


1Nephrology Unit, Department of Internal Medicine I, Departments of 2Laboratory Medicine, 3Pathology and 4Dermatology, Paracelsus Medical University, Salzburg, and 5Department of Dermatology, Medical University Graz, Graz, Austria
Subcutaneous calcifications can lead to complications, including pain, inflammation, ulceration and immobilization. Studies on the pathophysiology of mineral compositions and effective treatment modalities are limited. We therefore studied 14 patients with subcutaneous calcifications. Mineral material was collected and analysed by Fourier transform infrared spectrometry. Blood analyses were run to evaluate systemic alterations of mineral metabolism. Carbonate apatite (CAP) was found to be the single constituent in the majority of patients (n = 9, 64.3%), 3 cases (21.4%) had a composition of CAP and calcium oxalate dihydrate and one case had a combination of CAP and magnesium ammonium phosphate, whereas CAP was the major component in all 4 cases. Only one case showed predominantly calcium oxalate. Thus, CAP was found to be the only or predominant component in most cases of subcutaneous calcifications. Chemical analyses of the mineral compositions may aid in the development of new treatment regimes to improve the solubility of mineral components and to decrease extraosseous calcifications.
Key words: subcutaneous calcifications; tumoural calcinosis; carbonate apatite.
Accepted Jun 28, 2017; Epub ahead of print Jun 29, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Hermann Salmhofer, Nephrology Unit, Department of Internal Medicine I, Paracelsus Medical University, Müllner Hauptstrasse 48, AT-5020 Salzburg, Austria. E-mail: h.salmhofer@salk.at
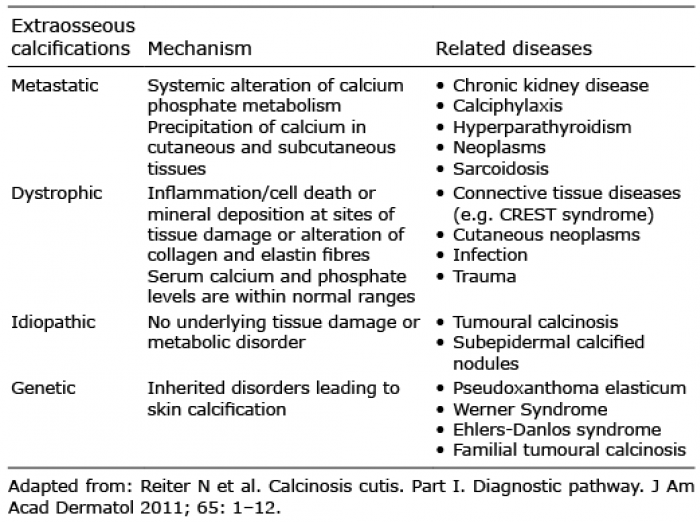
Various disorders may lead to calcium-containing extraosseous mineral depositions or even ossification. Calcifications may occur in subcutaneous or periarticular localizations and in circumscript or generalized distributions. Extraosseous calcifications can be further stratified into metastatic, dystrophic, idiopathic and genetic forms (1, 2) (Table I). Metastatic calcifications are the effect of a systemic alteration of calcium phosphate metabolism, such as in chronic kidney disease, calciphylaxis, hyperparathyroidism, neoplasms and sarcoidosis (2).
Table I. Mechanisms of extraosseous calcification and related diseases
Dystrophic calcification arises from inflammation or cell death and nucleation of mineral deposition at sites of tissue damage or alterations of collagen and elastin fibres. This may occur in various diseases, including connective tissue disease, cutaneous neoplasms, infections and trauma. The nature of idiopathic calcifications is unclear, since no systemic or local trigger has yet been identified (3, 4). Additional knowledge of promoters and inhibitors of extraosseous calcification has arisen from mouse models without human counterpart (3).
Clinically, end-stage renal disease and connective tissue disease predominate among calcifying disorders. However, the pathogenesis of some forms of cutaneous or subcutaneous calcinoses remains unclear.
In biological systems, a variety of calcium phosphate compounds may be found: carbonate apatite (CAP), amorphous calcium phosphate, calcium pyrophosphate, Whitlockite, di-calcium phosphate dihydrate and octa-calcium phosphate (5). Changes in pH or solution composition may induce transformation of calcium phosphate phases; formation and transformation may further be influenced by organic or inorganic moieties (5).
To date, only a few reports on the pathogenesis and mineral composition of various extraosseous calcifications have been published, including the discovery of CAP depositions in calcific periarthritis, uraemic tumoural calcinosis, idiopathic inflammatory myopathies, calcified mitral valves, calcified calculi of hydrocele, in atherosclerosis, as well as in the cervical spine of a patient with CREST (calcinosis, Raynaud’s phenomenon, oesophageal dysmotility, sclerodactyly, and telangiectasia) syndrome (5–14).
In order to determine the composition of calcium precipitations in a variety of calcifying skin diseases, we collected extruded material of cutaneous and subcutaneous calcifications.
We conducted a retrospective study of 14 patients with calcium-containing mineral depositions of skin and subcutaneous tissues. The study protocol was waived by the Institutional Review Board and was conducted according to the Federal Laws and Regulations of Austria and is adherent with the Declaration of Helsinki 1975, as revised in 2000. All individual patients gave their written informed consent to collection, analysis and scientific work-up of the extruded inorganic material.
Spontaneously extruded cutaneous calcifications of 14 patients were collected and instantly transferred for further laboratory analysis.
Fourier transform infrared spectrometry (FTIR): Inorganic samples were prepared for FTIR according to the manufacturer’s instructions. Briefly, inorganic material was pulverized in a pestle and mortar and subsequently homogenized with potassium bromide. This mixture was pressed into discs approximately 0.2 mm thick. Spectra were recorded using the Bruker Tensor 27 system (Bruker Optik GmbH, Germany). OPUS software was used for data analysis.
Laboratory analysis, including calcium, phosphate, parathyroid hormone, alkaline phosphatase, C-reactive protein and creatinine blood levels was performed.
A total of 14 patients were evaluated. Their demographic data, composition of mineral depositions and primary diseases are summarized in Table II and Fig. 1. The majority of patients were women (n = 11, 78.6%) and the median age at diagnosis was 63.5 years (range; 46–88 years). Six patients (42.9%) had CREST syndrome, 4 cases (28.6%) had calcinosis cutis, one had generalized calcifying morphaea, one dermatomyositis, one septal panniculitis and one tumoural calcinosis.
Table II. Patient characteristics, primary diseases and mineral compositions
Fig. 1. Radiographic images of 3 patients with calcifying skin disorders. X-ray of right hand (A) and CT scan of buttocks (B) in severe CREST syndrome; abdominal CT scan in generalized morphaea (C); CT scan of buttocks in septal panniculitis (D).
Apart from one patient with severe renal hyperpara-thyroidism associated with haemodialysis treatment (patient 14) and one patient with isolated hyperphosphataemia under haemodialysis treatment (patient 5), they did not reveal any systemic pathologies of mineral metabolism.
In all 14 cases (100%) of various skin diseases, carbonate apatite was found. In 9 cases (64.3%), pure carbonate apatite was found. Four cases (28.6%) had minor admixture of other minerals: calcium oxalate dihydrate in 3 patients (21.4%) and magnesium ammonium phosphate in one patient (0.7%). In only one (patient 3) the extruded material was composed of 90% calcium oxalate dihydrate and 10% CAP.
Extraosseous calcifications may manifest in various clinical forms. They can present as minor depositions in the skin and subcutaneous tissues of manifold distributions. Sometimes, these depositions are spontaneously extruded and may result in poorly healing skin defects.
On the other hand, vast, tumour-like and possibly debilitating calcifications may develop.
Determination of the exact mineral composition of extraosseous calcium precipitations may help to better understand the pathological mechanism of mineral deposition. This may contribute to the development of treatment regimens delaying the progression of potentially debilitating (painful, immobilizing, deforming or ulcerating) diseases.
Various treatment recommendations for calcifying skin diseases have been reported (15), including aluminium hydroxide (16), bisphosphonates (17), magnesium supplementation (18), minocycline (19), diltiazem (20), intra-lesional injection of corticosteroids (21) surgery (22, 23) and lithotripsy (24).
A further promising treatment modality for cutaneous calcification includes the use of sodium thiosulphate. It has been assumed, that sodium thiosulphate may improve dissolution of calcium phosphate precipitates by forming highly soluble calcium thiosulphate complexes; it has been successfully applied in vascular calcifications of calciphylaxis (25).
The mechanisms of calcification of the skin still remain unclear; however, there are parallels to the pathomechanism of urolithiasis. Taking these into consideration might aid the future development of new therapeutic targets. Possible methods could include: (i) influencing calcium exposure, e.g. via dietary restriction and correct choice of calciuretic diuretics; (ii) to influence the precipitation partners of calcium, e.g. phosphorus and oxalate exposure; (iii) to influence bone metabolism (parathyroid hormone, vitamin D) and; (iv) to influence the extracellular environment/ambience; this might affect the type of mineral formation as well as the solubility of the extraosseous calcium precipitates (via urine dilution, pH modification or systemic or local solubility mediators, such as fetuin, matrix GLA protein, vitamin K (26), magnesium, pyrophosphate, and sodium thiosulphate.
Interestingly, in a variety of diseases leading to skin calcifications, CAP was the only or predominant mineral found. In our series, there was only one patient (patient 3) with a different type of mineral deposition, containing 90% calcium oxalate dihydrate and only minor amounts (10%) of CAP. This patient had gluteal necrotizing septal panniculitis and arteriolar hyalinosis, clinically presenting as tumoural calcinosis of the lumbar regions and buttocks. Two years later, according to minor criteria, systemic lupus was diagnosed.
This finding is significant, since CAP, the mineral regularly found in bone, would not be expected to occur spontaneously in extraosseous, soft tissues. Calcification is mostly believed to be a regulated process involving matrix proteins. Depending on matrix proteins, such as collagen type I and dentin matrix protein-1, a controlled synthesis of CAP (and its inhibition by osteopontin) has been reported by Gajjeraman et al. (27). Transmineralization processes of various calcium phosphate components (CAP, amorphous calcium phosphate, octa-calcium phosphate, di-calcium phosphate di-hydrate, Whitlockite) may arise under pathological conditions, at least in vascular calcification (5).
De Yoreo & Dove (28) could demonstrate shaping of in vitro crystal formation by other molecules.
Body fluids are near super-saturation with calcium and phosphate. In a supersaturated inorganic blood serum model, carbonate apatite could be precipitated in vitro, as shown by Sandin et al. (29). Yet, inhibitors of calcification prevent generalized calcification (30).
Inducers (such as sodium-dependent phosphate co-transporters) and inhibitors of calcium phosphate precipitation (such as fetuin, matrix GLA protein and osteopontin) may play a role in the formation of extra-osseous calcifications (31).
Many inducers and inhibitors of extraosseous calcification have been identified in vascular calcification (32). It is tempting to speculate, that similar mechanisms may influence dystrophic calcification. Eidelman et al. (11) hypothesized, that a loss of local inhibitors caused mineral deposition in inflammatory myopathies.
Enzyme activities, such as tissue non-specific alkaline phosphatase (33) or ectonucleic pyrophosphatase/phosphodiesterase-1and their polymorphisms (34) need to be further evaluated in extraosseous calcification.
Thus, many diverse mechanisms may influence the risk of extraosseous mineral deposition.
Recently a nano-particle-based assay to measure the overall propensity for calcification in serum has been established and is to be evaluated in patients with renal failure (35). It is thus hoped that further knowledge will also be gained about other calcifying diseases.
The prevailing mineral in most cases of subcutaneous calcification is CAP; despite the different origins of diseases, a common pathway of mineral deposition is shared.
The results of the current study are limited by the small number of patients: thus, in the future larger prospective analyses of calcium depositions in extraosseous tissues will be needed to validate these findings. It is hoped that this will ultimately lead to new concepts of pathophysiology and treatment.
Future research directions might be targeted to influencing tissue and/or urine pH (to increase solubility of the respective calcium compound); influencing calcium homeostasis by loop diuretics to modify calcium homeostasis; influencing the exposure to precipitation partners of calcium (e.g. phosphate or oxalate); activating matrix GLA protein via vitamin K2 supplementation; influencing calcium phosphate solubility via sodium thiosulphate (a putative chelator of divalent cations, which has proved effective in tumoural calcinosis and calciphylaxis; yet the exact mechanism of sodium thiosulphate has not been clarified) and by magnesium supplementation. And, possibly, by influencing enzymes that may play a role in extraosseous mineralization (e.g. by changing the level of pyrophosphate).
The authors thank Mr Simon Auer for his excellent expert technical assistance.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize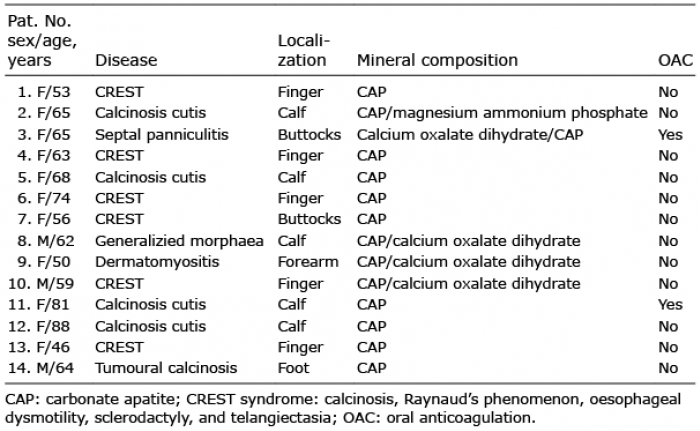 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize