


1Department of Psychiatry and Psychosomatics, I.M. Sechenov First Moscow State Medical University, 2Department of Boundary and Psychosomatic Disorders, Mental Health Research Center, Moscow, Russia, 3Betsi Cadwaladr University Health Board North Wales, Centre for Mental Health and Society Bangor University, UK, 4Mysore Medical College and Research Institute, Mysore, India, 5Department of Dermatology, Barts Health NHS Trust, Royal London Hospital, UK, 6Department of Psychiatry, General Hospital Bruneck, South Tyrol, Italy, 7Department of Psychiatry and Psychotherapy III, University of Ulm, Germany, 8Department of Clinical Dermatovenerology and Cosmetology, Moscow Scientific and Practical Center for Dermatovenerology and Cosmetology, Moscow, Russia, 9Tropical Medicine, Liverpool School of Tropical Medicine, UK, 10GGnet Community Mental Health Centre, Warnsveld, and 11Dutch Information Centre for Coercive Measures, Stichting Benchmark GGZ, Bilthoven, The Netherlands
We examined the association between the duration of untreated psychosis and outcome for patients with delusional infestation. This multi-centre international study included 211 consecutive patients. Illness severity was evaluated at first presentation and outcome was measured with the Clinical Global Impression scale (CGI) at baseline and follow-up. A regression analysis showed a clear clinical and statistically significant association between shorter duration of untreated psychosis and better outcome at follow-up. Patients with a duration of untreated psychosis of less than one year showed a CGI-S change from 5.37 to 2.07; those with a duration of untreated psychosis of 1–5 years a change from 5.48 to 2.59, and those with a duration of untreated psychosis of > 5 years a change from 5.59 to 3.37. This difference of 1.1 CGI points between the groups resembles a clinically relevant difference in patient outcome. Our results suggest that longer duration of untreated psychosis in patients with delusional infestation is associated with significantly less favour-able clinical outcomes.
Key words: delusional infestation; duration of untreated psychosis; early intervention; outcome; clinical relevance; liaison psychiatry.
Accepted Jan 23, 2018; Epub ahead of print Jan 24, 2018
Acta Derm Venereol
Corr: Dmitry V. Romanov, Professor, Department of Psychiatry and Psychosomatics, I.M. Sechenov First Moscow State Medical University, and Mental Health Research Center, 127566 1-5-79 Vysokovoltny proezd, Moscow, Russia. E-mail: newt777@mail.ru, dm.v.romanov@mail.ru
Delusional infestation is a psychiatric disorder in which patients have the belief that they are infested with parasites or other living on non-living things undetectable by objective examination. Duration of untreated psychosis is the time that passes from manifestation of the first psychotic symptom to initiation of adequate antipsychotic drug treatment. It has been proven to be an important clinical outcome measure in schizophrenia and other psychoses but no studies exist for delusional infestation. We performed the first international multicentre study and showed a clear association between shorter duration of untreated psychosis and better outcome in delusional infestation. Our results suggest that earlier intervention is a desirable option in delusional infestation, leading to better outcomes.
Delusional infestation (DI) is a psychiatric disorder in which patients have the delusional belief that they are infested with parasites or other living creatures (worms, fungi etc.), or inanimate pathogens such as fibres, threads or particles (1). DI is a psychotic disorder distinctly different from schizophrenia, schizoaffective and brief psychotic disorders. It is categorized as a delusional disorder, somatic type (297.1 in DSM-5; F22 in ICD-10). DI patients fail to fulfill criteria for schizophrenia, as they do not normally show disorganised speech, disorganised or catatonic behaviour, and negative symptoms such as blunting of affect, poverty of speech and thought, reduced social drive, loss of motivation, lack of social interest, and inattention to social or cognitive input. Hallucinations in DI, if present, are not prominent and related to the delusional theme of the infestation. Apart from the impact of the delusion(s) or its ramifications, functioning is not markedly impaired.
The prevalence of DI is estimated between 5.58 and 83.23 cases per 1 million inhabitants (2, 3). Because patients with DI do not believe that they have a psychiatric illness, they usually seek referral to dermatologists or other specialists. Patients may also contact pest control businesses in order to detect and eradicate the perceived pathogen (1). Patients’ search for an identifiable infestation leads them to visit multiple physicians (1). As a result long duration of untreated psychosis (DUP) may be a common problem in patients with DI.
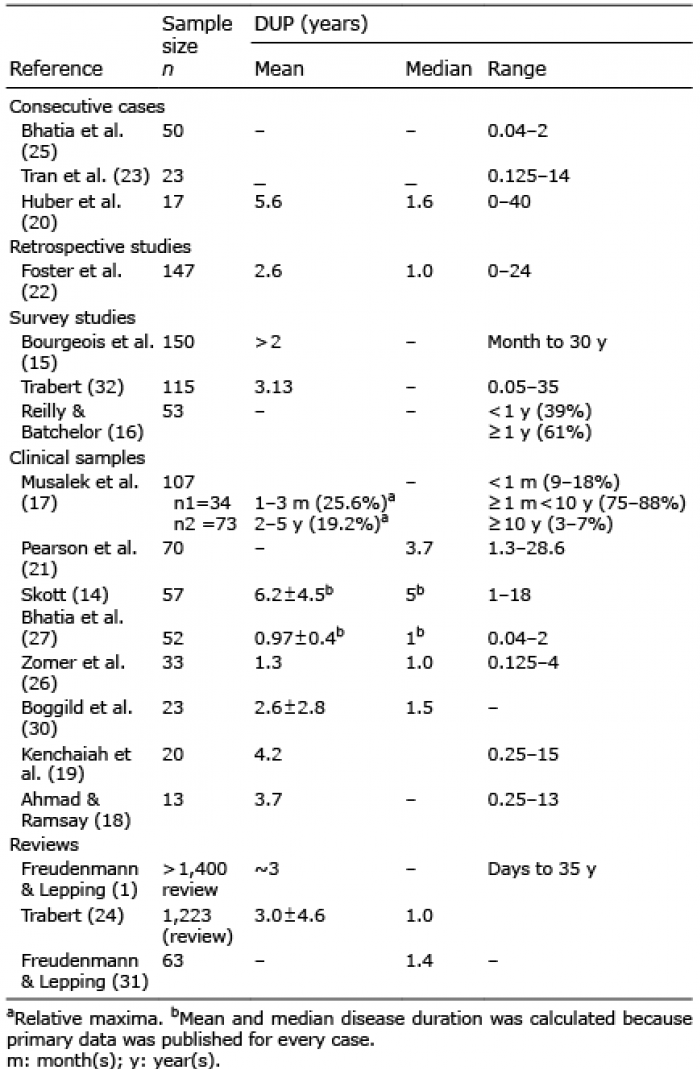
DUP is defined as the time that passes from manifestation of the first psychotic symptom to initiation of adequate evidence-based antipsychotic drug treatment (4, 5). Defining the precise onset of psychosis can sometimes remain approximate as it may depend on patient recall. Nevertheless, generally, the measurement of DUP has proven to have good to excellent inter-rater reliability, as pointed out by Rubio & Correll (6). In their review they found that although heterogeneous definitions of DUP can complicate comparing DUP across studies, measurements of DUP are reliable within the same study (6). Furthermore, DI patients usually have a good memory for the time of perceived symptom onset because of the impairment of quality of life the symptoms normally cause. There is evidence of an association between long DUP and adverse clinical outcome in patients with schizophrenia (7–10). To date, DUP and clinical outcome for patients with DI has not been systematically investigated. Available literature data on disease duration in DI are summarized in Table I. In publications disease/symptoms duration is equivalent to DUP, as patients are introduced to treatment with antipsychotics typically not earlier than from the moment of correct diagnosis.
Table I. Available studies on duration of untreated psychosis (DUP) for delusional infestation (DI)
Data on DI symptoms duration report disease durations varying from days to decades (11–23) (see Table I). It has been noted that the duration distribution followed an exponential function with 52% of all cases showing a DUP of one year or less (24, 25). Focusing exclusively on publications from the last 30 years, mean psychosis duration before receiving adequate treatment in DI varies from 0.97 to 5.6 years (see Table I) (1, 18–20, 22, 26–30). Only two studies provide mean duration values in a “M ± SD” format (23, 30). The variance of median psychosis duration is less prominent. It ranges from 1 to 3.7 years (20, 21, 29–31), but the most frequently provided median duration is 1.0 year (22, 24, 26, 27).
Some of the studies mentioned above include data on DI outcome. In these studies adherence to treatment was assumed but not verified, and DI patients are unlikely to have had a high adherence rate (32, 33).
There are some suggestions that a short preclinical course in DI may indicate better outcome (24). However, the only study showing that shorter duration of DI was related to improved outcome had a rather small sample size (23 subjects) (29). Boggild et al. (30) showed that patients with full recovery of symptoms described as mild had a shorter DUP than patients with an incomplete or absent remission.
The aim of the current international multicentre study was to verify mean duration of untreated psychosis in patients with DI. Our hypothesis is that longer duration of untreated psychosis is associated with poorer outcome as assessed by change in clinical presentation during treatment.
Our consecutive cohort study comprises 211 cases of DI seen in multidisciplinary outpatient clinics in England (London: 89 patients, Liverpool: 32), Italy (Bruneck: 26) and Russia (Moscow: 64) over a period of 10 years (2006–2015). The included clinics are specialized in the treatment of DI. These clinics receive referrals from a wide range of sources and cover large geographical areas. All clinics consist of a psychiatrist and a physician, either a dermatologist or a specialist in tropical medicine. In setting up our study, all patients underwent a similar clinical approach including the staffing of the clinics, follow up intervals according to clinical need, and the use of second generation antipsychotic medication as first line treatment. We excluded centres which were not able to demonstrate clinical uniformity. Standard clinical psychiatric and dermatological assessments were carried out for all patients to establish a diagnosis of DI. There were no patients identified with a genuine infestation. Once the diagnosis of DI was established, all patients were offered antipsychotics as treatment. In addition, they were offered appropriate treatment for any secondary skin condition or other secondary illness that may have triggered their DI. All patients were followed up rigorously as much as possible. Data on age and sex at presentation, DUP, and disease severity (CGI severity score at baseline and CGI severity score at last follow-up) (34) were obtained. DUP was defined as the time from manifestation of the first psychotic symptom to initiation of evidence-based adequate antipsychotic treatment (35).
The severity of the DI was measured with the Clinical Global Impression Severity Subscale (CGI-S), a well-validated physician assessed scoring tool used frequently in psychiatry which grades symptom severity from 1 to 7: 1 “normal, not at all ill”; 2: “borderline mentally ill”; 3: “mildly ill”; 4: “moderately ill”; 5: “markedly ill”; 6: “severely ill”; and 7: “among the most extremely ill patients” (34). CGI-S was assessed at baseline and last follow-up.
Simple demographic frequencies are presented to identify the general characteristics of the population. To understand possible selection bias, we compared completers and dropouts with regards to those characteristics. We then investigated the change between CGI-S at baseline and follow up by means of a paired sampled t-test. In addition, an analysis of variance (ANOVA) was performed. Since we expected DUP to be positively skewed (24), we first categorized DUP in 3 groups in line with the literature (35, 36); those below and above one year and the outliers with a DUP of above 5 years. In accordance with the literature these groups have clinical relevance: we may expect treatment compliance to be better in the first as opposed to the last group (36). The ANOVA was performed to investigate group differences of CGI-change between these 3 clinically relevant groups.
Following this, we performed a linear regression to investigate if one of the background characteristics other than duration of untreated psychosis were related to the treatment response as measured by change in the CGI. We first performed a Pearson and, where necessary, Spearman correlation to understand the direct association between the predictors age, sex, country and DUP and CGI change. We then included these variables in a multivariable (37, 38) regression, using the relevance criterion of Braun & Oswald (39). A stepwise, forward entry, backward deselection linear regression procedure was used to identify variables also associated with CGI-S change. To adjust for DUP skewedness, we repeated the analysis, using log transformed DUP as predictor, in order to improve the understanding of the effect of the variable “DUP” on outcome (38). This careful procedure provides an impression of the contribution of possible confounders in the final model.
The consecutive sample consisted of 211 patients (65% females (n = 138)) (Table II). In this sample the mean age was 58.8 years (range 18–95). The mean ± standard deviation duration of untreated psychosis (DUP) was 3.4 ± 4.2 years), with a minimum of 2.5 months and a maximum of 29 years. The median was 2.0, with a positive skew value of 2.8, implying a number of outliers at the longest number of years of DUP. Thirty-seven patients did not engage with treatment or were lost to follow-up, one patient died from an unrelated illness. The majority of patients (n = 173, 82.0%) accepted treatment and confirmed relatively higher adherence to treatment matching previously published data from multidisciplinary psycho-dermatology clinics (32). Age, sex distribution, CGI-S at baseline and DUP in the patients refusing treatment did not differ from those accepting treatment. Of the 173 patients included in the comparative analyses, 74 were from London, 57 from Moscow, 24 from Bruneck, and 18 from Liverpool. Treatment dropout differed significantly between countries, with the largest dropout seen in UK, and the lowest in Italy. Fig. 1 shows the distribution of DUP for all included patients.
Table II. Baseline data and description of the population
Fig. 1. Distribution of duration of untreated psychosis (DUP) in years.
Table III shows the main result with the numbers of patients per DUP category and parametric analysis of variance comparing CGI-S scores at baseline and follow-up. This shows a clear and positive association between longer DUP and poorer outcome. Patients with a DUP more than one year, and more importantly in the outliers, mean scores and mean ranks are substantially and significantly higher. When looking at the DUP changes in those 3 groups with an ANOVA, patients with a DUP of less than one year showed a CGI change of 3.30 on the 7-point CGI-S scale (CGI-S change from 5.37 to 2.07). Those with a DUP of 1–5 years showed a CGI-S change of 2.89 points (5.48 to 2.59), while those with a DUP of > 5 years showed a change of 2.22 CGI-S points (5.59 to 3.37). There was no statistical difference between the 3 groups with regards to the CGI-S scores at baseline (p = 0.610). However, the difference between the groups was significant at follow-up (p = 0.010), as was the significance of the difference of the change in CGI-S scores (p = 0.037).
Table III. Numbers of patients per duration of untreated psychosis (DUP) category and analysis of variance (baseline, follow-up and change of Clinical Global Impression Severity Subscale (CGI-S))a
Our analysis of CGI-S score changes from baseline to last follow-up revealed a marked improvement in symptoms (mean change from 5.46 to 2.64; see Table II). Whereas before treatment most patients were on average ‘markedly ill’, with treatment the median score was ‘borderline ill’. A paired sample t-test between CGI-S scores at baseline and at follow-up showed a statistically significant difference (mean difference = –2.87; t-value=22.37, p < 0.001; see Table II). Importantly, the median reduction was 3 points in CGI-S severity, which is highly clinically relevant.
In Fig. 2 the relationship between DUP (in years) and CGI-S change is shown. Fig. 2 shows a downward slope of DUP the larger the CGI-change. This means that in general there was more improvement of CGI with shorter time of DUP. Furthermore, we categorized the patients into 3 clinically important groups according to the CGI severity at follow-up: (i) patients not at all ill (n = 62; 35%, CGI-S: 1), (ii) patients borderline or mildly ill (n = 70; 40%, CGI-S: 2–3) and (iii) patients moderately ill or above (n = 41, 25%, CGI-S: 4–7). Between these 3 groups, the mean DUP differed significantly, 2.18 in the ‘not at all ill’ group (group 1), 3.9 in the ‘borderline or mildly ill’ group (group 2) and of 4.22 in the ‘moderately ill’ or above group (group 3) (f-value=3.83, p = 0.024).
Fig. 2. Relationship between duration of untreated psychosis (DUP) (in months) and Clinical Global Impression Severity Subscale (CGI-S) score change (we only present the mean DUP per change category).
When examining the change in severity from baseline, we identified 3 clinically important groups: (i) those much improved with a CGI-S score difference of more than four points, (ii) those somewhat improved (CGI-S score difference of 1–3 points), (iii) those with unchanged CGI-S scores or worsened CGI-S scores (change of 0 to –1 CGI-S points). Between these groups, the mean DUP differed significantly, with a mean DUP of 2.54 in the much improved, of 3.66 in the somewhat improved, and of 5.10 in the unchanged or worsened group (f-value=3.24, p = 0.041).
A regression analysis was performed in a number of steps (Tables IV and V). To identify relevant predictors, we first performed a Pearson and Spearman correlation (Table IV). Age was left out of the regression, as it showed a correlation of 0.011 to CGI-S change. In the regression analysis (Table V), DUP proved to be a significant predictor after correction for country as a confounder. The final model showed that sex was not related to changes in CGI-S scores, whilst country (Beta 0.705, 95% CI 0.514–0.896; p < 0.001) and duration of untreated psychosis (Beta 0.068, 95 CI 0.014–0.122; p = 0.014) showed an association. Using log transformed DUP as a predictor (38) showed that country (Beta 0.356, 95 CI 0.405–0.927; p < 0.001) and duration of untreated psychosis (Beta 0.208, 95 CI 0.108–0.546; p = 0.004) had comparable associations. The adjusted R-square (as indicator of model effect) was 0.136 (ESDup = 0,157), and 0.146 (ESLog Dup = 0.172) in these final models, which is reasonable, given the number of predictors and the sample size. Stratification of the analyses by country improved the explained variance to 0.186 and 0.312. Co-linearity diagnostics performed beforehand showed no underlying associations of variables. DUP was not confounded by country (Table II).
Table IV. Correlation of Clinical Global Impression Severity Subscale (CGI-S) change with age, gender, country and duration of untreated psychosis (DUP) (n = 173 treatment completers)
Table V. Regression of CGI change corrected for sex, country and duration of untreated psychosis (DUP)a
These analyses show that in the final model a clear prediction of change in CGI-S by DUP is observed. It confirms that there is an association between longer DUP and poorer outcome as measured by change in CGI-S. For results of further analyses please contact the authors.
Our results indicate that there is a clinically relevant association between shorter DUP and increased improvement of CGI-S scores. Longer DUP was associated with significantly less symptomatic improvement (as measured by CGI-S scores). The mean DUP obtained in our study was 3.4 years and falls into the range of mean values published elsewhere (1, 18–20, 22, 26–28), including studies with large samples sizes (1, 24, 28, 29). Only small studies with small sample sizes have so far presented DUP of < 3 or > 4 years with the exception of Foster et al. (n = 147, DUP: 2.6 years) (22). In general, most previously published mean values are within the SD of our mean value. Thus, the population in our study could be considered as representative of the population of DI patients described elsewhere.
The range of disease duration shows similarities with previous studies, i.e. a minimum of 2.5 months and a maximum of 29 years in our study. This wide range of DUP is comparable to previously published data (18, 19, 22, 23).
The negative effects of a long DUP have been explored in numerous studies for a variety of psychiatric diagnoses (6, 10, 36, 40–45). They are heterogeneous but all concluded that DUP is an important modifiable indicator of prognosis. However, there are no data on DUP and its association with outcome in delusional disorders. There is a single comparative study that suggests that DUP in patients with delusional disorders does not differ significantly from DUP in patients with schizophrenia (46). Our results are consistent with the only previous small study on DUP in DI (30), showing that shorter DUP is related to improved outcome and prognosis. However, probably as a result of small sample size, the authors of that study could distinguish only two relevant follow-up groups: “full recovery/mild residual symptoms” versus “incomplete /absent remission” that differed significantly (mean ± SD 1.2 ± 0.8 vs. 3.0 ± 1.5 years). In contrast, our results comprise more distinct strata (“much improved”, “somewhat improved”, “unchanged”, “worse”), the use of a standardized instrument for severity measurement (CGI-S) and a much bigger study sample (173 vs 23 subjects). In addition, our study is a truly consecutive, multicenter study which has followed up patients systematically from specialist multidisciplinary clinics.
Our findings have clear clinical relevance. The potential of DUP being modifiable raises the possibility of improving clinical outcomes by shortening DUP. In designing interventions to shorten DUP, it is important to identify factors contributing to DUP. Factors previously associated with a longer DUP include stigma-related concerns (47, 48), an insidious mode of onset (49, 50), and a diagnosis of non-affective psychosis compared with affective psychosis (51, 52, 53). In contrast, DUP shortening is associated with development of early interventions that reduce treatment delay and promote recovery as it has been shown in schizophrenia studies. Early intervention is followed by an improvement in the prompt treatment of people with first episode psychosis (54). It remains unclear at this point how applicable the principles of early intervention are for patients with DI. However, in keeping with general early intervention approaches of destigmatization and insight improvement in psychosis, educational and contact interventions may be potentially beneficial. Any early intervention programs for DI should be provided in partnership between mental health professionals and other physicians (“joint care”) (55), as there is evidence for Joint clinics in DI (1). There is an opportunity not only for combined assessment and treatment, but also for cross-education between representatives of different medical specialties to improve care and thus DUP. This can be provided in combined psychiatric and dermatological or psychiatric and tropical medicine clinics with specialists able to address the question how to persuade the DI patient with little or no insight to shorten the period of untreated psychosis by trying evidence-based antipsychotic treatment.
This study investigated patients from specialist settings. These settings are probably the optimal treatment venues currently available for patients with DI, as they provide combined dermatology or tropical medicine and psychiatric services (54). It is not clear whether the same association between DUP and outcome applies to patients being seen only in primary care or for patients with DI managed in general dermatology clinics without specialist psycho-dermatology expertise. However, given that even in specialist psycho-dermatology clinics, there is an association between DUP and poorer clinical outcomes, and given that there is evidence (albeit non-randomized) that care of patients with DI is optimized in specialist psycho-dermatology clinics, the association between DUP and poorer clinical outcome may be even worse in non-specialized clinics. Even in our specialist settings 18% of patients did not agree to try any medication, which is in keeping with earlier publications (31). Clearly this is not an inconsequential number. It highlights the difficulties with engagement of this challenging patient group.
Even though we had the biggest sample size of any such study to date and the model required 150 patients to yield statistically relevant results, bigger sample sizes may improve the results in future research. We therefore need to emphasize the clinical rather than the statistical relevance of the association we found. Furthermore, general demographic factors as education, having a job, or being married may increase the power of the findings, as may possible drug abuse, which was examined by our group in a separate study that included patients of this sample (56).
We have not factored in the length of follow-up in our study and different length of follow-up could potentially influence outcome. We have found a statistical association, which is of course no proof of causality. We did find a variation between countries. However, this variation was expected because of the differences in clinic settings. The Bruneck sample was responsible for much of the variance. It was by far the smallest and the only rural sample. It showed better follow-up rates, comparable baseline CGI and lower follow-up CGI than the urban samples. This effect has been well documented in the literature where treatment compliance and effect is often better in rural versus urban settings (57).
Research in DI is difficult as few randomized controlled trials exist for a variety of practical and other issues (2). Possible factors that contribute to longer DUP in DI should be studied. It will be essential to identify which barriers the groups with the shortest DUP and longest DUP had to overcome before starting treatment. This would require a qualitative research approach examining a variety of treatment approaches to identify the most successful approach in these patients. This may also include looking at characteristics of patients who refuse treatment. An interesting question for further studies may be whether early intervention (EI) models proposed for other psychoses are an adequate option for DI patients. A recent study showed that the concept of EI may be relevant in the age range of over 35-year-olds (58), more akin to the DI population. Finally, assessing the length of DUP and clinical outcomes for patients with primary compared to secondary DI would be an important next step.
This research collaboration was facilitated by most authors’ membership of ESDaP (European Society for Dermatology and Psychiatry). We would like to thank Rebecca Cannell from BCUHB for her secretarial support.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize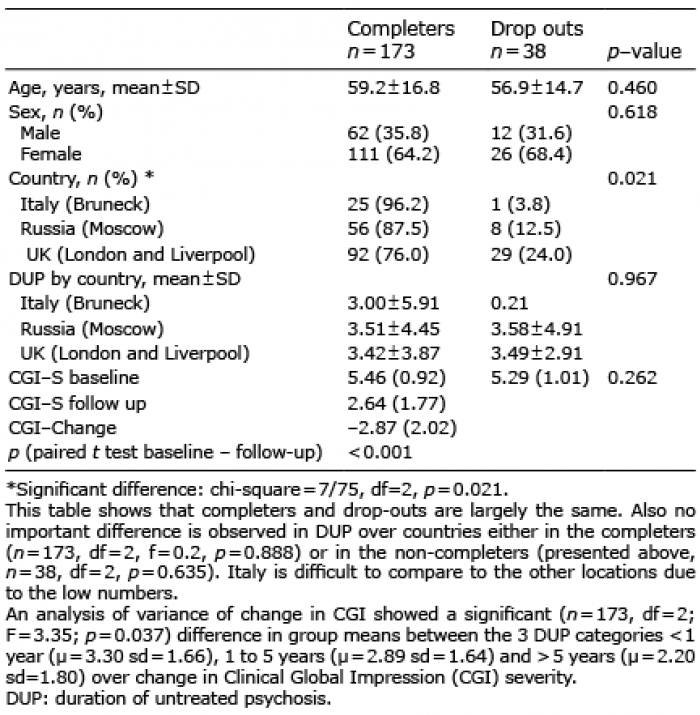 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize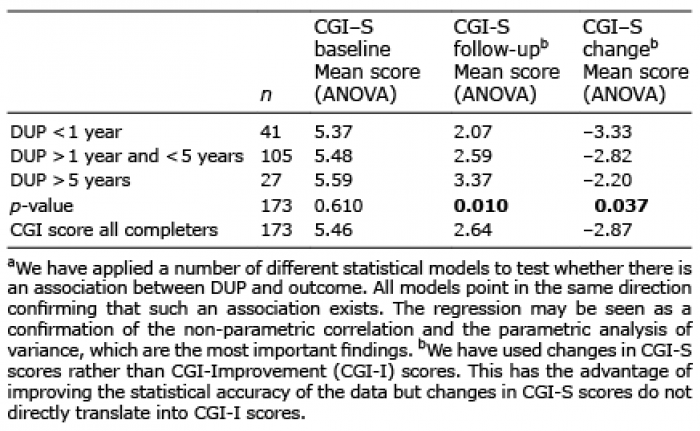 Click to show fullsize
Click to show fullsize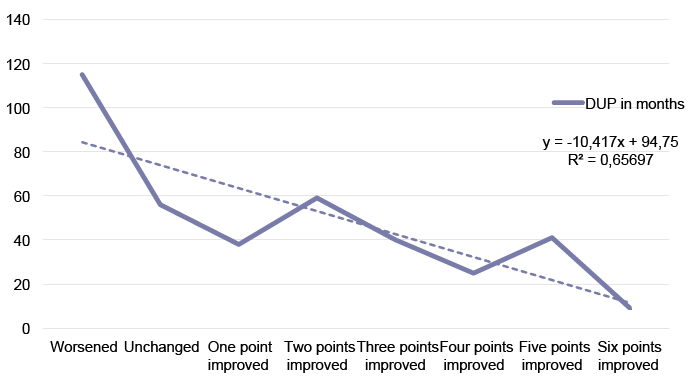 Click to show fullsize
Click to show fullsize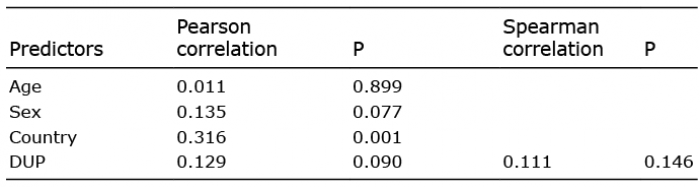 Click to show fullsize
Click to show fullsize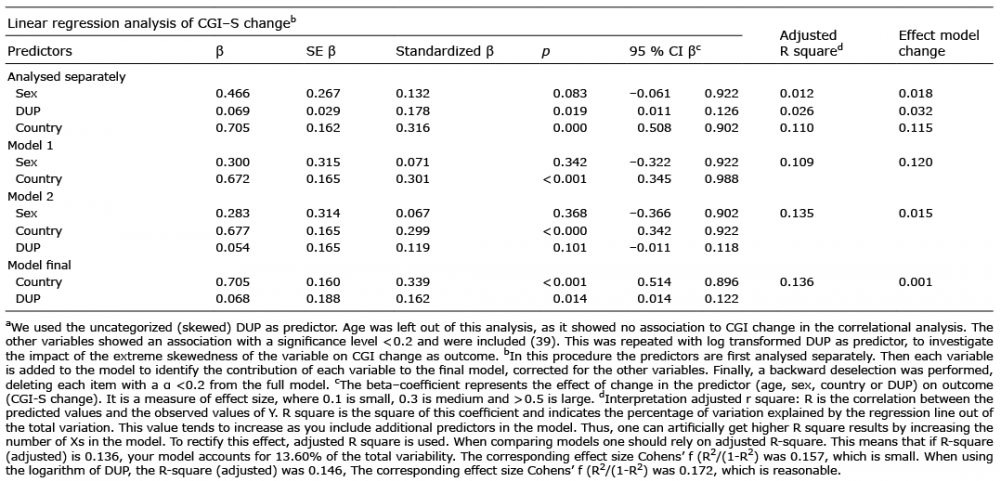 Click to show fullsize
Click to show fullsize