


Departments of 1Dermatology and 2Nuclear Medicine and PET Centre, Aarhus University Hospital, Aarhus, and 3Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, Denmark
The spleen is thought to play a role in atherosclerosis-associated immunity and cardiovascular research has indicated the existence of a cardio-splenic axis. The aim of this study was to assess splenic 18F-fluorodeoxyglucose uptake as a measure of systemic inflammation in patients with untreated psoriasis compared with historical controls assessed by positron emission tomo-graphy-computed tomography. Patients with moderate-to-severe psoriasis (n = 12, age 61.4 ± 4.1 years, 83% men, mean Psoriasis Area Severity Index score of 14.5) and controls (n = 23, age 60.4 ± 4.5 years, 87% men) were included in the study. Splenic inflammation was measured using the background-corrected spleen-liver-ratio (SLR) based on mean standardized uptake values. Mean ± SD SLR was increased in patients with psoriasis compared with controls (0.94 ± 0.11 vs. 0.82 ± 0.08; p = 0.001). SLR was significantly associated with aortic inflammation. These results support the existence of systemic inflammation in patients with psoriasis, and provide the rationale for a mechanistic link between psoriasis-driven inflammation and cardiovascular comorbidity through a spleen-atherosclerotic axis.
Key words: positron emission tomography computed tomo-graphy; inflammation; spleen; psoriasis; vascular inflammation;
atherosclerosis.
Accepted Dec 20, 2017; Epub ahead of print Dec 20, 2017
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Kasper F. Hjuler, Department of Dermatology, Aarhus University Hospital, P.P. Orums Gade 11, Bldg. 15, DK-8000 Aarhus C, Denmark. E-mail: kasperfjellhaugenhjuler@gmail.com
Psoriasis is a common immune-mediated inflammatory disease that affects the skin, nails and joints. However, in recent years the disease has also been linked (directly or indirectly) to a host of comorbidities, with a strong focus on cardiovascular comorbidities. For example, psoriasis has been associated with an increased prevalence of all traditional cardiovascular risk factors (1), with premature coronary artery disease (2), and an increased risk of major adverse cardiovascular events and cardiac mortality (3, 4). Exploratory studies indicate shared immunological mechanisms in psoriasis and atherosclerosis (5, 6), Furthermore, patients with psoriasis exhibit increased inflammation of the aortic wall (7–9). In addition, it has been hypothesized that an increased systemic inflammatory load in patients with psoriasis, at least in part, causes premature atherosclerotic disease (10). Some studies show evidence of systemic inflammation in psoriasis, whereas other studies rebut these findings (11). A recent meta-analysis of soluble biomarkers of systemic inflammation shows evidence of mild systemic inflammation in patients with psoriasis compared with healthy control subjects (12). Taken together, it remains unclear to which extent psoriasis causes systemic inflammation, whether this is clinically relevant and if it is causally associated with premature development of cardiovascular disease.
Since the approval of the first commercial system in 2001, 18F-fluorodeoxyglucose-positron emission tomography computed tomography (FDG-PET/CT) has become a valuable imaging method in oncology. In addition, this modality is increasingly being used as an imaging tool for inflammatory conditions in general. Given the focus on inflammation in vascular plaque formation, FDG-PET/CT imaging has been investigated as an imaging tool in atherosclerosis (13), and it has been shown that FDG accumulation correlates with atherosclerotic plaque inflammation (14, 15). Preliminary insights indicate an association between FDG uptake in the vascular wall and increased risk of future cardiovascular events (16, 17). In addition, splenic inflammation can be visualized by FDG-PET/CT. Splenic FDG uptake is increased in inflammatory, malignant and infectious diseases, and the spleen-to-liver ratio (SLR) correlates with the peripheral neutrophil count (18–22). As shown in a human autopsy study, the spleen may play a role in activating and directing monocytes to the heart following ischaemic events (23). Furthermore, it has been shown that the activation state of the spleen may be closely related to proinflammatory gene activation within circulating leukocytes and that splenic FDG uptake independently predicts the risk of cardiovascular events (24). Based on preclinical and clinical data, a central role of the spleen in the progression of atherosclerotic disease has been suggested and conceptualized as the “cardio-splenic axis” (24–26). This concept entertains the hypothesis of a spleen-atherosclerotic plaque crosstalk.
We recently showed that aortic inflammation and subcutaneous adipose tissue inflammation, assessed by FDG-PET/CT, are significantly increased in patients with psoriasis compared with control subjects (9). The primary objective of the present study was to expand on these findings by assessing splenic FDG uptake as a measure of systemic inflammation in the same cohorts of patients with psoriasis and control subjects. A secondary objective was to investigate whether splenic inflammation is associated with aortic and subcutaneous adipose tissue inflammation.
The study was designed as an open-label, controlled clinical study. We utilized a previous study cohort, established between January 2015 and May 2016 at a single tertiary dermatology university hospital clinic (9). Imaging investigations were performed at a university hospital nuclear medicine PET centre.
Consecutively enrolled patients with moderate-to-severe psoriasis were examined with FDG-PET/CT and compared with a retrospectively age- and sex-matched control group.
The study was conducted in compliance with the principles of the Declaration of Helsinki. The protocol was reviewed and approved by the Central Denmark Region Committees on Biomedical Research Ethics and by the Danish Data Protection Agency. All consecutively enrolled participants provided written informed consent prior to any study procedures. The Committee on Research Ethics waived the requirement for informed consent regarding the retrospectively matched control group.
Details of the inclusion and exclusion criteria have been described previously (9). Briefly, patients aged between 50 and 70 years with moderate-to-severe psoriasis vulgaris, i.e. a Psoriasis Area Severity Index (PASI) score of at least 10, were eligible for study inclusion if they had no concurrent inflammatory or autoimmune diseases, no history of malignancies within the past 5 years (excluding localized non-melanoma skin cancer) and no contraindications for the clinical use of FDG-PET/CT. Where appropriate, patients with psoriasis were entered into a pre-study washout period, wherein all active anti-psoriatic topical and systemic therapies were discontinued according to pre-specified time frames. The control group comprised age-matched men and women aged ≥ 18 years who were examined at the same centre, using the same technique as that employed for the study cases. The control subjects were either patients with localized melanoma or patients with localized stage 1 penile cancer. Additional eligibility criteria and details on clinical assessments are shown in Appendix S1.
Whole-body FDG-PET/CT in patients with psoriasis was performed using a combined PET/CT scanner (GE Discovery 690, General Electric Medical Systems, Milwaukee, WI, USA). Control subjects were either scanned on the same GE Discovery 690 PET/CT or on a Siemens Biograph 64 PET/CT (Siemens, Germany).
A detailed description of the scan parameters is provided in Appendix S1.
PET and CT data were fused and analysed with PMOD v3.703 (PMOD Technologies, Zurich, Switzerland). CT and PET images were reviewed for quality, and the images were manually co-registered to ensure optimal anatomical correlation. Image analysis was performed in accordance with recent nuclear medicine imaging guidelines by one expert observer (L.C.G.).
In accordance with previously published methodology the splenic volume was assessed in each CT examination by measuring: the maximal width of the spleen, determined as the largest diameter on any transverse section; the maximal thickness, defined as the largest distance between the inner and outer borders of the spleen perpendicular to the plane of the maximal width; and the thickness at the hilum, determined as the distance between the inner and outer borders of the spleen on a plane perpendicular to the splenic width and through the hilum (27).
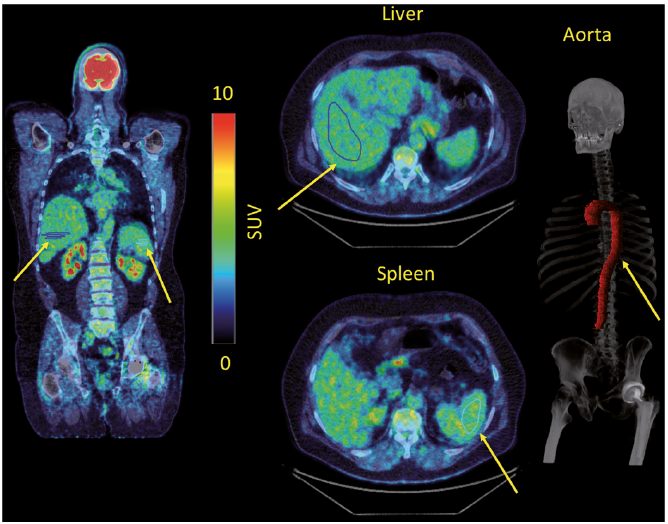
Splenic inflammation was measured using mean standardized uptake values (SUVmean) and maximal standardized uptake values (SUVmax) and the SLR in accordance with current recommendations and previously published methodology (18, 21, 22, 26). Spleen volume of interest (VOI)s were drawn on 5 adjacent axial slices covering the central part of the organ, whereas liver VOIs were drawn on 6 adjacent axial slices in the right lobe (Fig. 1). Vascular inflammation was measured using aortic SUVmax and the target-to-background ratio (TBRmax) of the whole vessel and aortic segments in accordance with recent nuclear medicine imaging guidelines (13) and previously published methodology (9, 28). The TBR was calculated from the ratio of the SUV of the aorta compared with background venous activity, derived from the superior vena cava, for correction of aortic values.
Subcutaneous adipose tissue inflammation was assessed as SUVmax. A detailed description of the aortic wall and subcutaneous adipose tissue image analyses has been published previously (9).
Fig. 1. Coronal and transverse PET images with volume of interests drawn in the spleen and the liver in a representative patient with psoriasis. Arrows indicate the region of interest in the spleen, liver, and aorta.
Summary statistics were expressed as mean ± standard deviation (SD) for normally distributed variables. Patient characteristics were compared using Student’s t-test for continuous variables and Pearson’s χ2 for categorical variables. The primary outcome measure was the mean difference in SLR between the patients with psoriasis and the control group. Between-group differences were compared using the unpaired t-test with equal variances. A multivariate analysis of covariance (ANCOVA) was performed as a secondary analysis to test the effect of the continuous covariates of age and body mass index (BMI) and categorical variable sex on difference in SLR.
Associations were tested using Pearson’s correlation coefficient. Data were tested for normality using the D’Agostino-Pearson normality test (see Appendix S1 for details). The level of statistical significance was set at α = 0.05. Graphs and statistical analyses were made in GraphPad Prism version 7.0 (GraphPad software, San Diego, CA, USA) and STATA/IC ver. 12.1 for Mac (StataCorp LP, College Station, TX, USA).
Included in the study were 12 subjects with moderate-to-severe psoriasis and 23 controls. Table I shows the characteristics of the included study subjects. The mean ± SD splenic total volume was slightly higher, albeit insignificantly so, among psoriasis patients compared with controls (269.5 ± 95.6 cm3 vs. 224.5 ± 62.8 cm3; p = 0.11).
Table I. Patient characteristics
Further imaging analyses are shown in Table II. FDG uptake in aortic segments and subcutaneous adipose tissue has been published previously (9). Mean SLRmean was increased in patients with psoriasis compared with controls (mean ± SD SLR 0.94 ± 0.11 vs. 0.82 ± 0.08; p = 0.001 (Fig. 2).
Table II. 18F-fluorodeoxyglucose-positron emission tomography/computed tomography imaging results
Fig. 2. Mean spleen-liver ratio based on mean standardized uptake values (SUVmean) in psoriasis and control subjects. The lines indicate median values, and the boxes extend from the 25th to 75th percentiles. The whiskers indicate min to max range. The mean is indicated by “+”.
A significant association between SLR and aortic mean whole vessel TBRmax was found in the populations overall (Pearson r = 0.51; p = 0.002) and in the subjects with psoriasis (Pearson r = 0.65; p = 0.02) (Fig. 3A). No significant association between SLR and aortic mean whole vessel TBRmax was found in the control subjects (Pearson r = 0.16; p = 0.48). Comparable results were seen when assessing SLRmax based on spleen and liver SUVmax (see results in Appendix S2).
Fig. 3. Correlation between FDG uptake in spleen, arterial wall and subcutaneous adipose tissue. (A) Association between spleen–liver ratio based on mean standardized uptake values and aortic mean whole vessel target-to-background ratiomax among subjects with psoriasis and controls. Pearson r = 0.51; p = 0.002. (B) The association between spleen-liver ratio based on mean standardized uptake values and subcutaneous adipose tissue inflammation among psoriasis subjects and controls. Pearson r = 0.43, p = 0.01. Symbols represent individual patients and the line represents the linear association between variables.
A significant association between SLR and subcutaneous adipose tissue inflammation was found in the population overall (Pearson r = 0.43; p = 0.01), but no significant associations were found in either of the specific groups (Fig. 3B). No significant association was found between PASI score and SLR (Pearson r = –0.42; p = 0.18) or between psoriatic disease duration and SLR (Pearson r = 0.40; p = 0.20).
After adjusting for BMI, age and sex using a multivariate ANCOVA regression model, psoriasis remained significantly associated with elevated SLR levels (F = 3.79, p = 0.01). Furthermore, no difference was seen between PET investigations in controls using GE Discovery 690 PET/CT vs. Siemens Biograph 64 PET/CT (mean ± SD SLRmean 0.81 ± 0.07 vs. 0.83 ± 0.09; p = 0.60).
This is the first clinical study to show increased splenic inflammation in patients with moderate-to-severe psoriasis compared with control subjects. It also shows that splenic inflammation is associated with aortic inflammation in patients with psoriasis. Taken together with our previous findings of increased global arterial and subcutaneous adipose tissue inflammation in this cohort, these data provide evidence to support a role of systemic inflammation and a likely role of an interplay between the spleen and atherosclerotic plaque in patients with psoriasis.
The hypothesis that psoriasis may be a systemic inflammatory disease rather than a localized disease of the skin and nails has gained much attention in recent years, but the concept rests mainly on evidence from soluble blood biomarker studies and on deductive reasoning based on observational registry data (29). Most published studies on soluble biomarkers indicate a moderate role of systemic inflammation in psoriasis (1, 12). However, these studies have a number of limitations in addition to unknown predictive values and the non-specificity of certain biomarkers. Nevertheless, systemic inflammation in psoriasis has become a key suspected culprit in the link between psoriasis and cardiovascular comorbidities, as well as in the reasoning on the role of psoriasis as an independent risk factor for future cardiovascular events that is seemingly unrelated to the traditional cardiovascular risk factors. Although this hypothesis has gained considerable momentum, the reported cardiovascular effects of dampening the systemic inflammation with tumour necrosis factor-alpha (TNF-α inhibitors have been somewhat conflicting (30, 31).
FDG-PET/CT provides a direct measure of metabolic activity in vessels and other tissues. FDG is a radiolabelled glucose analogue that is taken up by tissues with high metabolic activity, such as inflammatory active tissue and tumour cells. Accumulation of FDG in the arterial wall localizes to macrophage-rich regions and correlates with immunohistochemical staining and gene expression for macrophage-specific markers, as well as with soluble markers of inflammation (32, 33). Furthermore, arterial FDG uptake increases in proportion to atherosclerotic risk factors, with plaque morphological complexity, and after atherothrombotic events (34). It has been shown that FDG-PET/CT significantly improves cardiovascular disease prediction beyond that of traditional risk factor scoring, and that FDG-PET/CT imaging provides prognostic information adding to that which may be obtained using soluble biomarkers (16, 17, 35, 36).
The spleen is a key organ in erythrocyte homeostasis and plays important roles in the immunological system. Leukocytes in the spleen include various subsets of T and B cells, dendritic cells and macrophages that initiate and control innate and adaptive immune functions.
It has been shown that splenic inflammation assessed by FDG-PET/CT is increased in patients with autoimmune and inflammatory diseases, and that the splenic FDG uptake correlates with measures of systemic inflammation (18–22). Furthermore, studies in murine models indicate a role of the spleen in atherosclerosis-associated immunity (25, 37). Human proof-of-concept studies show increased levels of splenic FDG uptake in patients with recent myocardial infarction and an association between splenic and arterial inflammation (38, 39). Emami et al. showed that aortic wall FDG uptake correlated with splenic FDG uptake in a large number of patients (n = 464). Moreover, in this study splenic FDG uptake appeared to be a predictor of future cardiovascular events. Taken together with the correlation between splenic and aortic inflammation, this entails that not only does the spleen react acutely to myocardial infarction, but it also appears to drive cardiovascular inflammation in a stable setting (24, 26). Thus, the results of the current study corroborate the existence of systemic inflammation in psoriasis beyond that ascertained in previous biomarker studies, and the current study provides the rationale for a mechanistic link between psoriasis-driven inflammation and cardiovascular comorbidity through a spleen-atherosclerotic axis.
In addition, we observed an increased volume of the spleen in patients with psoriasis compared with controls, albeit insignificantly so. Thus, a recent publication described increased spleen longitudinal diameter in patients with psoriasis compared with non-psoriatics, as well as an association between disease duration and splenic diameter (40). While this publication provided important quantative analyses of the spleen in psoriasis, our study extends these findings by providing functional imaging analysis, which quantifies the metabolic activity of the spleen.
Interestingly, we found no association between PASI scores and splenic inflammation. Hypothetically, a dose-response relationship between psoriasis severity and the inflammatory activation state of the spleen would be plausible. The absence of such correlation in our data may be due to the low variation in PASI scores and the limited number of subjects investigated. Another reason may be that PASI is not an optimal instrument for assessment of systemic inflammation in patients with psoriasis (41). This viewpoint is supported by the fact that studies with cardiovascular and systemic inflammatory outcomes show conflicting results when assessing the association with PASI (2, 8, 9, 31, 42, 43).
These findings are strengthened by the use of background-corrected ratios TBR and SLR rather than SUV. Thus, the use of a ratio between 2 measurements limits the effects on signal quantification of errors in patient weight and in the dose of radiotracer injected and of the imaging time-point (13). It has been shown that exclusive use of SUV does not reliably reflect tissue metabolic activity and that, especially, correlations between SUV in various tissues should be interpreted with caution due to a positive correlation between SUV and body weight (26, 44). Thus, and in agreement with recent literature (26), SLR and not SUV was the primary outcome measure in this study. Further methodological strengths of the present study include our use of robust splenic and liver SUVmean values, which reduces the risk of measurements based on single high pixel values; the analysis of the entire aorta without sampling of slices; the inclusion of untreated psoriasis patients with moderate-to-severe disease activity only; and the use of semi-automatic software for image analysis, which makes the results reproducible with a low risk of biased assessments. The findings remained significant after adjusting for age, sex and BMI.
The main limitations of the study include the small sample size, the open-label design, restricted age groups due to radiation exposure, and the use of historical control subjects for whom only limited medical data were available.
It is well known that psoriasis is associated with an increased risk of non-alcoholic fatty liver disease (NAFLD) (45). As the presence of NAFLD was not specifically assessed it cannot be ruled out that some patients with NAFLD may have been included in our study. Although contradictory results have been published, recent studies indicate that NAFLD may increase the liver FDG uptake, which may have caused us to underestimate the SLR in such patients (46, 47). In addition, 2 PET/CT systems were used. Comparable protocols were used, however, and no significant differences between results obtained from the 2 systems were noted.
Finally, although compelling interrelationships were observed between splenic activation and arterial inflammation, these relationships do not necessarily indicate causality.
In conclusion, our data provide evidence of increased splenic inflammation in subjects with moderate-to-severe psoriasis. Furthermore, we show that splenic activity correlates with aortic wall inflammation in subjects with psoriasis. These findings indicate clinically relevant systemic inflammation in patients with moderate-to-severe psoriasis. The cardio-splenic axis may mechanistically, at least in part, explain the epidemiological observation that patients with psoriasis have an increased risk of heart disease.
Funding. This study was supported by a grant from Pfizer (grant number WS2640077). Pfizer had no influence on the design of the study, the collection of data, the interpretation of the results, the preparation of the manuscript or the decision to submit for publication.
Disclosures. KFH reports research funding from AbbVie and honoraria as a consultant and/or speaker from AbbVie, Novartis and Eli Lilly; and travel grants from AbbVie, LEO Pharma, and Novartis, all unrelated to the submitted work. AE has received research funding from Pfizer and Eli Lilly, and honoraria as a consultant and/or speaker from Pfizer, Eli Lilly, Novartis, Galderma and Janssen Pharmaceuticals, and was previously employed by Pfizer. JN was employed according to the listed affiliation during all study activities except during the critical review process, at which time he was employed by Leo Pharma.
LI reports grants from AbbVie, Pfizer and Novartis; and has served as a consultant and/or a paid speaker for and/or participated in clinical trials sponsored by: Abbvie, Almirall, Amgen, Celgene, Centocor, Eli Lilly, Janssen Cilag, Leo Pharma, MSD, Novartis, Pfizer and UCB, all unrelated to the submitted work.


 Click to show fullsize
Click to show fullsize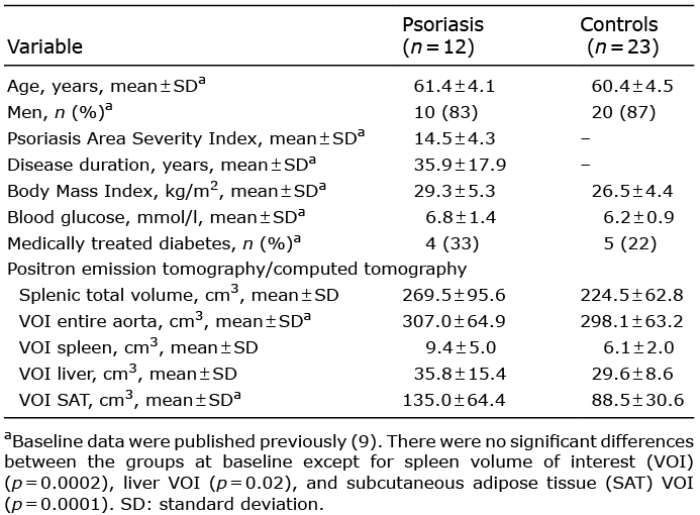 Click to show fullsize
Click to show fullsize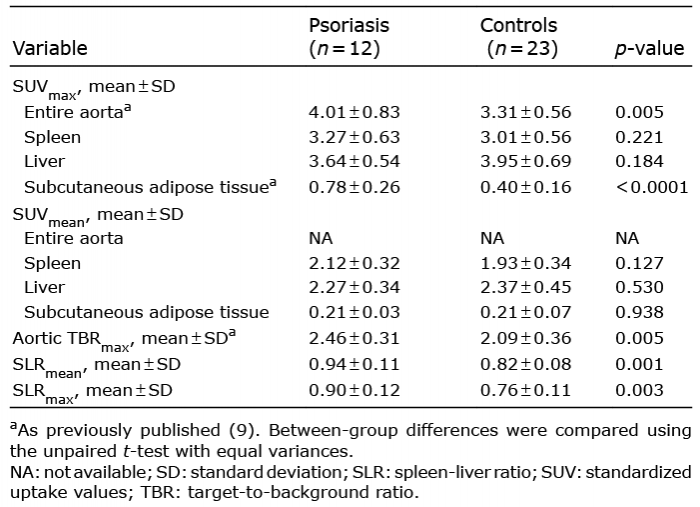 Click to show fullsize
Click to show fullsize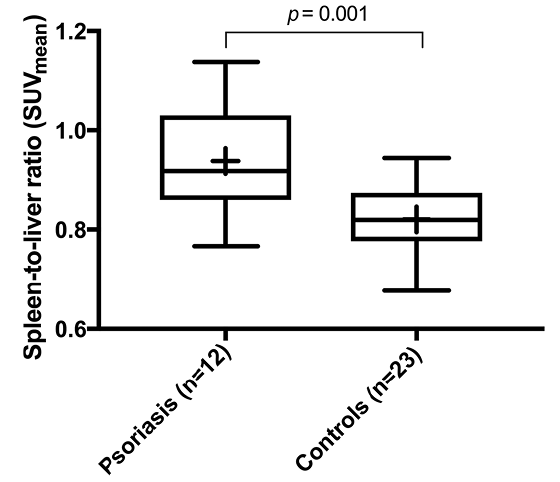 Click to show fullsize
Click to show fullsize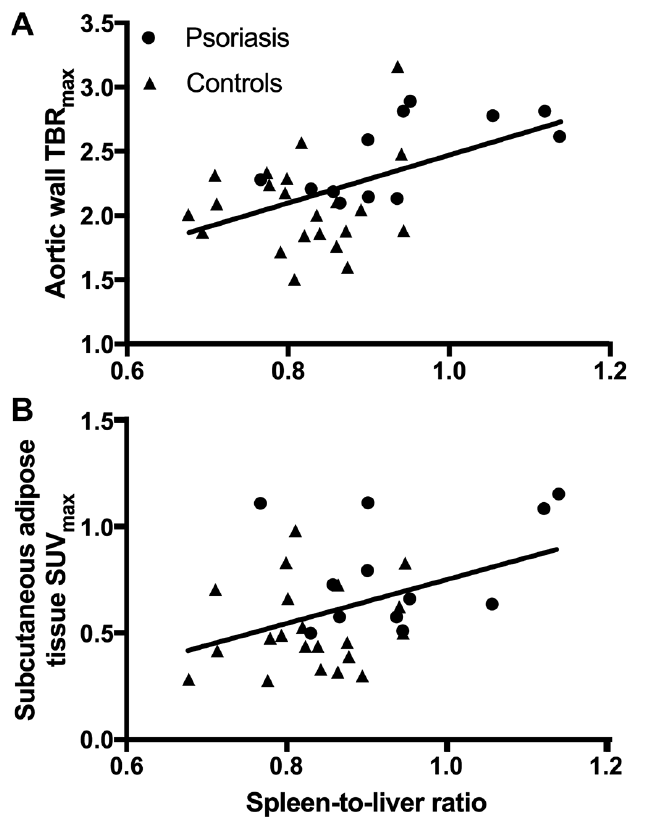 Click to show fullsize
Click to show fullsize