


1Department of Dermatology, University Medical Center Mannheim, 2Mannheim Institute of Public Health, Social and Preventive Medicine, Medical Faculty Mannheim, Heidelberg University, Mannheim, 3Institute for Health Services Research in Dermatology and Nursing (IVDP), University Medical Center Hamburg-Eppendorf, Hamburg, 4Dermatological Practice Wroblewska, Spaichingen, 5Department of Dermatology, Psoriasis-Center, University Medical Center Schleswig-Holstein, Kiel, 6Department of Dermatology, University Hospital of Erlangen, Erlangen, and 7Department of Dermatology and Phlebology, Vivantes Klinikum im Friedrichshain, Berlin, Germany
Systemic antipsoriatic treatment options are increasing rapidly. The aim of this nationwide discrete choice experiment was to compare patients’ (n = 222) and physicians’ (n = 78) preferences for outcome and process attributes of systemic antipsoriatics using Relative Importance Scores (RIS). Both groups considered Psoriasis Area and Severity Index 90 (PASI 90) to be most important (RIS 21.4 and 20.8, respectively). Moreover, patients were highly concerned about mild and severe adverse events (RIS = 18.2 and 14.2), physicians about severe adverse events (RIS = 14.9) and cost (RIS = 13.8). Compared to physicians, patients worried more about mild adverse events and treatment location, but less about cost and frequency of laboratory tests. Physicians’ preferences were influenced by work experience and percentage of biological prescriptions, patients’ preferences by age, disease duration and severity. Older and less severely affected patients recruited via a patient organization focused more on safety, but less on efficacy and time until response than did patients from study centres. In conclusion, these differences in trade-offs should be integrated into a shared decision-making.
Key words: biologicals; conjoint analysis; discrete choice experiment; preferences; psoriasis; systemic treatment.
Accepted Nov 2, 2017; Epub ahead of print Nov 7, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Wiebke K. Ludwig-Peitsch, Department of Dermatology and Phlebology, Vivantes Klinikum im Friedrichshain, Landsberger Allee 49, DE-10249 Berlin, Germany. E-mail: wiebke.ludwig-peitsch@vivantes.de
Psoriasis has a prevalence of 2–3% in Northern countries. Approximately 20% of patients have moderate-to-severe psoriasis and require systemic treatment. Traditional medications approved for this indication in Germany are acitretin, cyclosporine, fumaric acid esters and methotrexate (1). Biologicals and apremilast have substantially expanded the treatment repertoire in the last decade. Biologicals are associated with a more favourable risk-benefit profile, but also with higher medication costs than are traditional drugs (2–9). Therefore, biologicals are mostly prescribed second- or third-line in Germany, although interleukin 17 antagonists and the tumour necrosis factor (TNF) inhibitor adalimumab have first-line approval. Several novel systemic drugs are expected to become available soon (10–12).
Systemic antipsoriatics differ considerably from each other in terms of efficacy, safety, adverse events (AE), administration process, costs and monitoring requirements. Due to the rapidly increasing number of options, several medications may be suitable for an individual patient. The choice of a specific drug depends on the physician’s assessment, experience and prescription preferences. However, the medication should also match the patient’s preferences, which must be included to provide patient-centred care (13, 14). Physicians can counsel patients more appropriately if they understand their perspective. They should be aware that their own perception and the patients’ view may differ (14, 15) and that mismatch between treatment attributes and patients’ preferences can result in a vicious circle of low satisfaction, non-adherence and suboptimal outcome, problems commonly encountered among patients with psoriasis (16).
We recently performed discrete choice experiments (DCE) to evaluate patient preferences for biologicals and showed high preferences for safety and efficacy (17). However, our previous study had a monocentric design, did not address preferences for other systemic treatments and did not consider physicians’ preferences. The aim of the nationwide DCE presented here, the PsoCompare study, was to compare physicians’ and patients’ preferences for attributes of all systemic medications that were either approved or in advanced development for moderate-to-severe psoriasis.
The study was conducted in Germany from 1 September 2015 to 31 August 2016. Patients were recruited in 2 ways. First, through a call for participation published in the member magazine of the largest German patient organization for psoriasis (Deutscher Psoriasis Bund e.V.). Secondly, 5 study centres (4 Dermatology Departments of University Hospitals and 1 dermatological practice) enrolled patients during regular visits. All individuals aged ≥ 18 years who had physician-confirmed plaque-type psoriasis and who were able to provide informed consent were eligible for inclusion.
Dermatologists and residents in dermatology experienced with psoriasis treatments were eligible for inclusion in the physician cohort. Physicians participating in the German Psoriasis Network “PsoNet” and/or working in psoriasis centres were invited via email to complete the survey. All participants received detailed information on the study, and, after providing informed consent, were given an access code and a link to the survey. The study was performed according to the principles of the Declaration of Helsinki and approved by the Ethics Committee of the Medical Faculty Mannheim (ethics approval 2009-329E-MA, 22 October 2009; amendment 30 July 2015).
A web-based questionnaire containing a DCE was used to elicit preferences. For generation of the discrete choice scenarios, all systemic antipsoriatics approved for moderate-to-severe psoriasis in Germany or in advanced clinical development (ongoing or completed phase III trials) were decomposed into outcome (probability of Psoriasis Area and Severity Index (PASI) 75 and 90 response, time until response, probability of mild and severe AE) and process attributes (treatment location, frequency, delivery method, frequency of laboratory tests and cost to the healthcare system). Four realistic levels for each attribute were chosen based on the Summary of Product Characteristics, literature research and consultation with experts (Table SI). Attributes were assigned to 2 groups to prevent information overload. Probability of PASI 75 and PASI 90 response were allocated to separate groups, as were probability of mild and severe AE. Cost was part of both groups to allow comparison of Relative Importance Scores (RIS) across all attributes. Attributes and levels were the same for patients and physicians, but in the patient survey medical terms were explained in laymen’s language.
Hypothetical treatment scenarios were designed with the CBC/HB feature of commercially available conjoint analysis software (www.sawtoothsoftware.com) by combining these levels in a random fashion. CBC/HB is a tool for estimating individual-level results for Choice-Based Conjoint (CBC) experiments. Examples of scenarios are shown in Table SII. Twelve choice sets, each comprising 2 alternative scenarios, were selected per group and participant by random-orthogonal method. Patients were repetitively asked to choose their preferred scenario. Physicians were requested to choose the alternative they would prefer for treatment of a virtual average patient with moderate-to-severe psoriasis. Two fixed experiments, with one option being superior in each attribute, were presented for control. Part-worth utilities for each attribute level were computed with logit regression. Utilities were estimated by calculating the range between the highest and the lowest part-worth utility for each attribute. A RIS for each attribute was calculated by dividing the attribute’s range by the sum of all attribute ranges and multiplying by 100 (18). RIS were determined individually for each participant and later averaged across the sample.
The patient survey additionally contained questions on demographics, income, education, medical history, disease severity and comorbidities and the Dermatology Life Quality Index (DLQI). The physician survey comprised questions on demographics, occupational status and characteristics of psoriasis patients usually treated. The surveys were pilot-tested in n=10 patients and n=3 physicians to verify understandability.
Associations of participants’ characteristics with RIS were analysed with SPSS Version 22. Analyses were performed with respect to age, sex, net monthly household income (< €2,000 vs. €2,000–4,000 vs. < €4,000), education (secondary school certificate vs. general qualification for university entrance), recruitment method (via patient organization vs. via study centres), disease duration, psoriatic arthritis (PsA; yes or suspected vs. no), body surface area (BSA) affected by psoriasis (estimated by using the patients’ palms, excluding the fingertips, to measure the extent of their psoriasis) and DLQI for the patient cohort and with respect to sex, work experience in dermatology, qualification in dermatology (specialist or resident), workplace (hospital or practice), number of patients with psoriasis treated per year, number of patients with PsA per year, percentage of patients with moderate-to-severe psoriasis and percentage receiving biologicals for the physician cohort. If necessary, variables were transformed (e.g. log10) to approach normal distribution. Associations of characteristics with RIS were tested with analysis of variance (ANOVA) for categorical variables and with Pearson’s correlations (PC) for continuous factors. Differences in RIS between the patient and physician cohort were explored using ANOVA.
For multivariable linear regression analysis, each attribute’s RIS was defined as dependent variable. Models for the patient cohort included age, sex, disease duration, PsA and BSA as independent variables; models for the physician cohort comprised sex, work experience in dermatology, workplace, number of patients with PsA per year and percentage of patients with biologicals. Other variables were neglected due to possible multicollinearity. Standardized regression coefficients (β) were assigned to each independent variable, indicating the amount of change in RIS when varying the respective variable.
Significance was assumed at p ≤ 0.05.
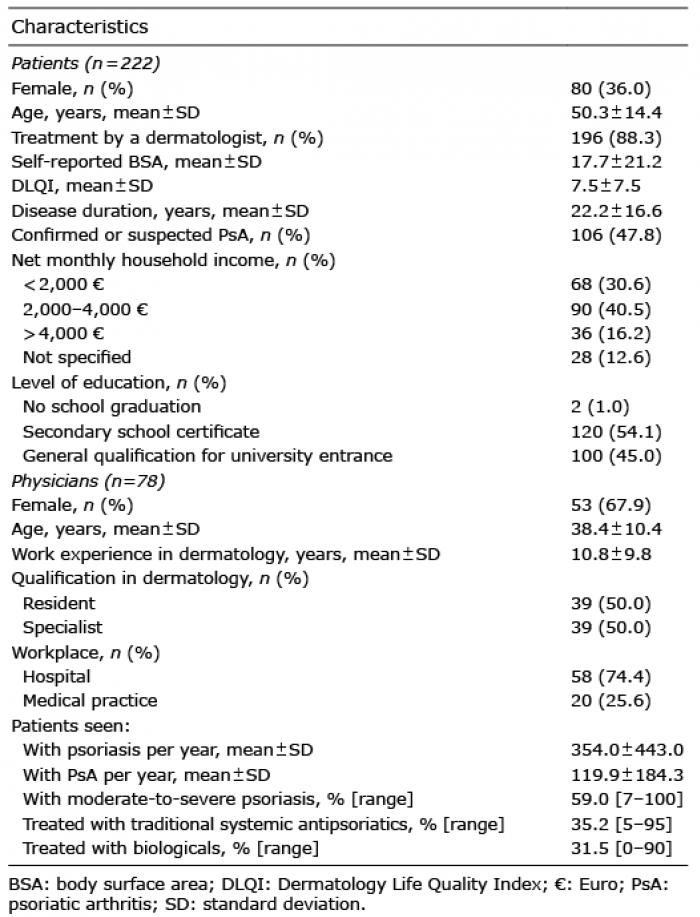
A total of 222 individuals with psoriasis were recruited, 56 (25.2%) via the patient organization and 166 (74.8%) via the study centres. The majority of subjects were male (64.0%), the mean age of subjects was 50.3 years, and mean disease duration 22.2 years. A total of 106 (47.8%) stated physician-confirmed or suspected PsA. The mean self-reported BSA was 17.7, and mean DLQI 7.5 (Table I).
Table I. Characteristics of the patient and physician cohorts
The response rate for physicians was 17.9% (78 of 436 contacted; 67.9% females). Half of the respondents were dermatologists and half residents in dermatology. Of all physicians participating in the study, 74.4% worked in a hospital. The mean length of work experience in dermatology was 10.8 years. On average, 354 patients with psoriasis were treated per year (range 30–2,000); 59% of these were estimated to have moderate-to-severe psoriasis (BSA > 10 or PASI > 10 and DLQI > 10) (19), 35.2% were estimated to receive traditional systemic medications and 31.5% were estimated to receive biologicals (Table I). All respondents passed the fixed choice tasks.
The attribute regarded as most important in both cohorts was probability of PASI 90 response (patients: RIS 21.4, physicians: RIS 20.8, Fig. 1). Patients also attached great importance to mild AE (RIS 18.2), severe AE (RIS 14.2) and PASI 75 (RIS 12.5), whereas delivery method (RIS 7.7), treatment frequency (RIS 7.4), treatment location (RIS 5.5), time until response (RIS 5.5), frequency of laboratory tests (RIS 3.5) and cost to the healthcare system (RIS 4.2) were less essential from their perspective.
Fig. 1. Comparison of patients’ and physicians’ preferences. The probability of Psoriasis Area and Severity Index (PASI) 90 response was regarded as most important in both groups. Physicians were significantly more concerned about cost to the healthcare system and frequency of laboratory tests than patients, whereas mild adverse events (AE) and the treatment location were significantly more relevant to patients. Differences in Relative Importance Scores (RIS) were tested with analysis of variance (ANOVA). Bars: means with standard deviations. **p ≤ 0.01; ***p ≤ 0.001.
Physicians considered severe AE (RIS 14.9), mild AE (RIS 12.6) and cost (RIS 13.8) highly relevant, and placed less value on all other process attributes (delivery method: RIS 7.8, treatment frequency: RIS 6.6, frequency of laboratory tests: RIS 4.4, treatment location: RIS 3.7) and time until response (RIS 5.1).
Comparison between the cohorts revealed that physicians were significantly more concerned about cost to the healthcare system (p < 0.001) and frequency of laboratory tests (p = 0.002) than were patients, while mild AE (p < 0.001) and treatment location (p = 0.001) were more relevant for patients.
Patients. With increasing age participants considered PASI 90 response as less important (Pearson’s correlations (PC) –0.193, p = 0.004, Fig. S1A), but were more concerned about mild AE (PC 0.176, p = 0.009) and treatment location (PC 0.137, p = 0.041; β = 0.162, p = 0.045 in regression models, Table SIII). Efficacy also became less relevant with increasing disease duration (PASI 75: PC –0.140, p = 0.037; PASI 90: PC –0.207, p = 0.002), whereas safety gained importance (mild AE: PC 0.164, p = 0.015; severe AE: PC 0.138, p = 0.04; β = 0.163 p = 0.043; Fig. S1B, Table SIII). Increasing disease severity (increasing BSA) was associated with decreasing concern about severe AE (PC –0.148, p = 0.028; β = –0.145, p = 0.036). Participants with PsA were less interested in time until response than participants with-out this comorbidity (RIS 4.7 vs. 6.2, p = 0.004; Fig. 2; β = –0.199, p = 0.004). Participants recruited via the patient organization attached greater importance to mild AE (RIS 21.4 vs. 17.2, p = 0.027) and severe AE (RIS 17.0 vs. 13.2, p = 0.031), but were less interested in PASI 90 (RIS 15.8 vs. 23.2, p = 0.001) and time until response (RIS 4.5 vs. 5.8, p = 0.024) than those recruited via the study centres. These differences may be attributable to the facts that participants from the patient organization were significantly older (p < 0.001) and had a longer disease duration (p < 0.001), a lower BSA (p < 0.001) and a lower DLQI (p = 0.001) than those from the study centres (Table SIV). Sex, income, education and DLQI had no significant impact on preferences.
Fig. 2. Impact of concomitant psoriatic arthritis (PsA) on patient preferences. Participants with PsA attached less importance to time until response than others. Differences in Relative Importance Scores (RIS) were tested with analysis of variance (ANOVA). AE: adverse events; PASI: Psoriasis Area and Severity Index; bars: means with standard deviations. *p ≤ 0.05.
Physicians. Severe AE gained importance with longer work experience (PC 0.261, p = 0.021; Fig. S2A). Accordingly, specialists in dermatology were more concerned about severe AE than were residents (RIS 18.0 vs. 11.8, p = 0.045). With an increasing proportion of patients on biologicals, cost to the healthcare system lost relevance (PC –0.231, p = 0.042), whereas mild AE became more important (PC 0.257, p = 0.023; Fig. S2B). Sex, workplace, numbers of patients with psoriasis and PsA per year and percentage with moderate-to-severe psoriasis had no impact on preferences. Regression analyses performed for the physician cohort did not reveal significant findings (data not shown).
This study shows that both patients with psoriasis and physicians are highly interested in safety and efficacy of systemic treatments. In contrast to patients, physicians also attached great importance to the cost to the healthcare system. In Germany the cost of systemic antipsoriatics is covered by health insurance if they are prescribed “on-label”, which limits the importance of the cost to patients. However, physicians have to select an economically justifiable treatment, or they may be subject to liability claims. Physicians were also more concerned about the frequency of laboratory monitoring than were patients, because repeated laboratory tests may be cost-intense, time- and resource-consuming, and compensation for follow-up appointments may be reduced by health insurers. Furthermore, more need for monitoring may be perceived as an indicator of higher risk for AE.
Patients were more concerned about mild AE than were physicians. Mild AE are relatively frequent during systemic treatment, especially with traditional antipsoriatic medications (2, 20). Even if AE can often be managed well, they may cause considerable discomfort. It is noteworthy that patients were more willing to accept a relatively low risk of severe AE than a higher risk of mild AE. Clearly, their perceptions of AE depend on awareness and education.
Patient preferences for attributes of psoriasis treatments were evaluated using various methods, including DCE (17, 21–23). However, DCE comparing the preferences of patients with psoriasis and physicians are scarce. More than a decade ago a group in the UK used this method to investigate the treatment preferences of 227 dermatologists (24) and 126 patients (25). Attributes included in their survey were time to 50% improvement, time to relapse and risks of skin irritation, high blood pressure, liver damage and skin cancer. Both cohorts valued time to improvement more than time to relapse and ranked liver damage and skin cancer as the most important AE. However, the DCE did not take process attributes into account, and the outcome attributes do not reflect the features of biologicals. More recently, the preferences of 174 patients with psoriasis and 100 dermatologists for efficacy and safety of biologicals were compared using DCE (26). The attributes considered were location and coverage of the plaques, improvement in severity, and risks of tuberculosis, serious infections and lymphoma. Risk tolerance of AE was greater for patients than for physicians and efficacy improvements were highly valued by patients. Preferences varied depending on the location of the plaques and the severity of AE. This study provides valuable insights into patients’ and dermatologists’ preferences for outcome attributes of biologicals, but did not incorporate process attributes and attributes of other systemic medications.
Consistent with the results of our previous monocentric studies, patients’ preferences varied significantly depending on age, disease duration and severity. These findings, which underscore the importance of integrating individual characteristics into shared decisions, have been discussed previously (18, 27–29).
Within the physician cohort, longer work experience correlated with increased concern about severe AE. It is likely that experienced physicians encountered severe AE more often than those with less experience, and therefore took severe AE more seriously. Specialists in dermatology have to take full responsibility for the management of severe AE and their consequences, whereas residents can often refer to senior physicians.
Cost to the healthcare system became less relevant and mild AE more important with an increasing proportion of biological prescriptions. Physicians frequently disposing biologicals probably appreciate their good tolerability and safety profile. They experience a high net benefit from biologicals and therefore rate the cost as economically justifiable. Frequent application of biologicals interacts with more routine and less concerns in using them. Moreover, frequent prescribers of biologicals probably have accurately implemented treatment algorithms and documentation systems, which reduce concern about liability claims.
This study has several limitations. The DCE method is theoretical and can be cognitively challenging. Participants are obliged to select 1 of 2 scenarios even if they dislike both. In addition, our recruitment methods imply selection bias and the patient cohort was heterogeneous. Not all participants had moderate-to-severe psoriasis, had been treated by a dermatologist or had received systemic antipsoriatics. Almost 48% of subjects had physician-confirmed or suspected PsA. Compared with other studies (30, 31), this rate is very high, reflecting the limitations of patient self-assessment. Similarly, self-reporting of BSA implies a high risk of bias.
Levels ascribed to the risk of AE were based on the Summary of Product Characteristics. However, this does not allow distinct assessment of the effect size attributable to the intervention, since data corresponding to placebo in clinical trials are not incorporated and the differential or relative risks cannot be provided.
The choice of systemic treatment is influenced by a multitude of patient characteristics, e.g. age, comorbidities, course of disease, psychological strain, personal situation and individual needs. In our DCE physicians were asked to decide for an average patient with moderate-to-severe psoriasis. Treatment preferences for an individual patient may be divergent.
Our study included only dermatologists and residents in dermatology. Other specialists, e.g. general practitioners or rheumatologists, may have different treatment preferences (32). However, dermatologists are the major healthcare providers for patients with moderate-to-severe psoriasis in Germany (32). Fifty percent of our physician respondents were residents in dermatology who were not yet board certified. Depending on their training level and programmes, preferences for and concern about specific systemic treatments may differ significantly.
Associations between several patient characteristics and RIS were significant, but rather weak. In the physician cohort, correlations identified as significant in descriptive analyses could not be confirmed in regression models. These limitations, which may be attributable to the moderate sample sizes, underscore the necessity of verifying our findings in larger cohorts.
Major strengths of this study are that the preferences of patients and physicians for all systemic medications currently approved or expected soon for treatment of moderate-to-severe psoriasis were compared in a nationwide setting with a method resembling clinical decision-making. The DCE included all attributes with major relevance to patients and physicians, as determined in pilot tests, interviews and previous studies (17, 18). The current study shows that patients and physicians share high interest in efficacy and safety despite other heterogeneities in trade-off. The results emphasize that physicians need to explain PASI response rates and AE in detail to patients when discussing systemic treatment options. They must take both mild and severe AE seriously and counsel patients adequately regarding their management. Last, but not least, physicians must ask patients about their individual preferences, needs and fears, and integrate these aspects into the treatment decision in order to optimize patients’ treatment satisfaction (33).
Conflicts of interest. M-LS conducted clinical trials for Abbvie, Boehringer Ingelheim, Celgene, Eli Lilly, Janssen-Cilag, Merck, Novartis and UCB Pharma; obtained honoraria from Janssen-Cilag and Novartis; and received financial support for participation in conferences from Abbvie, ALK-Abello, Biogen Inc., Janssen-Cilag and MSD. MG received financial support for participation in conferences from Abbvie and obtained honoraria from Novartis. SG served as advisor and/or received speakers’ honoraria and/or obtained grants and/or participated in clinical trials of the following companies: Abbott/AbbVie, Almirall-Hermal, Amgen, Bayer Health Care, Biogen Idec, Bioskin, Boehringer-Ingelheim, Celgene, Centocor, Dermira, Eli Lilly, Foamix, Forward Pharma, Galderma, Hexal AG, Isotechnika, Janssen-Cilag, Leo Pharma, Medac, Merck Serono, Mitsubishi Tanabe, MSD, Novartis, Pfizer, Polichem SA, Sandoz Biopharmaceuticals, Schering-Plough, Takeda, Teva, UCB Pharma, VBL Therapeutics and Wyeth Pharma. MS obtained scientific support by Biogen, Pfizer and Novartis; was member of an advisory board of Abbvie, Celgene, Janssen Cilag, Lilly, Pfizer, MSD, Mundipharma, Novartis, Amgen, Leo and Actelion; served as speaker for Abbvie, Actelion, Janssen Cilag, Leo, MSD, Novartis and Pfizer; and conducted clinical studies for Abbvie, Actelion, Amgen, Galderma, GSK Janssen Cilag, Pfizer and Regeneron. MA served as consultant to or paid speaker for clinical trials sponsored by companies that manufacture drugs used for the treatment of psoriasis, including Abbvie, Almirall, Amgen, Biogen, Boehringer Ingelheim, Celgene, Centocor, Eli-Lilly, GSK, Janssen-Cilag, Leo, Medac, Merck, MSD, Novartis, Pfizer, Sandoz, Stiefel, UCB and Xenoport. WKP served as investigator for Abbvie, Boehringer-Ingelheim, Eli Lilly, Janssen-Cilag, Merck, Novartis, Pfizer and UCB Pharma; was member of an advisory board of Abbvie, Eli Lilly, LEO Pharma, MSD and Novartis; obtained honoraria from ALK-Abello, Abbvie, Janssen-Cilag, MSD, Novartis and Roche; and received support for conferences from Abbvie, Actelion, ALK-Abello, Alma Lasers, ARC Lasers, Asclepion, BMS, Celgene, Dermapharm, Dermasence, Eli Lilly, Galderma, GSK, Interlac, Janssen-Cilag, L’Oreal, La Roche Posay, LEO Pharma, Medac, Merck, MSD, Novartis, P&M Cosmetics, Pfizer, Roche and Stiefel.
The other authors have no conflicts of interest to declare.
The study presented here was not supported by pharmaceutical companies.
Financial support. This work was supported by the German Psoriasis Network “PsoNet” and by the patient organization for psoriasis Deutscher Psoriasis Bund e.V. Marthe-Lisa Schaarschmidt received a grant for postdoctoral lecture qualification from the University of Heidelberg and a grant for a research stay at the Institute for Health Services Research in Dermatology and Nursing (IVDP) in Hamburg from the Deutsche Stiftung Dermatologie.


 Click to show fullsize
Click to show fullsize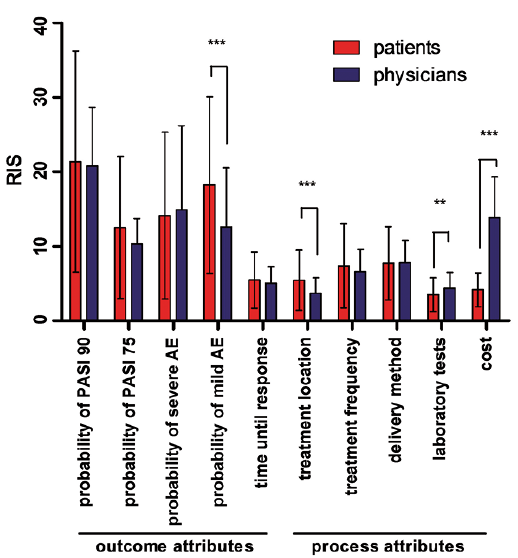 Click to show fullsize
Click to show fullsize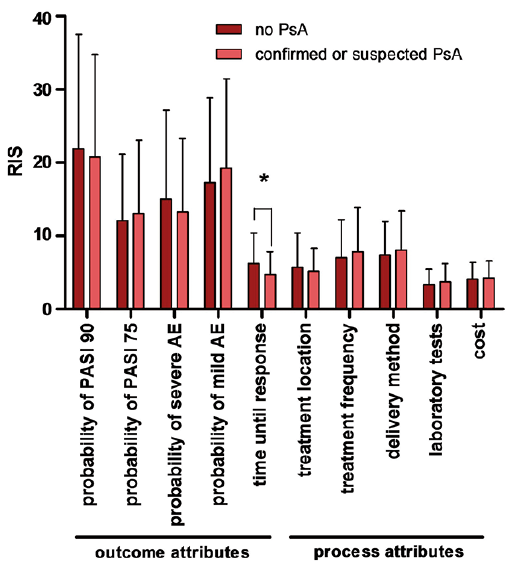 Click to show fullsize
Click to show fullsize