


12nd Dermatology Department, Medical School, Aristotle University of Thessaloniki, Papageorgiou General Hospital, Ring Road 56403, N, Efkarpia, Thessaloniki, 2Clinical Research and Evidence-Based Medicine Unit and 3Unit of Reproductive Endocrinology, First Department of Obstetrics and Gynecology, Medical School, Aristotle University of Thessaloniki, Thessaloniki, Greece, and 4Department of Dermatology, St George Hospital, University of New South Wales, Sydney, NSW, Australia. E-mail: katerinapatsatsi@gmail.com, apatsats@auth.gr
Accepted Jun 28, 2017; Epub ahead of print Jun 29, 2017
Autoimmune bullous diseases (AIBD) place a significant burden on patients’ quality of life (QoL). Specific QoL instruments (1, 2), Autoimmune Bullous Diseases Quality of Life (ABQOL) (1) and Treatment Autoimmune Bullous Diseases Quality of Life (TABQOL) (2), were introduced to quantify the impact of AIBD and its treatment on patients’ well-being. The aim of this study was to assess QoL in Greek patients with AIBD, using the ABQOL and TABQOL questionnaires.
Patients with newly diagnosed AIBDs were recruited consecutively. Ethical approval was obtained from the local Institutional Review Board and all patients signed an informed consent form. In patients with AIBD in the pemphigus spectrum, the clinical extent and severity were measured with Pemphigus Disease Area Index (PDAI) (3) and Autoimmune Bullous Skin Disorder Intensity Score (ABSIS) (4). Thus, in patients with AIBD in the pemphigoid spectrum, the clinical extent and severity were measured with BPDAI and ABSIS. The questionnaires were handed in at 4 different time points:
The time point of established diagnosis, at which the patient had the typical clinical picture and no therapy had yet been administered, was defined as baseline (BL).
Time point 2 was the point at which the patients presented with no new lesions (NL).
Time points 3 and 4 were defined as 1 (M1) and 3 months (M3) after baseline, respectively.
Dermatology Life Quality Index (DLQI) and ABQOL were completed at all 4 time points (BL, NL, M1 and M3) before the patients were reviewed by the physician. TABQOL was handed out and completed at time points 2, 3 and 4 (NL, M1, M3), as at baseline patients had not yet been under treatment and this is a treatment-based questionnaire.
Statistical analysis of the data was performed using the software Statistical Package for Social Sciences (SPSS), version 22.0 (SPSS, Inc., Chicago, IL, USA). All tests were 2-sided and the significance level was chosen to be α = 0.05. Spearman’s = r, Friedman’s = χ2, Wilcoxon = z were used.
Fifty-three patients were invited into the study; of these, 50 agreed to be included and completed the study. Patients were studied and analysed, after they had been divided into 2 groups based on the disease type (intra-epidermal or subepidermal AIBD).
At baseline, DLQI was strongly and significantly correlated with both ABSIS (r = 0.677, p = 0.006) and PDAI (r = 0.559, p = 0.03). Thus, ABQOL was significantly correlated with PDAI (r = 0.559, p = 0.03), but not with ABSIS (r = 0.490, p = 0.064). Moreover, ABQOL was significantly correlated with the initial titres of anti-desmoglein 1 (DSG1) (r = 0.542, p = 0.037), but not with the titres of anti-DSG3 (r = 0.405, p = 0.134). ABQOL and DLQI were significantly correlated (r = 0.712, p = 0.003).
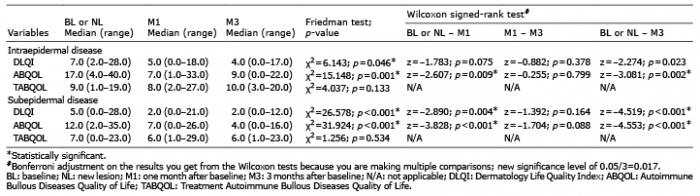
A marginal, statistically significant decrease was observed in the median DLQI scores when values at selected consecutive time points were compared (χ2 = 6.143, p = 0.046). However, ABQOL scores were significantly different between consecutively selected time points (χ2 = 15.148, p = 0.001). TABQOL, which relates to the treatment effects, showed no statistically significant differences among selected consecutive time points up to M3 (χ2 = 4.037, p = 0.133) (Table I).
Table I. Descriptive statistics for DLQI, ABQOL and TABQOL during weeks of evaluation based on the disease type
At baseline, DLQI was also significantly correlated with BPDAI (r = 0.730, p < 0.001) and ABSIS (r = 0.480, p = 0.004). Thus, ABQOL was significantly correlated with both BPDAI (r = 0.553, p = 0.001) and ABSIS (r = 0.460, p = 0.005). There was no statistically significant correlation of either ABQOL or DLQI with the initial titres of anti-BP180 and anti-BP230. ABQOL and DLQI were significantly correlated (r = 0.816, p < 0.001).
A statistically significant decrease was observed at the median DLQI scores when values at consecutive time points were compared (χ2 = 26.578, p < 0.001). Thus, ABQOL scores were also significantly decreased (χ2 = 31.924, p < 0.001). Regarding TABQOL, no statistically significant differences between selected consecutive time points up to M3 were observed (χ2 = 1.256, p = 0.534) (Table I).
AIBD may severely affect QoL. A German study used the dermatology-specific questionnaire DLQI for the first time in pemphigus patients. The mean DLQI for pemphigus was higher than the mean scores for other AIBD, such as bullous pemphigoid (5). Last year, in a Brazilian study, the medians of total DLQI scores of patients with pemphigus and pemphigoid diseases did not differ significantly from each other (6). In our study, we observed a significant impairment in QoL at baseline and a rather heavier impact in the group with intraepidermal AIBD.
The first study that was designed to develop a disease specific for AIBD QoL instrument was conducted in Australia. In this development and validation study, there was a low correlation between ABQOL and disease activity measures and a moderate correlation between ABQOL and DLQI (1). In our study, ABQOL and DLQI were significantly correlated with disease activity as it was captured by ABSIS, PDAI or BPDAI in all patients.
According to Boulard et al. (7), cut-off values of 15 and 45 for PDAI and 17 and 53 for ABSIS, distinguish moderate, significant and extensive pemphigus forms. The mean PDAI in our patients was 35.80 ± 32.35 and mean ABSIS was 19.40 ± 10.92. Consequently, we assessed QoL in patients with significant to extensive pemphigus. Notably, a statistical significant correlation between QoL scores was observed only with the titres of anti-DSG-1 autoantibodies and not with anti DSG-3, anti BP180 or anti BP230 autoantibodies. This finding is in accordance with a previous study in a cohort of 35 Greek patients with pemphigus (8).
Reliability of the ABQOL was evaluated in a Northern American patient cohort (9). An important distinction from the Australian patient group was that, in this cohort, a greater proportion of patients had active disease. In our group of Greek patients the mean ABQOL scores were higher compared with the Australian and North American patients.
Treatment of AIBD may have a significant risk of medical complications and a severe impact on QoL, which is difficult to differentiate from the burden of the disease itself. TABQOL was developed and validated to allow a quantitative measurement of treatment-based QoL impact in AIBDs (2). TABQOL had a high correlation with ABQOL and a moderate correlation with DLQI. In the above-mentioned study, the majority of patients were in remission and during routine follow-up (2).
We should emphasize that ABQOL, in pemphigus patients, showed a significant correlation with clinical severity and a significant decrease from the first month of treatment. This was not captured by DLQI scores. With this study, we assessed for the first time the QoL in Greek patients with various AIBD using disease-specific QoL measurement tools. There were no difficulties for the patients to comprehend and answer the questions and even more, no patient refused to complete the tool at the consecutive time points needed. Applying pemphigus-specific measures, may allow clinicians to recognize which aspects of AIBD most affect a patient and provide a personalized care. Moreover, ABQOL and TABQOL may be used as an additional end-point in clinical trials, in order to better monitor and report the impact of side-effects of therapeutic interventions.


 Click to show fullsize
Click to show fullsize