


1Department of Dermatology, Medical University of Graz, Austria, and 2Dermatology Unit, Galliera Hospital, Genova, Italy
Treatment recommendations for pityriasis rubra pilaris (PRP) are based solely on case reports and small case series, as to-date no randomized controlled trials are available. We present here a case series of 3 patients and a literature review of 28 studies treating a total of 116 patients, with the aim of providing data regarding efficacy and safety of methotrexate in the treatment of PRP. Methotrexate was effective in our patients; the review showed an overall response rate of 65.5% with complete clearing in 23.3% and excellent improvement in 17.2%, respectively. After excluding studies with other concurrent systemic therapies or low reliability, the overall response rate increased to 90.9%, with complete clearing in 40.9% and excellent improvement in 31.8%, respectively. Sixteen adverse reactions, of which 11 were mild, were observed in 15 patients (12.9%). In conclusion, the available literature supports good response rates and safety of methotrexate in PRP.
Key words: pityriasis rubra pilaris; methotrexate; treatment; response; review.
Accepted Jan 15, 2018; Epub ahead of print Jan 16, 2018
Acta Derm Venereol 2018; 98: XX–XX.
Corr: Cesare Massone, Dermatology Unit–Ospedali Galliera, Via Volta 6, IT-16128, Genova, Italy. E-mail: cesare.massone@galliera.it
Treatment recommendations for pityriasis rubra pilaris (PRP) are based solely on case reports or small case series, as to-date no randomized controlled trials assessing different treatment efficacies are available. We report here our experience with methotrexate (MTX) in the treatment of PRP and provide a systematic review of the literature regarding the efficacy and tolerability of treatment with MTX.
A 55-year-old man consulted our outpatient clinic in August 2014 with a 2-month history of skin changes, which had started on the scalp and spread consecutively to his shoulders and trunk. Prior treatment with systemic corticosteroids had not improved the disease. Apart from an umbilical hernia the patient was otherwise healthy and did not take any medication regularly.
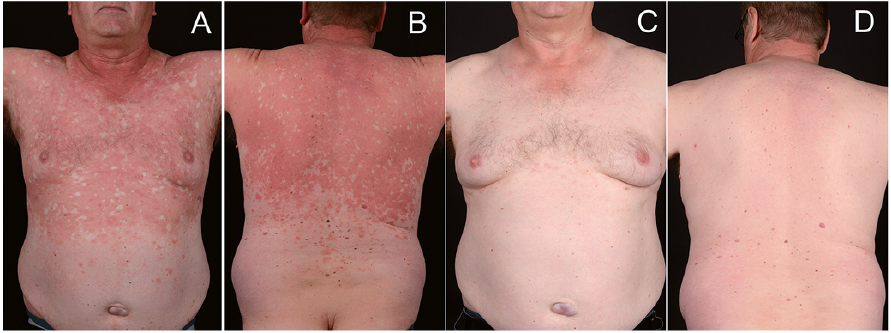
Skin examination revealed scaling erythematous to orange confluent plaques with islands of unaffected skin on his trunk, buttocks, neck, face and scalp (Fig. 1A, B). Furthermore, the patient had palmoplantar keratoderma with fissures; the affected body surface area (BSA) was approximately 50%. Histopathological examination of a skin biopsy was compatible with a clinical diagnosis of PRP and after unremarkable pre-treatment screening (Table SI), MTX treatment was initiated, 20 mg subcutaneously once weekly, followed by 5 mg oral folic acid substitution every following day.
Fig. 1. Pityriasis rubra pilaris. Case 1: skin condition (A, B) before and (C, D) after treatment with methotrexate (MTX).
At 1-month follow-up there was considerable improvement in the erythema on the trunk, but scaling and erythema on the arms and palmar keratoderma persisted. The dosage of MTX was increased to 25 mg once weekly.
At 4-month follow-up the patient showed further improvement on the trunk, but only little improvement of palmoplantar keratoderma, which later completely disappeared after 9 months of MTX treatment, when only a few erythematous non-scaling patches persisted on the trunk. MTX was then consecutively reduced each month, down to 7.5 mg/week in February 2016, when the skin had almost completely cleared. MTX was ceased in June 2016: the total MTX dosage applied was 817.5 mg, with no adverse drug reactions during the whole treatment period. A 26-month follow-up in October 2016 revealed an almost complete remission of PRP with minimal non-scaling tender plaques on the ventral trunk affecting less than 1% of the BSA (Fig. 1C, D).
A 50-year-old man with no comorbidities or long-term medication had developed facial erythema with scaling in June 2015, which then had spread to the trunk and arms after 2 weeks. He was hospitalized in our inpatient clinic in July, with a diffuse-scaling erythema covering approximately 50% of the BSA with multiple islands of sparing. The palms showed orange-red discoloration with mild keratoderma. A skin biopsy was compatible with the diagnosis of PRP and after unremarkable pre-treatment screening MTX was initiated, 10 mg/week subcutaneously, followed by 5 mg oral folic acid every following day. The MTX dose was increased by 2.5 mg/week up to 20 mg weekly with regular unremarkable laboratory controls.
At 6-week follow-up the skin worsened showing erythroderma and MTX was increased to 25 mg/week. Three weeks later erythema started to improve and an extensive scaling appeared. The erythema slowly, but progressively, reduced with a marked improvement 4 months after therapy initiation. MTX was continued at 25 mg/week until April 2016. With a total dose of 732.5 mg and less than 5% of BSA affected, weekly MTX doses were then reduced by 2.5 mg each month to a maintaining dose of 12.5 mg/week and a sustained response with < 5% BSA involved. At the last follow-up, in October 2016, the patient had a total MTX dose of 1237.5 mg with stable disease.
Apart from an intermittent elevation of liver function tests in April 2016 (GOT 70 U/l (normal ≤ 35), GPT 149 U/l (normal ≤ 45) and GGT 56 U/l normal ≤ 55)), which lowered significantly after dose reduction the patient did not have any laboratory or clinical side-effects during treatment.
An 83-year-old man had developed erythroderma in January 2014. With the initial diagnosis of psoriasis he received 311 nm ultraviolet B (UVB) phototherapy and adalimumab for one month in an external outpatient clinic with worsening of the disease. Besides untreated hypercholesterolemia and atrial fibrillation he did not have any further comorbidity.
The patient attended our department in February 2014 showing erythroderma with islands of sparing, palmoplantar hyperkeratosis with fissures and onychodystrophy. A punch biopsy revealed psoriasiform dermatitis compatible with PRP (previous treatment has probably influenced the morphological features). Acitretin, 30 mg/day, was started and increased up to 50 mg/day within 2 months with only minimal skin improvement. In July 2014 erythroderma worsened and acitretin was switched to MTX 10 mg/week, subcutaneously, followed by 5 mg oral folic acid the every following day.
At 2-month follow-up the skin already improved and MTX was increased to 12.5 mg/week. Remarkably, at 3-month follow-up only individual plaques remained on the trunk and both arms. Therapy was maintained, but the dose was not increased further due to good therapy response on low doses and a heterozygous C677T mutation of the MTHFR gene, as well as an intermittent slight elevation of GGT (81 U/l, normal ≤ 55 U/l) with GOT and GPT always within normal ranges. Transient elastography of the liver did not show any signs of liver parenchyma impairment.
At 6-month follow-up, with a total dose of 392.5 mg MTX, remission was sustained with less than 1% BSA involved. Unfortunately, follow-up was lost thereafter due to a severe trauma with intracranial bleeding and persistent brain damage. MTX and skin condition were not mentioned in the subsequent medical reports (MTX was probably discontinued at the time of trauma) and the patient died several months later at the age of 85 years due to nosocomial pneumonia.
A systematic search of MEDLINE was conducted for case reports and case series published from 1964 until August 2017 using the key words “pityriasis rubra pilaris”, “methotrexate” and “treatment”. Studies treating patients of any age and any type of PRP were included. Studies without a clear statement regarding MTX treat-ment response were excluded. Reports combining MTX with other systemic drugs, such as retinoids, were included. Together with our case series a total of 28 publications treating 116 patients were included.
Methotrexate treatment efficacy was divided into 6 effect groups: “total clearance” (for complete clearance), “excellent improvement” (“almost” or “95%” clear as well as “dramatic”, “excellent”, “favourable”, “significant”, “marked” or “considerable” improvement, respectively), “partial improvement” (“partial improvement”, “improved” as well as “partial”, “good” or “satisfactory” effects, respectively), “slight improvement” (“slight”, “sluggish” or “mixed” response, respectively), “any improvement” (“improvement” without information regarding the extent of improvement) and “no improvement”.
Reliability of case reports and studies was categorized into “high” if data on both, MTX dosage and treatment duration were available or “low” if data on MTX dosage or therapy duration were missing.
Table SII presents the clinical data, MTX dosage, treat-ment efficacy, adverse drug reactions and reliability of the reviewed studies, separated into positive and negative reports, as well as studies with other concurrent systemic therapies. MTX treatment efficacy is summarized in Table I, separated into overall response and studies with MTX single treatment and high reliability.
Table I. Methotrexate (MTX) treatment response according to the literature review
MTX is a potent folate analogue that interferes with nucleic acid synthesis and cellular proliferation due to inhibition of dihydrofolate reductase. While the exact mechanism of action in inflammatory skin conditions, such as psoriasis or PRP, remain unclear, it presumably depends mainly on 2 different effects. On the one hand, MTX acts as an antiproliferative agent, as it depresses the mitotic rate of keratinocytes via induction of apoptosis of proliferating keratinocytes through oxidative stress (1). This could explain why PRP responds to MTX in a much slower manner than psoriasis does (2), because although it has been shown that the epidermal turnover time in PRP is higher than in normal skin, it is considerably slower than in psoriasis (3). On the other hand, MTX has anti-inflammatory effects, especially via reduction of proinflammatory cytokines such as interleukin 1 (IL1) and tumour necrosis factor alpha (TNFα) (4, 5). Furthermore, as shown for rheumatoid arthritis, an increased gene expression of the anti-inflammatory Th2 cytokines IL4 and IL10, a decreased gene expression of the proinflammatory Th1 cytokines IL2 and interferon gamma (IFNγ), or the induction of apoptosis in cells involved in the immune/inflammatory reaction could play a therapeutic role (4).
Treatment efficacies are difficult to assess in PRP due to potential spontaneous clearing in up to 80% of cases after 3 years reported by some authors (6). Thus, some of the therapeutic successes reported could be related to spontaneous clearing rather than MTX treatment. Nevertheless, the use of MTX in PRP is strongly supported by the remarkable chronical correlation between MTX initiation or MTX reinstitution after therapy discontinuation and disease improvement observed in numerous studies (2, 7–12). MTX was effective in our 3 patients with PRP, inducing almost complete remission in all patients, and it was well tolerated with no major adverse drug reactions.
Combining our data with the available literature, an overall response rate after MTX therapy could be observed in 65.5% of patients, with complete clearance or excellent improvement in 23.3% and 17.2%, respectively. Furthermore, after exclusion of publications with other concomitant systemic therapy or low reliability, the overall response rate increased considerably, to 90.9%, with a complete clearance or excellent improvement in 40.9% and 31.8%, respectively. This remarkable difference can mainly be explained by a dropout of the 2 largest negative studies after excluding studies with low reliability. Significant therapy response could be observed after 3–12 weeks in several studies (2, 7–12). However, the majority of patients required therapy for several months (8, 12–21). In fact, in most cases MTX needs several weeks to become effective. MTX is a prodrug, which to become active needs a polyglutamation process, therefore it takes as long as 27.5 weeks to reach a steady state (22). Moreover, differences in absorption after oral vs. subcutaneous administration may explain why some patients respond better than others.
In contrast to these positive data, one publication mentioned that only 17 out of 44 patients showed any response to MTX treatment (6). In addition, another study treating 5 patients (23), as well as several case reports did not observe any benefits of MTX treatment (24–29). Unfortunately some of these reports, in particular the 2 larger studies (6, 23), did not mention any MTX doses or treatment durations, hence they had to be classified in the low-reliability group. The reason for MTX failure in the other studies (24–29) could mainly be explained by the relatively short treatment periods of 2 weeks (24), 6 weeks (25), 1–2 months (26) and 3 months (27).
The majority of the patients investigated had adult-onset PRP; only 14 patients were children or had childhood-onset disease. Although, with overall response rates of 57.1%, the benefit of MTX treatment was lower in childhood-onset compared with adult-onset disease, MTX was also effective in at least every second patient with childhood-onset.
Ectropion is a characteristic and common finding in PRP. Interestingly, a case report by Durairaj & Horsley (14) observed dramatic resolution of a cicatricial ectropion after treatment with low-dose MTX.
There is insufficient data available to recommend whether MTX should be prescribed orally or parenterally for treatment of PRP. Some authors showed an advantage of oral compared with parental drug administration in 2 patients (7). However, others reported a case in which 25 mg orally once weekly for 6 months did not lead to any improvement, but after 3 injections of 50 mg/week intravenously, the skin was 95% clear (12). A study treat-ing patients with rheumatoid arthritis suggests greater efficacy with equal tolerability of subcutaneous MTX compared with oral application (30). This increase in efficacy could be explained by a plateau effect of systemic drug exposure after oral application of ≥15 mg MTX, which was not observed in subcutaneous administration (31). Although we cannot transfer these findings to PRP patients with certainty, we prefer to administer MTX subcutaneously once weekly due to this mentioned plateau effect and further disadvantages of oral application, such as potentially increased gastrointestinal adverse reactions, varying drug levels because of fluctuating or insufficient gastrointestinal resorption of MTX, or a potentially erroneous daily instead of weekly oral dosing.
Concerning MTX doses recommended in PRP, there is no official statement available, as the use is still off-label. Although individual publications had used doses of up to 70 mg/week, most of the studies had administered doses between 15 and 25 mg. Reports with doses higher than 25 mg/week did not show any trend to a better outcome, but the risk of side-effects theoretically increases with higher doses. Combining the available data we recommend doses from 15 to 25 mg per week, similar to the dose for use in psoriasis (32), with individual dose adaption for every patient. After clinical improvement, the dose should be tapered to the lowest effective dose for maintenance therapy and then, as soon as the disease allows, gradually tapered off and ceased.
Sixteen adverse drug reactions could be observed in 15 out of 116 patients (12.9% of the study population) (2, 7–10, 12, 15, 19, 20, 26). The majority (n = 11) were mild side-effects including leucopaenia (n = 6), elevated liver function parameters (n = 3) and oral ulcers (n = 2), one of the latter 2 patients also had gastrointestinal side-effects. All of these adverse drug reactions resolved completely after short-term discontinuation of therapy, and although relapse of the disease occurred in some patients when MTX was temporarily suspended, reinstitution of the drug usually resulted in rapid clinical improvement (2, 7, 10, 12). Nevertheless, in 5 patients (4.3% of the study population) MTX therapy was withdrawn completely due to more severe adverse drug reactions, including one case of pneumocystis carinii pneumonia, 2 reports of severe upper gastrointestinal symptoms and 2 reports of gastrointestinal intolerance (9, 19, 20, 26). Three patients died due to diseases unrelated to PRP or therapy. To minimize adverse drug reactions, regular clinical and laboratory controls during MTX treatment are mandatory, as published previously (32). Our approach is listed in Table SI1.
Regarding therapy alternatives, oral retinoids often serve as first-line therapy in PRP. Treatment is usually well tolerated and therapy response is satisfactory, with improvement in up to 76.2% or 96% of patients (13, 33). However, in the latter study only 6 out of 45 patients experienced complete or near complete remission post-treatment (34). Furthermore, in our study population, 15 out of 116 patients had unsuccessful retinoid pre-treatment. For severe and difficult to treat PRP a combination of MTX and retinoids could be an option, although it has to be stated, that according to the Food and Drug Administration (FDA) approved prescribing information, e.g. for acitretin, this combination therapy is contraindicated. The reason is an increased hepatotoxic risk, which resulted in a case of toxic hepatitis in a patient with psoriasis (35). However, a review addressing this issue concluded that the evidence is not strong enough to support a general contraindication regarding the concomitant use of methotrexate and retinoids (36), although consequent laboratory monitoring is mandatory. Out of 116 patients included in this review, 14 patients in 3 studies had concomitant MTX and retinoid therapy with overall response rates of 85.7%, complete clearance in 50% and excellent improvement in 35.7%, with no hepatotoxic adverse drug reactions mentioned (20, 37, 38).
Another treatment option for therapy-resistant PRP is the use of biologicals such as TNFα antagonists, ustekinumab or secukinumab as well as the use of the phosphodiesterase 4 inhibitor apremilast, with promising results published recently (18, 29, 30, 39–44). Nevertheless, at present these drugs remain second-line in most countries due to availability and costs.
This study had a number of major limitations. Potential publication bias due to lower publication rates of negative results and the above-mentioned potential spontaneous clearing of the disease could have led to an overestimation of response rates. In addition, although patients requiring combination therapy, who probably experience the most severe forms of PRP, were included, some cases could have been omitted because MTX treatment effects were not mentioned in all studies with multiple therapies. Furthermore, there is a possibility that we have missed publications that are not listed in MEDLINE or did not meet our search criteria.
In conclusion, the available literature confirms positive response rates and good tolerability of MTX in the treatment of PRP. Therefore, MTX might be considered as a first-line treatment option for PRP, considering also the cost of biological therapies.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize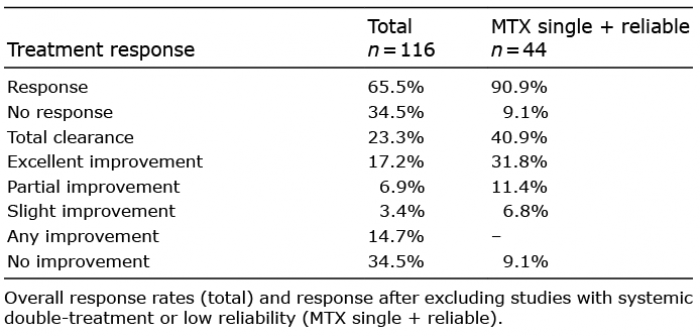 Click to show fullsize
Click to show fullsize