b) Multiple red-brown and yellowish papules and nodules in the face, on the scalp and in the axilla. (c, d) Haematoxylin-eosin stained skin biopsy specimen from the face showing dermal epithelioid cell granulomas with central areas of caseating necrosis. Magnification: (c, survey) ×20 or (d, detail) ×100. A biopsy from the axilla yielded identical findings. Written permission is given to publish these photographs.
LMDF usually affects young adults of both sexes, but it has also been reported in children (8) and elderly patients (9, 10). It typically presents with yellowish-brown dome-shaped papules and pustules localized in the central face, commonly involving the eyelids (1–3). Moreover, extrafacial lesions in the axillae, scalp, trunk, genitalia, neck, hands and legs have been described (1, 3–7). They may occur in addition to facial lesions (1, 3, 4, 6, 7) or, rarely, as the only manifestation of LMDF (4, 5). To make allowance for lesions in non-facial sites Nemer & McGirt recently suggested renaming LMDF “lupus miliaris disseminatus” (6).
The papules have a yellowish-brown (‘’apple-jelly’’) infiltrate on diascopy. On histopathological examination they are characterized by a superficial granulomatous inflammation and perifollicular epithelioid cell granulomas with central necrosis, but findings are dependent on the stage of the disease (11). The aetiology and pathogenesis of LMDF remain unclear. It has been considered to be a form of cutaneous tuberculosis, tuberculoid or sarcoidosis, but work-ups for these diseases performed in several case series did not support any associations (9, 11, 12), and neither does our case. Furthermore, Propionibacterium acnes (13) and Demodex folliculorum were thought to play a role in the pathogenesis of LMDF, and it was speculated to be a variant of granulomatous rosacea (2, 14). Indeed, LMDF shares similarities with granulomatous rosacea, but it typically occurs at a younger age. Furthermore, it can be distinguished from granulomatous rosacea by lack of erythema and telangiectasia and by the presence of caseating necrosis within the granulomas (3). In order to clearly differentiate LMDF from other conditions Skowron et al. (9) suggested designating it “facial idiopathic granulomas with regressive evolution (FIGURE)”.
After a sudden onset and a chronic course over several months or years LMDF often heals spontaneously (7, 12). However, treatment is required to prevent scarring and to reduce the duration of this sometimes disfiguring disease (2). Standard treatment recommendations and controlled trials are lacking. Topical steroids are known to be ineffective. Several other approaches, including intralesional or systemic corticosteroids, topical tacrolimus, tetracyclines, metronidazole, erythromycin, dapsone, anti-tuberculous antibiotics, isotretinoin, chloroquine and clofazimine, have been attempted, with variable results (3, 4, 6–8, 10, 11). Combination regimens of oral antibiotics and topical tacrolimus were efficient in some cases (5, 8). In addition, there are reports of successful laser therapy of the lesions and scars with 1,565-nm non-ablative fractionated laser (15), 1,450-nm diode laser or carbon dioxide laser. The papules and pustules on the face and scalp of our patient resolved upon treatment with isotretinoin; however, clearance of the axillary lesions was not achieved. The patient did not desire further treatment and wanted to await the spontaneous course.
The patient is acknowledged for permission to share his case and photographs.
Conflicts of interest. M-LS conducted clinical trials for Abbvie, Eli Lilly, Merck, Novartis, Boehringer Ingelheim and UCB Pharma, obtained honoraria from Janssen-Cilag, and received financial support for participation in conferences from Abbvie, ALK-Abello, Biogen Inc., Janssen-Cilag and MSD. MS received financial support for participation in a conference from Meda. JS has no conflicts of interest to declare. AS performed clinical trials for Abbvie, Boehriner Ingelheim, Celgene, MSD, Novartis, Eli Lilly and Pfizer, received honoraria from Janssen-Cilag and Novartis, and support for participation in conferences from Abbvie, Celgene, Janssen-Cilag, Novartis and Pfizer. SG obtained honoraria as Editor-in-Chief of the Journal of the German Dermatological Society (JDDG) and support for conferences from Abbvie, ALK-Abello, Alma Lasers, ARC Lasers, Asclepion, BMS, Dermasence, Eli Lilly, GSK, Interlac, Janssen-Cilag, L’Oreal, La Roche Posay, LEO Pharma, Medac, Merck, MSD, Novartis, P&M Cosmetics, Pfizer, Roche and Stiefel. WKP served as investigator for Abbvie, Boehringer Ingelheim, Eli Lilly, Janssen-Cilag, Merck, Novartis, Pfizer and UCB Pharma, was member of an advisory board of Abbvie, Eli Lilly, LEO Pharma, MSD and Novartis, obtained honoraria from ALK-Abello, Abbvie, Janssen-Cilag, MSD, Novartis and Roche and received support for conferences from Abbvie, ALK-Abello, Alma Lasers, ARC Lasers, Asclepion, BMS, Celgene, Dermasence, Eli Lilly, GSK, Interlac, Janssen-Cilag, L’Oreal, La Roche Posay, LEO Pharma, Medac, Merck, MSD, Novartis, P&M Cosmetics, Pfizer, Roche and Stiefel. None of the conflicts of interest reported is relevant for the content of this manuscript.


 Click to show fullsize
Click to show fullsize