


1Department of Dermatology and Allergology, Ludwig Maximilian University, Munich, Germany, and 2Division of Dermatology, Richmond Road Diagnostic and Treatment Centre, University of Calgary, 1820 Richmond Road SW, Calgary, AB, T2T 5C7, Canada. E-mail: cozhang@ucalgary.ca
Accept Jun 8, 2017; Epub ahead of print Jun 9, 2017
Pemphigus vulgaris (PV) is an autoimmune vesiculobullous disease characterized by suprabasal acantholysis. It is caused by pathogenic autoantibodies against desmoglein III, sometimes in conjunction with desmoglein I. Because desmoglein III is the major desmosomal component in mucosa, PV almost always involves mucosal surfaces. We present an unusual case of PV with an isolated lesion on the nose, and no mucosal involvement. The literature on this rare presentation is reviewed. The nose, face, and scalp are the commonest sites for localized PV, and this is likely related to both the regional pattern of antigen expression and the effects of ultraviolet radiation. We suggest local topical corticosteroids as first-line therapy based on our experience and the reports in the literature.
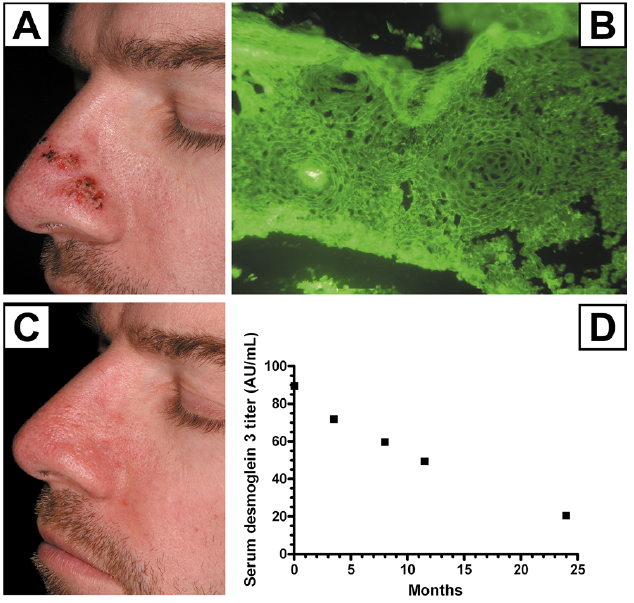
A 36-year-old previously healthy man, taking no medications, presented to us with a 9-month history of a solitary, 2 × 4 cm, erosive, crusted plaque on the nose (Fig. 1A). He had no other mucocutaneous erosions or blisters. He had not applied any topical medications to the site, and he reported no trauma. The lesion was associated with a sensation of congestion and occasional epistaxis. Previously, he had been biopsied at a different clinic with a clinical suspicion of basal cell carcinoma. The pathology showed striking suprabasal acantholysis extending down hair follicles, fitting with PV. At our initial visit, we repeated biopsies including direct immunofluorescence (DIF). Repeated DIF showed IgG and C3 in a patchy net-like intercellular pattern in the epidermis (Fig. 1B). Overall, the biopsy results were consistent with pemphigus vulgaris, but the patchy IgG pattern was unusual. Desmoglein (Dsg) 3 serum ELISA was positive (89.6 U/ml, normal < 20) but Dsg1 ELISA and indirect immunofluorescence on monkey esophagus were negative. After establishing the diagnosis of localized PV, he started mometasone furoate 1% cream BID to the lesion and had a complete response (Fig. 1C). However, he was unable to taper below 2–3 times weekly applications before a flare would appear, and pimecrolimus 1% cream was not effective.
Fig. 1. Clinical and autoimmune features of pemphigus vulgaris (PV) before and after treatment. A: Isolated erosive, crusted, erythematous plaque on the left nose. B: Direct immunofluorescence performed on a perilesional shave biopsy showed epithelial cell surface IgG and C3 staining with patchy intensity. Anti-Dsg3 antibodies did not stain. C: Healing of localized PV after application of topical mometasone furoate 1% cream BID. He maintained control with 2–3 × weekly use. D: Changes of serum Dsg3 titers over time. With topical mometasone furoate only, systemic Dsg3 antibody titers steadily declined to a borderline value, correlating with good disease control.
Over two years of ongoing follow-up, his anti-Dsg3 antibody levels trended down to a borderline value of 20.6 U/ml (Fig. 1D), and he continued to have good control with mometasone furoate cream 2–3 times weekly, with no side effects. He did not develop any other pemphigus lesions throughout this period.
Furthermore, the sections were examined for expression of Dsg-1 and -3 using anti-human Dsg-1 (Progen #Dsg1-P124) and Dsg-3 (Invitrogen #32-6300) mouse monoclonal antibodies. Dsg1 had patchy staining in the epidermis, whereas anti-Dsg3 antibody did not stain at all (the epidermis of a control section was stained in a honey-comb like pattern with both antibodies). This was an unexpected finding, as the patient only had serum autoantibodies to Dsg3.
In PV, pathogenic IgG4 and IgG1 antibodies form against Dsg3; 50% of patients also have antibodies against Dsg1. Autoantibody binding to desmogleins causes direct inhibition through steric hindrance, as well as inducing signal transduction pathways, both contributing to acantholysis. Clinically, this results in flaccid bullae and erosions, mainly occurring in two patterns: mucosal-dominant and mucocutaneous forms (1).
Our case is unusual due to the highly localized cutaneous involvement without mucosal lesions, occurring as a persistently isolated plaque throughout more than two years of ongoing follow-up. A search of the literature revealed 23 additional cases of persistently localized PV (2–10), and 5 cases of localized PV that had disseminated lesions before or after the localized presentation (usually separated by a period of months) (11, 12). Some of these cases were associated with local trauma, prior healed surgical scars, and X-irradiation, suggesting Koebnerization of PV (3–5). Additionally, one case of localized ‘contact pemphigus’ has been reported after application of ketoprofen gel (13). The female:male ratio in the cases was 1.6:1, with a mean age of 49.8 years and median age of 53 years (range: 21–88 years). This is in keeping with a middle-aged mean age of onset for PV (1). Cases were reported in various different ethnicities. There were a few cases localized to only the tongue, the lip, or the genitals, but the most common sites were the nose, scalp, and face. Although the most common site for PV lesions is the buccal mucosa due to having the highest Dsg3 expression, on the skin PV has a predilection for the head, particularly the scalp, as this is the second-highest site of Dsg3 expression (14). Ultraviolet radiation has been shown to induce acantholysis in PV, and it is possible that ultraviolet exposure plays a role in the pattern of these cases (15). As well, it has been hypothesized that the nose is easily irritated by friction.
In these localized cases, it is unclear why PV does not involve the mucosal membranes, given that the majority of cases (including ours) have antibodies against Dsg3 in serum. Relatively low antibody levels may be partially responsible for the limited nature of these presentations (2). Alternatively, these patients may express higher levels of Dsg1 or Dsg2 in the mucosa. In our case, the low pathogenicity of autoantibodies may be a clue. Usually, a mixture of autoantibodies can be found binding to the whole epidermis, but in our patient, only patchy binding to the epidermis could be seen by DIF, and indirect immunofluorescence was repeatedly negative. This suggests low binding affinity of autoantibodies to the keratinocyte surface. Furthermore, given the negative staining of Dsg3 on DIF, we speculate that our patient may have had somatic mosaicism in Dsg3 altering the structure and autoreactivity of the molecule in the keratinocytes in the nasal skin, explaining the persistent isolated site of involvement. Alternatively, the epitopes may have been shared between the patient’s autoantibodies and the monoclonal mouse antibodies used for Dsg3 detection.
Because PV currently has a mortality rate of 5–10% despite advances in management, the first-line treatment for classic PV is systemic steroids, sometimes combined with other immunosuppressants (1). Of the localized PV cases in the literature with details available regarding therapy, 8 cases were treated with local therapy through some combination of topical corticosteroids, intralesional corticosteroids, and surgery. 10 cases were treated with systemic corticosteroids with or without azathioprine. One case was treated with topical corticosteroids and oral dapsone. The responses to both systemic and local therapy were largely excellent, with only one partial response in each group. Our case also achieved a complete response with good maintenance control with a topical corticosteroid. Interestingly, the circulating Dsg3 antibody titers also decreased to a borderline value with only topical therapy. Based on these successes, along with the fact that the prognosis is benign for localized PV, we suggest that topical corticosteroids should be the first-line therapy for localized PV.


 Click to show fullsize
Click to show fullsize