


Department of Dermatology, Oregon Health and Science University, 3303 SW Bond Ave CH 16D, Portland, OR 97239, USA. E-mail: rojek@ohsu.edu
A man in his early 50s presented to our department for a skin cancer screening examination. He was generally healthy with no personal history of skin or other cancers. His family history was notable for the fact that his mother died from metastatic ocular melanoma. He had no particular concerns on his skin. Physical examination revealed a 2.5 cm soft, skin-colored nodule on the right plantar foot. (Fig. 1a) He reported this nodule had been present since childhood and was biopsied in the distant past, with the results showing a benign nevus. An excisional biopsy was performed for histopathologic evaluation (Fig. 1b). By immunohistochemical analysis, there was negative staining for nuclear expression of BRCA1 associated protein-1 (BAP1) (Fig. 1c). Genetic testing revealed a heterozygous, pathogenic, truncating, germline BAP1 variant.
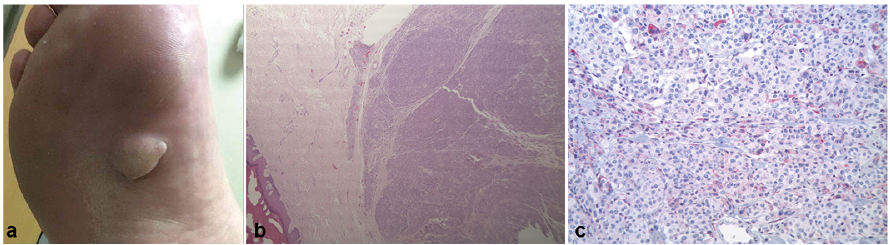
Fig. 1. (a) A large, soft, skin-colored nodule on the right plantar foot. (b) Histopathology: asymmetric, predominantly intradermal, melanocytic proliferation composed of nests and sheets of epithelioid melanocytes with large, pleomorphic nuclei and light eosinophilic cytoplasm (hematoxylin and eosin (H&E), original magnification × 2.5). (c) Negative immunohistochemical stain for BRCA1 associated protein-1 (BAP1) (original magnification ×20).
What is your diagnosis? See next page for answer.
Acta Derm Venereol
Diagnosis: Melanoma associated with germline BAP1 mutation
BAP1 is a nuclear deubiquitinating enzyme that functions as a tumor suppressor via its role in DNA damage repair (1). Identification of a cutaneous melanoma with germline BAP1 mutation confirms the diagnosis of the BAP1 cancer syndrome. This is a rare autosomal dominant genetic syndrome typified by the development of mesotheliomas and uveal melanomas. Less commonly, cutaneous melanomas, various types of carcinomas – mostly from the kidney and gallbladder – sarcomas, and brain tumors can arise as well (2). The mechanism by which these seemingly disparate malignancies arise in the setting of a germline BAP1 mutation remains poorly understood. Nevertheless, it likely depends on multiple factors including the tissue in which the second BAP1 allele is inactivated, the mechanism of inactivation of the second BAP1 allele, the functional consequences of a particular BAP1 mutation, environmental exposures, and concurrent mutations (1). Nearly all carriers of germline BAP1 mutations develop at least one malignancy by age 55, and 18% develop cutaneous melanoma (3).
Patients with BAP1 cancer syndrome develop several, distinct, melanocytic neoplasms. These are raised, pink or tan, dome-shaped, benign lesions that have been referred to in the literature as “melanocytic BAP1-mutated atypical intradermal tumors/MBAITs” or “BAPomas” (2). Histologically, these lesions have large melanocytes with superficial and deep mitotic activity, leading them to be labeled “atypical Spitz tumors” given their resemblance to Spitz nevi (2). Nevertheless, MBAITs are molecularly distinct from true atypical Spitzoid neoplasms, with comparative genomic hybridization (CGH) revealing the former have genetic aberrations at chromosome 3p21 (BAP1 locus), whereas the latter show aberrations at 6q23, 6p25, 8q24, 9p21, and/or 11q13 that influence the risk of aggressive behavior (4). Rarely MBAITs can progress to melanoma, as was the case with our patient, in which case they are staged and treated identically to conventional melanoma.
There are no formal guidelines regarding screening patients with BAP1 cancer syndrome for the associated malignancies. These patients should consider undergoing ophthalmologic exam and chest/abdomen CT every 6–12 months to evaluate for uveal melanoma, mesothelioma, and renal cancer respectively (5). We recommend that these patients receive a comprehensive dermatologic examination every 3–12 months, or according to NCCN guidelines if they have a personal history of melanoma.
In the case described here, our patient’s melanoma was at least 8.5 mm thick, so he had a brain MRI and whole-body PET/CT that showed no evidence of metastasis. He underwent wide local excision (WLE) with a sentinel lymph node biopsy (SLNB) that showed no metastasis. Baseline ophthalmologic exam was normal. Chest/abdomen/pelvis CT showed no sign of solid organ malignancy. Follow-up dermatologic exams revealed several skin-colored, dome-shaped, papules (i.e. MBAITs) that were subsequently excised. Unfortunately another cutaneous melanoma was found and he recently underwent another WLE with SLNB.


 Click to show fullsize
Click to show fullsize