


1Department of Dermatology and Allergy, and 2Department of Cardiology, Herlev and Gentofte Hospital, University of Copenhagen, DK-2900 Hellerup, Denmark. *E-mail: jacob.pontoppidan.thyssen@regionh.dk
Accepted May 16, 2017; Epub ahead of print May 17, 2017
Atopic dermatitis (AD) is a common chronic inflammatory skin disease. To date, few studies have examined the risk of cancer in adults with AD. However, the most consistent associations have been observed for skin cancers and lymphomas (1, 2). Potential explanatory factors for altered risk in AD include: (i) the use of immunosuppressant therapies; (ii) exposure to ultraviolet (UV) irradiation; and (iii) AD-related pathomechanistic factors, including impaired cell-mediated immunity. Furthermore, a compromised epithelial barrier function facilitating transcutaneous penetration of carcinogenic agents and viruses, including human papilloma virus (HPV), could influence the cancer risk. The aim of the present cross-sectional study was to investigate the occurrence of selected cancers among adult Danish patients with AD (both in- and outpatient) compared with general population controls.
This cross-sectional study was based on data from Danish administrative registries, which contain nationwide information on social and healthcare-related data, such as morbidity, medication use, hospitalizations, and personal income. A detailed description of the data source and methodology of this study is given in Appendix S1.
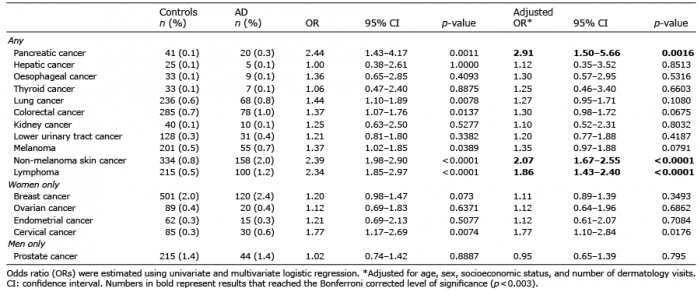
A total of 8,112 adult patients with a diagnosis of AD between 1 January 1997 and 31 December 2012, were included and matched based on age and sex with 40,560 control subjects. Baseline characteristics of the study populations are shown in Table SI. A significant association was found between AD and non-melanoma skin cancer (NMSC) compared with controls (2.0% and 0.8%; adjusted odds ratios (aOR) 2.07; 95% confidence interval (95% CI) 1.67–2.55) (Table I). Similar associations were found for cervical cancer, which occurred in 0.6% and 0.3% of patients with and without AD, respectively (aOR 1.77; 95% CI 1.10–2.84), although the p-value did not reach Bonferroni corrected level of significance which was set at < 0.003. Further adjustment for a proxy variable for smoking did not significantly change the estimates (aOR 1.76; 95% CI 1.09–2.83). The prevalence of lymphoma was 1.2% and 0.5%, respectively (aOR 1.86; 95% CI 1.43–2.40). Similarly, pancreatic cancer had a higher prevalence in patients with AD (0.3%) compared with controls (0.1%) (aOR 2.91; 95% CI 1.50–5.66). The model was further adjusted for alcohol abuse and a proxy variable for smoking, and the estimates were virtually unchanged (aOR 2.85; 95% CI 1.46–5.56). No significant associations were found between AD and malignant melanoma (MM), or between AD and hepatic, oesophageal, thyroid, lung, colorectal, kidney, lower urinary tract, breast, ovarian, endometrial, or prostate cancer.
Table I. Association between atopic dermatitis (AD) and cancers
The strongest association observed in our cohort was between AD and NMSC, which has also been shown in previous studies, although some have failed to identify this association (3, 4). Patients with AD appear to have SCCs localized to anatomical sites that are normally covered by clothes, and hence not exposed to the sun, suggesting that UV phototherapy could contribute to the risk of NMSC in these patients (4). AD-associated epidermal deficiency of filaggrin and its metabolite trans-urocanic acid may further facilitate penetration of UVB photons and, ultimately, the risk of DNA damage and skin malignancies (5). Furthermore, systemic anti-inflammatory agents have been associated with an increased risk of NMSC (6, 7). We observed no significant association between AD and MM, which is in line with most previous studies (2, 4, 8).
Adults with hospital-diagnosed AD had a higher prevalence of cervical cancer, although the estimates did not reach the Bonferroni corrected criteria for significant p-values. A recent US case-control study reported that AD was more common in HPV-positive cases compared with HPV-negative controls (9) and loss-of-function filaggrin gene (FLG) mutations have been associated with incident HPV-related cancers and pre-cancers, suggesting that HPV survival or invasion could indeed be facilitated in individuals with filaggrin deficiency (10). Furthermore, smoking has been associated with both cervical cancer and AD, and could also be a causal link between these 2 diseases (11).
The increased prevalence and risk of lymphoma in our study is in line with a systematic review and meta-analysis, which found a relative risk of lymphoma of 1.43 (95% CI 1.12–1.81) in patients with AD (1). Findings from that same study also suggested that severity of AD was a significant risk factor for lymphoma (1). While some, but not all, data suggest that AD-associated systemic and topical immunosuppressive drugs may affect the risk of lymphoma in patients with AD, this topic remains controversial (1). It is important to remember that AD and lymphoma may be subject to diagnostic overlap in selected cases, as severe AD and erythrodermic cutaneous T-cell lymphoma may have similar manifestations (12).
Finally, we found a significant association between AD and pancreatic cancer, and while other studies have reported similar results, the existing literature is scarce (2, 13). An increased prevalence of smoking and alcohol abuse in patients with AD, especially those with severe disease, may contribute to the risk of pancreatic cancer. Yet, sensitivity analyses with additional adjustment for markers of alcohol abuse and smoking did not yield significant changes compared with our primary analyses; thus, while smoking and alcohol abuse could partially explain the observed association, it is unlikely that our findings are explained solely by these lifestyle factors.
Certain limitations and strengths apply to the present study. We were only able to identify patients with a hospital (inpatient and ambulatory) diagnosis of AD; who are likely to have more severe AD disease courses than patients treated by general and private practitioners. Due to the disease severity, these patients are expected to receive immunosuppressive treatment, which could influence the risk of several malignancies. Furthermore, they often undergo more thorough examination; however, we adjusted for the number of dermatology visits to reduce surveillance bias. While we adjusted for age, sex, and number of dermatology visits in our analyses, we did not have information on lifestyle factors, such as diet, sun exposure, level of physical activity, sexual activity, occupation, and family history of cancer.
In our cohort, Danish adults with AD have a higher prevalence of NMSC, lymphoma, and pancreatic cancer compared with the general population. While these findings may, to some extent, be explained by altered immune responses, pharmacotherapy or certain lifestyle factors in adults with AD, causality remains to be established.
Funding and conflicts of interest: SF, YMFA and JPT are supported by an unrestricted grant from the Lundbeck Foundation. JPT has participated in international and national advisory board meetings for Sanofi-Genzyme and Roche and has given oral presentations about atopic dermatitis for LEO Pharma. AE has received research funding and/or salary/consultancy honoraria from Pfizer and Eli Lilly. GG is supported by an unrestricted research scholarship from the Novo Nordisk Foundation. LS has performed clinical trial for Regeneron, participated in advisory board meetings for Sanofi and is supported by a grant from the Capital Region of Denmark, Foundation for Health Research.
This research was performed independently through the authors’ academic university and hospital affiliations.


 Click to show fullsize
Click to show fullsize