


1Department of Dermatology, Fukuoka University School of Medicine, 7-45-1 Nanakuma, Jonan-ku, Fukuoka 814-0180, and 2Department of Medicine of Sensory and Motor Organs, Division of Dermatology, Faculty of Medicine, Tottori University, Tottori, Japan. E-mail: mob3mob3@yahoo.co.jp
Accepted Sep 13, 2017, Epub ahead of print Sep 13, 2017
Although 95% of patients with neurofibromatosis 1 (NF1) can be diagnosed by the age of 8 years using National Institutes of Health criteria (1), diagnosis in infants without a family history is sometimes difficult. Mutation analysis has recently been reported to be useful for early diagnosis, but it is often difficult to perform genetic diagnostics in daily medical practice (2). The presence of multiple café au lait macules (CALMs) on the entire body including the back is the most common symptom of NF1 in infants. Mongolian spots (congenital dermal melanocytosis) are frequently seen on the back and buttocks of Asian infants and generally disappear by adolescence (3–5); therefore, CALMs often accompany Mongolian spots in Asian infants with NF1. When CALMs are present within a Mongolian spot on the back of such infants, the CALMs are typically surrounded by a more lightly pigmented halo (6). The characteristics of this peculiar phenomenon have not been investigated in detail (7–10). We conducted a case series study of infants with NF1 to reveal the clinical characteristics of halo phenomenon.
This study included 24 patients from among 95 children (age range 0–10 years) with NF1 who visited the Department of Dermatology at Fukuoka University Hospital or Tottori University Hospital between 2005 and 2016. All patients had 6 or more CALMs and fulfilled the NF1 diagnostic criteria proposed by the National Institutes of Health (11). Some children did not fulfil the diagnostic criteria of NF1 at the time of first presentation, but we confirmed that all patients eventually fulfilled the criteria. The patients all had at least one CALM overlapping with a Mongolian spot on the back or buttocks and their records included a photograph of the lesion. Genetic screening tests were performed in 5 patients. Clinical information, including sex, age, family history of NF1, was retrieved from medical records. The number of CALMs within a Mongolian spot was counted manually on clinical pictures. We also investigated the colour tone of CALMs with and without the halo phenomenon using digital clinical photographs and computer software. The luminance of each CALM was quantified with Adobe Photoshop software (Adobe Systems, San Jose, CA, USA). For individuals with multiple CALM lesions, the luminance was averaged. A higher luminance index indicated a brighter lesion, suggesting a lighter coloured macule. The luminance of CALMs with and without haloed phenomenon was compared using Student’s t-test; p < 0.05 was considered statistically significant. The study was approved by the ethics committees of the institutional review boards of Fukuoka University Hospital and Tottori University Hospital.
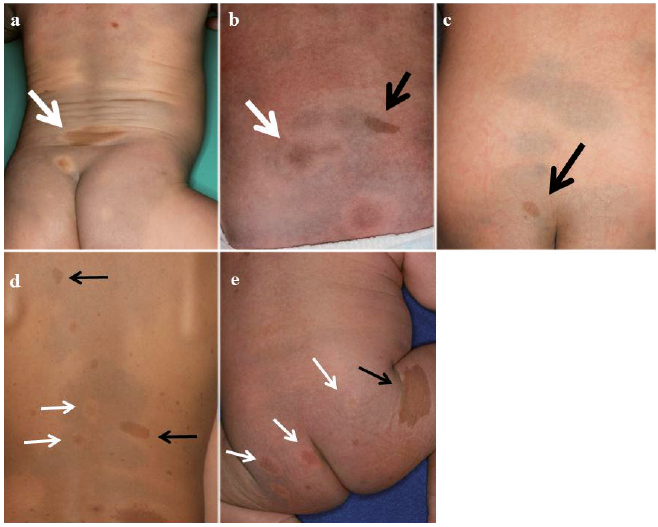
Summarized data from all patients with NF1 who had macules overlapping a Mongolian spot are shown in Table SI. Twenty-four patients with NF1 were enrolled in this study (9 boys, 15 girls; median age 7 months; range 0–91 months). Seven out of 21 patients (33.3%) had a family history of NF1 confirmed from medical records. Four out of 5 patients who underwent genetic testing had an NF1 gene mutation; in the fifth case, no obvious mutations were found in NF1. Twenty-one out of 24 patients (87.5%) had CALMS that showed the halo phenomenon. Among them, 10 patients (41.6%) showed the halo phenomenon around all CALMs within the Mongolian spot (Fig. 1a: representative case, F4). The remaining 11 patients (45.8%) had CALMs both with and without the halo phenomenon (Fig. 1b: representative case, F5). Three patients had only one CALM overlapping a Mongolian spot and did not show the halo phenomenon (Fig. 1c: representative case, F13). Among a total of 102 CALMs overlapping Mongolian spots in 24 patients, 69 (67.6%) showed the halo phenomenon and 33 (32.3%) did not.
Fig. 1. Clinical characteristics. (a) A case of the halo phenomenon within a Mongolian spot. All café au lait macules (CALMs) have this peculiar phenomenon. (b) A case of CALMs both with (white arrow) and without (black arrow) the halo phenomenon. (c) A case without (black arrow) the halo phenomenon. (b, d, e) In addition to having a light marginal zone, most CALMs with haloes (white arrow) are significantly paler than non-haloed CALMs (black arrow).
We focused on the 11 cases that had CALM lesions both with and without the halo phenomenon (Table SII). Macroscopically, we found that in most CALMs with the halo phenomenon, not only the circumference of the CALM, but also the CALM itself, was lighter in colour than CALMs without haloes (Fig. 1b, d, e). Also, CALMs with haloes had an indistinct edge compared with CALMs without the phenomenon. When digitally quantitated, the mean luminance index of CALMs with the halo phenomenon was higher than that of CALMs without the halo phenomenon. However, this difference did not reach statistical significance (p = 0.44).
To our knowledge, this is the first case series study focusing on this issue. First, we found that the halo phenomenon was present in 21 of 24 patients with NF1 (87.5%). Approximately half of the patients had CALMs both with and without haloes. We also found that this phenomenon does not occur around all CALMs within a Mongolian spot. Among all CALMs that overlapped with a Mongolian spot, 32.3% (33/102) did not show the halo phenomenon. In addition, 3 of the 24 patients (12.5%) had a single CALM overlapping a Mongolian spot and these did not show the halo phenomenon. This finding suggests that the number of CALMs within a Mongolian spot might be related to the development of the halo phenomenon.
Regarding the pathogenesis of CALM, second-hit mutations of NF1 in melanocytes have been revealed in CALM (12). A recent study found that inactivation of the NF1 gene resulted in increased melanin synthesis via cAMP-mediated PKA and ERK pathways (13). Hepatocyte growth factor and stem cell factor secreted by dermal fibroblasts in NF1 are also related to the development of CALM (14). The halo phenomenon is well known in Sutton’s naevus. Sasagawa et al. (8) demonstrated that haloes around CALMs were histopathologically different from that of Sutton’s naevi, with fewer inflammatory cells in CALMs than in Sutton’s naevi. Hamada & Suzuki (9) found decreased DOPA reaction of dermal melanocytes and slightly fewer dermal melanocytes in the halo zone. Although the exact mechanism of the halo phenomenon in NF1 remains unclear, we found that subjects with a single CALM within a Mongolian spot did not show the halo phenomenon. This finding may indicate that the halo phenomenon happens only stochastically, and that the presence of multiple CALMs may increase its probability. In addition, it may also affect the colour tone of the CALM itself, causing a clinically lighter tone in CALMs with the phenomenon.
We found an interesting case (case T5) of a patient with no mutation confirmed in the NF1 or Spred1 gene on full sequencing of those genes by next-generation sequencing, who still had CALM with the halo phenomenon. It is possible that this phenomenon is seen in other RASopathies. Further research is needed to elucidate the details of this condition.
This study has some limitations. The number of enrolled patients was relatively small. Also, as Mongolian spots are seen only in Asian infants, the significance of this phenomenon may not be relevant to other populations.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize