


1Molecular Oncology Group, CRUK Manchester Institute, University of Manchester, Wilmslow Road, Manchester, UK, 2QIMR Berghofer Medical Research Institute, Cancer and Population Studies, Brisbane, QLD, Australia, 3St George’s Hospital, London, and 4Histopathology, Royal Surrey County Hospital, Egerton Road, Guildford and Division of Clinical Medicine, University of Surrey, Guildford, Surrey, UK. E-mail: Adele.Green@qimrberghofer.edu.au
Accepted Nov 24, 2017; Epub ahead of print Nov 28, 2017
Cutaneous melanoma is a heterogeneous cancer that varies in its clinical characteristics and genetic alterations. While general features like size can give clues to likely prognosis, histopathologic appearance remains the gold standard for assessing cutaneous melanoma. Numerous histopathologic subtypes have been described, but the most common are superficial spreading melanoma (SSM) (60–80%), nodular melanoma (NM) (around 15%) and lentigo maligna melanoma (LMM) (5–15%) (1, 2). Of these, NM has the poorest outcome.
There has long been debate over whether NM’s poor prognosis signifies a distinct, inherently ‘aggressive’ entity (3) or if it simply reflects higher median thickness at diagnosis than other subtypes (4, 5). While current international classification (6) favors the latter, there remains compelling evidence that NM is unique in its clustering of high-risk features such as high mitosis rates (7) and ulceration (8), and in its lethality (9). We undertook a detailed evaluation of NM as a possible histopathologic entity in a collaborative study between England and Australia. We hypothesised that if they were a distinctly aggressive subtype, then from the outset when relatively thin, primary NMs would be more mitotic than other subtypes of equal thickness. We further tested this hypothesis by estimating disease-free survival (DFS) rates according to histological subtype in subgroups of equal thickness among the Australian study patients.
Patients aged 16–89 years, newly diagnosed with invasive, clinical stage IB or II cutaneous melanomas (6) in 2010–2014 were eligible for inclusion. In England, patients were ascertained at St George’s Hospital, London, with pathology review. In Australia, patients were diagnosed in primary care, regional or tertiary hospitals in Queensland (10). The study was approved by institutional ethics committees.
Subtype, site, thickness (mm), mitotic rate (per mm2 or per 10 hpf) and ulceration (present vs absent) were obtained from histopathology reports. We classified tumor thickness as > 0 to 2 mm (no stage IA and too few stage IB tumors ≤ 1 mm for meaningful analysis), > 2 to 4, and > 4 mm, and mitotic rates per mm2 as < 1, 1–< 2, 2 to 6, > 6 to give adequate numbers per category (n = 147 (10%) had 0 mitoses). Outcomes for English patients were not available, but were obtained for all Australian patients to August 31, 2017 via patient self-report, supplemented by systematic follow-up for melanoma recurrence or death in patients’ clinical records and the Queensland Cancer Registry. Differences in age, sex and histopathologic characteristics between melanoma patients diagnosed in England and Australia were assessed using chi-squared tests of homogeneity. Mean log-transformed mitotic rates of NMs adjusted for age, sex, thickness, ulceration, and country were compared with corresponding rates of SSM, LMM and ‘other’ (comprising unknown 55%, desmoplastic 14%, acral lentiginous 10%, naevoid 9%, other 11%) subtypes within categories of thickness. Differences between the adjusted least-squares means of log-transformed mitotic rates and between DFS rates were tested and analyses were performed in SAS 9.4.
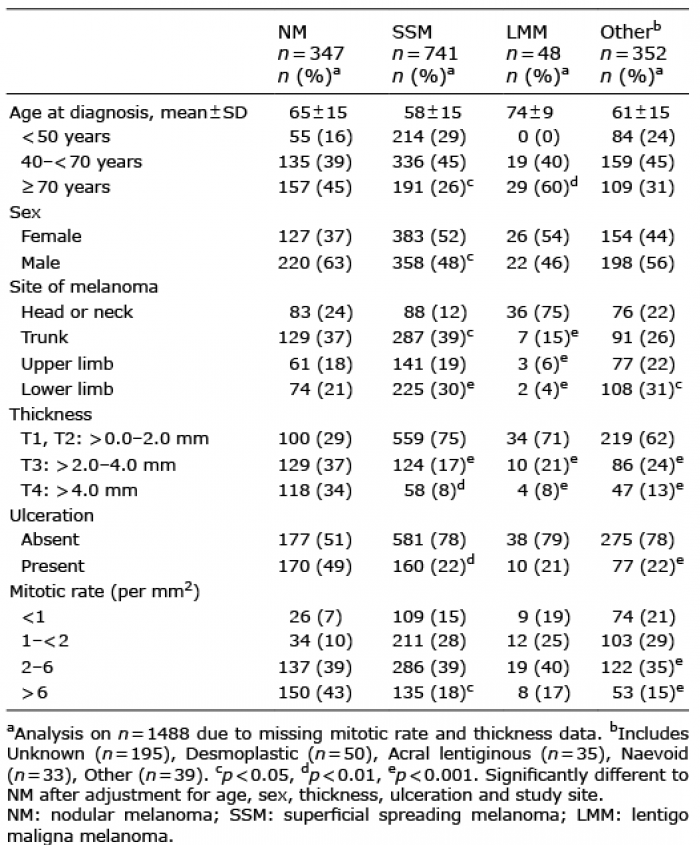
There were 709 eligible patients with 724 melanomas diagnosed 2010–2014 in the English series (mean age 60 years, 51% male) and 789 patients from Australia (mean age 62 years, 57% male). More melanomas occurred on the lower limb in England and head and neck in Australia (p < 0.003) and melanomas were thicker at diagnosis in England (3.15 ± 3.57 mm) than Australia (1.99 ± 1.67 mm) (p < 0.0001). SSM comprised 57% and 43% of the English and Australian series, respectively, nodular 24% and 22%, LMM 3% in both, and other subtypes, 14% and 26% respectively (p < 0.0001). The two series were combined since the same factors were associated with NM in both (Table SI), namely older age, male sex and head and neck location versus SSM, and thicknesses > 1 mm in relation to all subtypes (Table I). Ulcerated and highly mitotic (> 6 per mm2) melanomas were more likely to be nodular than another subtype.
Table I. Characteristics of stage IB, II melanomas in English and Australian patient samples combined
On average, the English melanoma patients had thicker lesions at diagnosis than the Australian patients (Table SII) and this was also true for each sex (median 2.2 mm vs 1.7 mm in males; 1.7 mm vs 1.3 mm in females). When mitosis rate was examined in relation to categories of thickness, thinner (≤ 2 mm) nodular subtypes had higher rates than all other subtypes ≤ 2 mm and except for LMM, differences were significant (Table II, Table SII). However for melanomas > 2 mm thick, there were no significant differences in mitosis rates between nodular, SSM or LMM subtypes; only remaining other subtypes had lower mitosis rates than NMs (Table II).
Table II. Mitotic rate in nodular melanomas (NMs) compared with other subtypes by thickness in English and Australian patient samples combined
Australian patients were followed-up after diagnosis for 2.9 to 6.9 years. Among those with known melanoma subtype whose melanomas were thinner (≤ 2 mm), DFS was 82% for NM, substantially worse than 91% for SSM (p = 0.051) and 90% DFS for LMM (p = 0.089). In contrast, for melanomas > 2 mm thick, there were no significant differences in DFS rates between nodular (66%), SSM (73%) (p = 0.95) or LMM (57%) (p = 0.41) subtypes.
The findings of higher mitosis rates in relatively thin (≤ 2 mm) NM compared with other subtypes (with the possible exception of LMM) support the hypothesis that primary NM is a histopathologic entity from the outset. The reason that the clear difference with LMM was not significant was most likely due to chance because of the small numbers of LMM cases (n = 48) compared with say SSM (n = 740), given that the distributions of mitotic rate, thickness > 4 mm and ulceration in LMM and other subtypes were almost identical. The similar mitotic rates across melanomas thicker than 2 mm regardless of subtype may reflect the erasing of radial growth phase by advanced melanomas and their convergence to thick, invasive tumours fitting the criteria for NM (11, 12). That it is among melanomas up to 2 mm thick where the nodular subtype is distinctive in its rapid growth rate is consistent with other large population series (9), and suggests the poor prognosis cannot be explained solely by greater measured thickness. These findings were borne out by actual survival data for the Australian patients with a mean 4.6 years follow-up, showing that patients with thin (up to 2 mm) NMs have substantially lower DFS compared with SSM and LMM of the same thickness, whereas there were no differences in DFS according to melanoma subtype among those with thicker melanomas.
The strength of this study is its large sample size and the inclusion of two international series. Its weakness is the lack of standardised reporting of histopathologic subtypes. Main differences were in the proportions of SSM (43% England, 57% Australia) and unknown (8% England, 15% Australia) subtypes, though proportions of NMs were almost the same (24% England, 22% Australia). We conclude that recognition of NM as a high-risk histopathologic entity is clinically most important for thinner (< 2 mm) melanomas. Since the vast majority of today’s melanomas are thin when diagnosed, identification of NM should remain a valuable aid to clinicians to predict outcome and guide patient management.
We thank Julia Newton-Bishop for helpful input and discussion.
The work was supported by Cancer Research UK (Ref C5759/A20971) and NHMRC Program Grant 1073898.


 Click to show fullsize
Click to show fullsize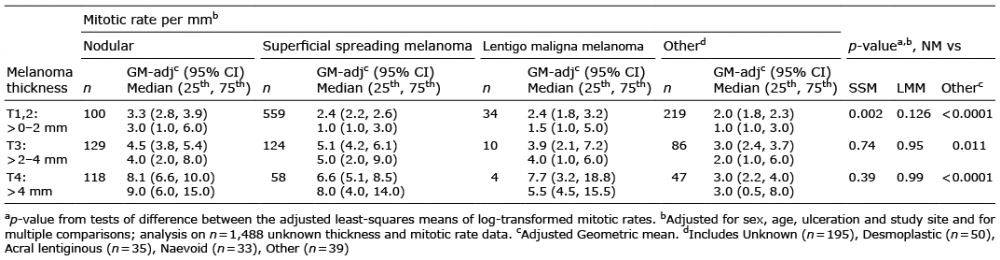 Click to show fullsize
Click to show fullsize