


1Department of Dermatology, University of Poitiers, Poitiers, 2Department of Dermato-Oncology, and 3SEME, CIC 1413, CRCINA Inserm 1232, CHU Nantes, Nantes, France
#These authors contributed equally and should be considered as first authors.
Nivolumab response rate is 40% in metastatic melanoma. Few studies have evaluated pre-treatment biomarkers predictive of response. The aim of this study was to identify potential peripheral blood biomarkers associated with survival in patients with advanced melanoma treated with nivolumab. All advanced melanoma cases treated with anti-programmed cell death protein 1 (anti-PD1) over a 3-year period in the Dermato-Oncology Department, Nantes, France were identified. For each case, 9 potential blood biomarkers were identified. Bivariate and multivariate analyses, adjusted for the American Joint Committee on Cancer (AJCC) classification stage, Eastern Cooperative Oncology Group (ECOG) performance status, lactate dehydrogenase (LDH) level and failure to respond to first-line therapy, were used to test the association between biomarkers and overall survival (primary outcome) or progression-free survival (secondary outcome). Increased monocyte count, leukocyte/lymphocyte ratio and neutrophil/lymphocyte ratio were significantly associated with decreased overall survival after bivariate and multivariate analyses. Increased monocyte count was also significantly associated with decreased progression-free survival. These blood variables are easily measured and could help to predict patient response before the introduction of anti-PD1 therapy.
Key words: nivolumab; anti-PD1; melanoma; biomarkers; predictive.
Accepted Dec 20, 2017; Epub ahead of print Dec 20, 2017
Acta Derm Venereol 2018; 98: xx–xx.
Corr: Brigitte Dréno, Department of Dermato-Oncology, University of Nantes, 1 place Alexis Ricordeau, FR-44093 Cedex 01, Nantes, France. E-mail: brigitte.dreno@wanadoo.fr
The introduction of new therapeutic agents has revolutionized the management of metastatic melanoma since 2011. Among these new agents are checkpoint inhibitors: human monoclonal antibodies targeting either programmed cell death protein 1 (PD1) or cytotoxic T-lymphocyte associated protein 4 (CTLA4), key players in immune regulation of tumour progression. PD1 is a T-cell receptor, which, when bound to PD ligand-1 (PDL1) or -2 (PDL2) on tumour cells, causes down-regulation in T-cell-mediated immune response.
Nivolumab is one of the 2 anti-PD1 monoclonal antibodies currently available on the market, which constitute the treatment of reference in advanced melanoma. In 2015, a randomized controlled trial demonstrated increased survival after one year in patients with metastatic melanoma without BRAF mutation treated with nivolumab compared with dacarbazine as first-line therapy (1). Similar results were seen when nivolumab was compared with other chemotherapy agents (dacarbazine or paclitaxel combined with carboplatin) used as second-line therapy after treatment with BRAF inhibitor or ipilimumab (2).
Anti-PD1 response rate is approximately 40%, meaning that patient selection is essential. There is a need for prognostic biomarkers, because administering treatment to patient non-responders is costly, exposes them to potential side-effects, and delays the introduction of alternative, potentially more effective, therapies. However, care must be taken to ensure that biomarkers are highly sensitive, in order to avoid the exclusion of patient responders.
Easily measurable, validated biomarkers predictive of anti-PD1 response are lacking. Current biomarker propositions include increased tumour expression of PDL1 (3) and tumour CD8 T-cell infiltration (4). Histological biomarkers require a tissue biopsy, which is not feasible in all patients because of the risk associated with certain visceral tumour locations and delays in obtaining results. Furthermore, the reliability of histological biomarkers is questionable because tumours are naturally heterogeneous, and histological samples are not representative of the whole tumour. Moreover, immunohistochemical methods are yet to be validated and homogenized between the different laboratories (5). The predictive value of PDL1 in melanoma metastasis and the definition of its range of positivity (5%, 10% of cells) are still discussed (5). To date, the most valuable finding is that an absence of PDL1 expression seems to be an argument for using a combination of 2 checkpoint inhibitors, anti-PD1 and anti-CTLA4.
Some prognostic blood biomarkers have already been identified for checkpoint therapies. High lactate dehydrogenase (LDH) (6) and high C-reactive protein (CRP) levels prior to anti-PD1 treatment are associated with poor outcomes (7). High lymphocyte count and high eosinophil count prior to first infusion have been shown to be associated with improved overall survival (OS) in metastatic melanoma treated with ipilimumab (anti-CTLA4 monoclonal antibody) (8) and pembrolizumab (anti-PD1 monoclonal antibody) (9). Inflammatory biomarkers, such as high neutrophil count and neutrophil/lymphocyte ratio (NLR), have been associated with decreased OS for ipilimumab (10, 11). These biomarkers have not been studied for anti-PD1 treatment in melanoma. Low absolute monocyte count (MC) is associated with increased OS in ipilimumab treatment (8). Studies evaluating peripheral blood biomarkers are lacking for anti-PD1.
This study examined the association between 9 peripheral blood parameters and the primary outcome, OS, in patients with advanced melanoma treated with anti-PD1. The secondary outcome was progression-free survival (PFS). The aim of this study was to identify potential, easy-to-use biomarkers predictive of patient response to anti-PD1 for advanced melanoma.
Patients were selected for this pilot monocentric retrospective study from the Melanoma Clinical Investigation Research Network (RIC-Mel), a French prospective cohort of melanoma patients. Inclusion criteria were: age greater than 18 years, histologically proven unresectable stage IIIC or IV melanoma, according to the American Joint Committee on Cancer (AJCC) classification (12). All patients must have received at least one dose of nivolumab between 26 June 2013 and 6 January 2016 at Nantes University Hospital, France.
Exclusion criteria were lack of documented peripheral blood sample in the 2 months preceding anti-PD1 treatment. For PFS analysis, patients with grade 3 or 4 side-effects according to Common Terminology Criteria for Adverse Events (CTCAE) leading to nivolumab discontinuation were also excluded (13). All participants had provided written informed consent for use of their clinical and biological data for the purposes of scientific research upon inclusion.
Nivolumab was administered intravenously at a dose of 3 mg/kg every 2 weeks, in accordance with the European Medicine Agency marketing authorization.
Data collected for each patient were: sex, date of birth, primary tumour characteristics (histological type, Breslow thickness, mitotic index, ulceration and BRAF status), pre-treatment AJCC stage, ECOG performance status (PS) and first-line therapy, if applicable.
For each patient included, a pre-treatment blood sample taken during the 2 months preceding nivolumab introduction, was identified. In the case of multiple blood samples, the most recent was selected. Biological tests were performed in several different laboratories including the Haematology and Biochemistry Department at Nantes University Hospital. Results were collected taking into account the normal ranges for each laboratory. Nine values were considered: leukocyte count, lymphocyte count, leukocyte/lymphocyte ratio (LLR), neutrophil count, NLR, MC, eosinophil count, LDH and CRP.
Standard imaging follow-up included a head, chest, abdomen and pelvis Computed tomodensitometry (CT) prior to treatment and every 2 months during treatment. Treatment response was defined according to RECIST (Response Evaluation Criteria in Solid Tumours) (13). RECIST scores were collected for all CT scans for each patient and therapeutic response was classed as progressive or non-progressive. A non-progressive response was then further defined as stable, partial or complete response. As part of usual practice in the Dermato-Oncology Department at Nantes University Hospital, all patients with complete radiological response underwent positron emission tomography (PET) and a CT brain, which was repeated 3 months later to confirm the absence of disease. In the event of disease-free imagery, treatment was discontinued. Three-monthly surveillance PET and CT brain scans were then performed for at least 1 year.
OS, the primary outcome, was defined as the number of days from the first dose of nivolumab to the date of death or to the date of analysis (15 April 2016) if the patient was still alive. PFS, the secondary outcome, was defined as the number of days from the first dose of nivolumab to the date of progression or death or, to the date of analysis if no progression was observed.
Descriptive statistics were used to present epidemiological data and disease-specific information. Bivariate Cox proportional hazard analyses were used to estimate risk factor associations between each biomarker and OS or PFS. Results were described by hazard ratios with 95% confidence intervals (95% CI) and p-values. For multivariate analysis, data were adjusted according to previously identified prognostic markers (AJCC stage, ECOG PS, LDH level and failure to respond to first-line therapy) and analysed using a Cox regression model.
All analyses were conducted using R statistical software version 3.12. p-values less than 0.05 were considered statistically significant.
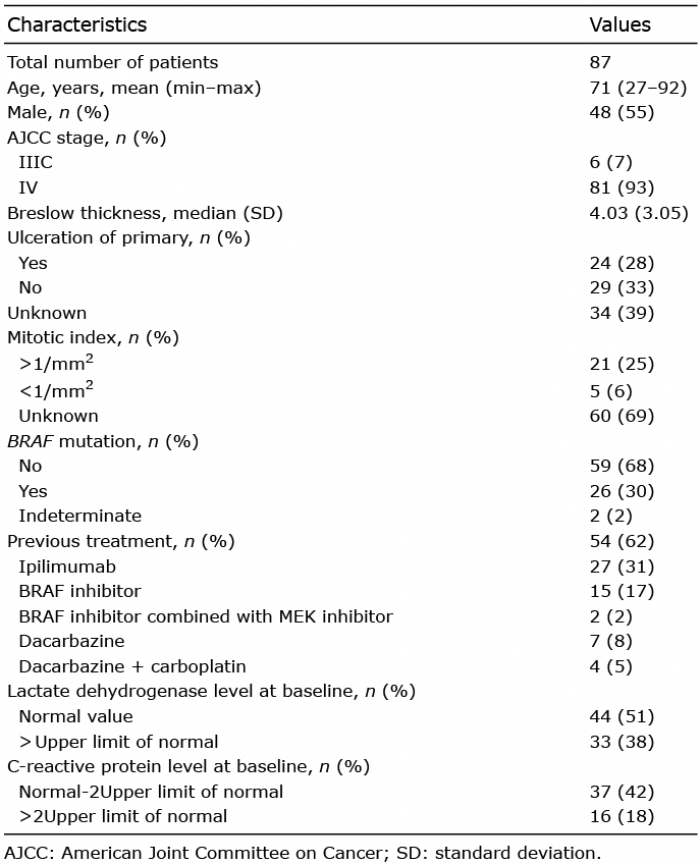
Eighty-seven patients fulfilled the inclusion criteria and were analysed for OS. Epidemiological data and primary tumour characteristics for OS are presented in Table I. Median age was 71 years, 48 patients were male. Mean Breslow thickness was 4.03 mm. Ulceration was seen in 24 patients (28%). Histological type was superficial spreading melanoma in 30% of cases (n = 26), nodular melanoma in 20% (n = 17), mucosal melanoma in 11% (n = 10), acro-lentiginous melanoma in 9% (n = 8), choroidal melanoma in 3% (n = 3), and other subtype in 5% (congenital naevus melanoma (n = 1), desmoplastic (n = 1), spitzoide naevus melanoma (n = 2)). Five percent of patients (n = 4) had an unclassifiable tumour type, and primary melanoma type was unknown in 11% (n = 10). For 5 patients, initial histological data of primary melanoma were missing at the time of diagnosis of metastatic disease and, despite efforts to contact general practitioners, histology laboratories and surgeons, remained unknown. Thirty percent of patients (n = 26) were found to be positive for BRAF mutation.
Table I. Epidemiological data
Nivolumab was used as first-line therapy in 33 patients. First-line therapy for the remaining 54 patients was BRAF inhibitor in 17% (n = 15), combined BRAF inhibitor/MEK inhibitor in 2% (n = 2), ipilimumab in 31% (n = 27), dacarbazine in 8% (n = 7) and combined dacarbazine/carboplatin in 5% (n = 4). No other anti-cancer treatment was administered concomitantly with nivolumab.
ECOG PS was 0 (n = 75), 1 (n = 7), 2 (n = 4) and 3 (n = 1). Median (standard deviation (SD) OS was 225 ± 100 days. Nineteen patients died during the study. After exclusion of 3 patients because of grade 3 or 4 side-effects (suspicion of drug-induced skin reaction, autoimmune pneumonitis and third-degree atrioventricular block) leading to discontinuation of treatment, 84 patients were analysed for PFS. Median ± SD PFS was 157 ± 115 days. Disease progression was observed in 42 patients. At the date of data analysis, mean follow-up was 227 days, 48% of patients were considered as having “non-progressive” disease (n = 42), of which 9 were considered as having a “complete” response to treatment.
Pre-treatment blood samples were used to extract values for each potential biomarker: leukocyte count, lymphocyte count, leukocyte/lymphocyte ratio (LLR), neutrophil count, NLR, MC, eosinophil count, LDH and CRP.
Bivariate analysis revealed a statistically significant relationship between decreased OS and an increase in the following biomarkers, expressed in absolute count (Table II): leukocyte count (p = 0.01; HR 1.13; 95% CI, 1.06–1.22), LLR (p = 0.01; HR 1.11; 95% CI, 1.04–1.17), neutrophil count (p = 0.01; HR 1.16; 95% CI, 1.08–1.26), NLR (p = 0.01; HR 1.08; 95% CI, 1.02–1.15), MC (p = 0.01; HR 4.31; 95% CI, 1.46–12.74), LDH (p = 0.01; HR 1.31; 95% CI, 1.18–1.45) and CRP (p = 0.01; HR 1.01; 95% CI, 1.01–1.02). Elevated eosinophil count (p = 0.04; HR 0.01; 95% CI, 0.01–0.86) was the only biomarker significantly associated with increased OS. Lymphocyte count was not significantly associated with OS. Similar results were found for PFS, except for eosinophil count, which was not statistically significant (Table II).
Table II. Overall survival and progression-free survival for bivariate and multivariate analysis
Pre-treatment LDH values were unavailable for 11 patients. Multivariate analysis was therefore performed for 76 patients in OS and 73 patients in PFS.
The results are shown in Table II. A statistically significant relationship was observed between a decrease in OS and an increase in the following biomarkers expressed as absolute values: LLR (p = 0.02; HR 1.11; 95% CI, 1.02–1.21), NLR (p = 0.02; HR 1.12; 95% CI, 1.02–1.23) and MC (p = 0.01; HR 6.31; 95% CI, 1.5–26.59).
Decreased PFS was significantly associated with increased MC (p = 0.04; HR 3.5; 95% CI, 1.01–12.1) (Table II).
In this study, high leukocyte/lymphocyte ratio, neutrophil/lymphocyte ratio and monocyte count were shown to be independently associated with decreased OS according to bi- and multi-variate analysis in patients with advanced melanoma treated with anti-PD1. Only increased MC was significantly associated with decreased PFS for adjusted and non-adjusted analysis.
The results of multivariate analysis appear, for the greater part, to be concordant with current literature for anti-CTLA4 treatment. Previous studies have demonstrated the poor prognostic value of high NLR in patients treated with ipilimumab (10, 11). Low MC has been shown to be associated with increased OS after treatment with ipilimumab (8). This study is the first to show LLR, NLR and MC as independent predictive biomarkers for anti-PD1 treatment in melanoma. In bivariate analysis, we confirm previous results published with anti-PD1 treatment (6, 7, 9). High LDH and high CRP were significantly associated with poor OS and PFS. High eosinophil count was significantly associated with increased OS and PFS.
Current predictive biomarkers for anti-PD1 treatment described in the literature are histological and require a tissue biopsy. Histological biomarkers are associated with a number of disadvantages: biopsy-associated risks, delays in obtaining results, lack of established normal value ranges and absence of validated immunohistochemical methods standardized across laboratories. This pilot study aims to identify easily measurable (via a peripheral blood test) predictive markers that could potentially be used to predict patient response. Such biomarkers are lacking for anti-PD1 therapy.
Current literature suggests an intimate relationship between chronic inflammation and tumour microenvironment (14). Although microenvironment observations must be differentiated from those of systemic biomarkers, interestingly, our significant results are markers of systemic inflammation and mobilization of the innate immune system. NLR describes relative changes in neutrophil count and lymphocyte count and is a well-validated predictive marker for visceral cancers and melanoma prior to ipilimumab treatment (10, 11). Monocytosis, although less studied, is also related to chronic inflammation and has been studied previously for other cancers (15, 16). NLR and MC reflect systemic inflammation, providing a biological explanation for our results.
OS was chosen as the primary outcome marker because it is generally accepted as the reference outcome marker in immunotherapy treatment. Its weakness, however, is that it does not differentiate the effects of treatments used after anti-PD1, and includes deaths from non-cancer-related causes. PFS is now accepted by the FDA as a surrogate biomarker for OS (17). It was chosen as the secondary outcome marker because it is particularly well adapted for shorter studies, metastatic disease and measures directly the effect of anti-PD1 without being affected by subsequent therapies. The weaknesses of PFS are that, firstly, it depends on the time of the re-evaluation and, secondly, it is considered less clinically relevant than OS. Interestingly, our study shows statistically significant results for MC for both OS and PFS, suggesting that this result is not only clinically relevant, but also directly related to nivolumab.
Despite the retrospective design, this study had a number of strengths. Patient inclusion was exhaustive and data were adjusted for previously identified prognostic factors (AJCC stage, ECOG PS, LDH level and failure to respond to first-line therapy). LDH was significantly associated with poor OS and PFS in bivariate analysis, validating our choice to use it as an adjustment factor. The use of OS as the primary outcome and PFS as the secondary outcome were also strengths. All patients were analysed in real-life situations and data were homogenized in PFS analysis by the exclusion of patients with grade 3 or 4 CTCAE. Continued follow-up of this study is required to confirm results. Performance status could also be considered. Finally, the large variability of our monocyte count hazard ratio may suggest a significant influence of other unaccounted for factors, highlighting the need for further studies examining PD1/PDL1 interactions.
Based on this pilot study, pre-treatment increased LLR, NLR and MC are independent biological markers associated with poorer outcome in patients with advanced melanoma treated with nivolumab. Not all patients respond to anti-PD1 treatment, and measures of PDL1 expression in tissue biopsies may not be accurate biomarkers. The biomarkers proposed here are accessible via a blood sample and could easily be used to improve patient selection, but require validation in larger multicentre trials.
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize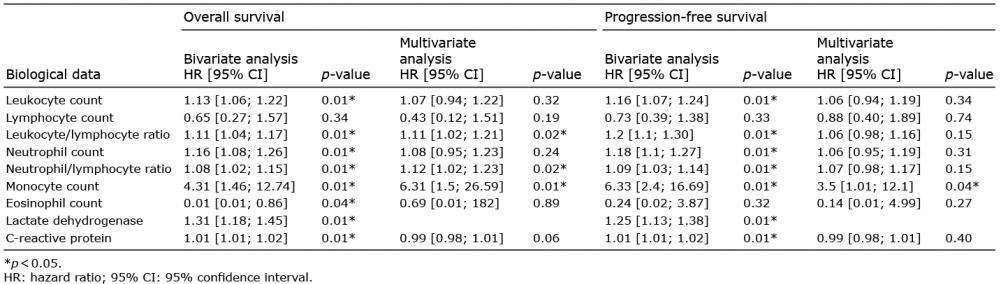 Click to show fullsize
Click to show fullsize