


Department of Dermatology, Friedrich-Alexander-University Erlangen-Nürnberg (FAU), Universitätsklinikum Erlangen, Ulmenweg 18, DE-91054 Erlangen, Germany. E mail: ugur.uslu@uk-erlangen.de
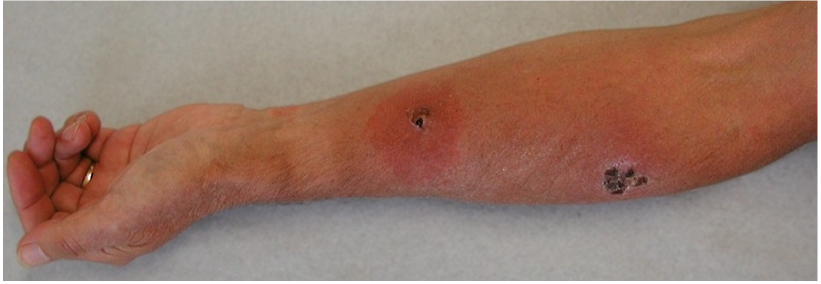
A 64-year-old German man, employed as a university biologist, with a past medical history of arterial hypertension and non-Hodgkin’s lymphoma presented with 2 swollen and erythematous boil-like lesions on his left lower arm. He had first noticed the lesions following insect bites while in Ecuador 4 weeks previously. Bacterial infection was suggested and oral ciprofloxacin treatment was started at a local Ecuadorian hospital. However, the skin lesions further increased in size and intermittent serosanguinous effusion was noted, leading to the current presentation after his return to Germany. In addition, intermittent pulsation and “movements” inside the skin lesions were reported. Fever and malaise were absent. Physical examination revealed 2 crusted nodules on the lower left arm (Fig. 1). Blood tests did not show pathological results. Ultrasound examination revealed subcutaneous oval lesions with thin echo-poor halo, and demarcated echo-rich structures with dorsal attenuation surrounded by oedematous connective tissue.
What is your diagnosis? See next page for answer.
Fig. 1. Clinical findings at the time-point of first presentation. Notable are 2 crusted nodules on the patient’s lower left arm, 1 cm in diameter with a central pore and pronounced surrounding erythema and swelling.
Given the patient’s history and clinical findings, furuncular myiasis was diagnosed, which is a parasitic infestation of living tissue, mainly caused by the larvae of the human botfly Dermatobia hominis (1). This causative botfly is frequently seen in Central and South America, where it is indigenous (1, 2). In Europe and the USA, however, only imported cases among travellers have been described (3, 4).
D. hominis is a perennially active, approximately 15-mm long, yellow-headed fly with a grey-blue thorax and metallic blue abdomen (5). It is seen mainly in high humidity and high temperature regions of Central and South America (1, 5). The larvae of this botfly are obligate parasites that develop in living tissue and cause furuncular myiasis in humans (5). In the Western world, especially, travellers returning from Central or Southern American countries may present with furuncular myiasis (1–5). It is typically diagnosed after careful history-taking and a characteristic clinical presentation: a crusted nodule with a central pore that intermittently exudes a serosanguinous discharge (1–5). The furuncle may be accompanied by nocturnal pain (1–5). A method to diagnose the infestation is to submerge the lesion in water to evaluate whether air bubbles appear (6). In addition, dermatoscopy or sonography may confirm the clinical diagnosis and rule out differential diagnoses, such as arthropod bite reaction, pyoderma, an inflamed epidermoid cyst, cutaneous larva migrans, or cutaneous leishmaniasis (6–8). Magnetic resonance imaging may not reveal any characteristic features to support the clinical diagnosis, but can be performed in order to make an exact localization and to rule out involvement of critical structures (4). Myiasis is generally self-limiting (1–5). However, severe complications can occur, including tetanus and bacterial superinfections (1, 2, 5). Surgical removal is the treatment of choice (1, 2, 5). Alternative methods based on asphyxiation by occlusion of the respiration pore to induce the larvae to move upwards in the skin have been described, e.g. by application of mineral oils, paraffin, petroleum jelly, glue, or beeswax, followed by minimal surgical incision (1, 2, 5). Complete extraction of the larva is essential to prevent severe inflammatory reaction (1, 2, 5).
In our patient, surgical removal of the larvae was recommended. Despite repeated detailed explanation of the medical risks, the patient refused surgical removal due to his professional interest as a university biologist. Thus, local antiseptic therapy and systemic treatment with levofloxacin under close clinical follow-up was initiated in order to avoid secondary infection. Follow-up examinations did not reveal any pathological laboratory parameters or clinical symptoms. While one of the larvae spontaneously deceased and was removed by the patient himself, the second larvae ejected itself approximately 10 weeks after infection (Fig. 2). The skin lesions healed, leaving 2 scars on the left lower arm.
Fig. 2. (a, b) Clinical findings of the skin lesions at the time the larva ejected itself, approximately 10 weeks after infection.


 Click to show fullsize
Click to show fullsize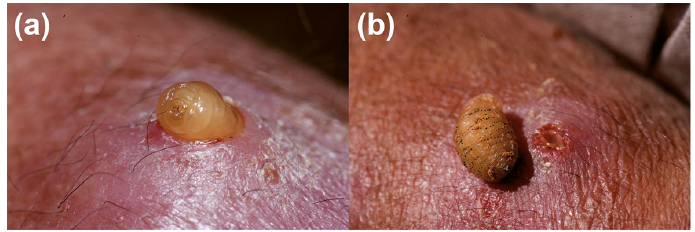 Click to show fullsize
Click to show fullsize