


1Department of Dermatology and Wound Healing, Division of Infection and Immunity, School of Medicine, College of Biomedical and Life Sciences, Cardiff University, Cardiff, 2School of Life and Medical Sciences, University of Hertfordshire, Hatfield, and 3Institute for Medicines Development, Cardiff, UK.
Accepted Jan 23, 2018; Epub ahead of print Jan 24, 2018
The minimal clinically important difference (MCID) is a widely used concept to interpret the meaning of health-related quality of life (HRQoL) score changes. However, to give a greater sense of the meaning of score change across a wider spectrum of score changes, we propose a new concept of ‘2MCID’. This represents a score change of twice the MCID. This approach, novel in dermatology, has been used in other areas (1, 2) and highlights therapies that reach this higher change thres-hold. We hypothesise that this method would better discriminate between the efficacy of interventions to help guide clinical judgement and patient progress.
HRQoL outcome measures capture several aspects of a patient’s overall well-being (3). Such measures are increasingly being implemented in interventional studies alongside clinical objective parameters as important contributors towards morbidity and mortality data (4). Reports of studies often include HRQoL data citing statistical differences pre- and post-intervention, though statistically significant changes may not be reflective of meaningful change in HRQoL, particularly within large sample sizes which may produce statistically significant change despite the change being small (5).
The MCID is the minimum difference needed for a patient to perceive the change as beneficial (6) and may be used to determine whether a medical intervention improves patient perceived outcomes. Factors to consider when calculating the MCID for a particular outcome include: patient baseline severity, particular disease or condition, patient demographics and treatment. There is no consensus on the best methodology for calculating the MCID (7), and values may therefore differ. Despite these limitations, it is still more useful for clinicians to assess intervention effectiveness based on the patient’s perspective, rather than solely on statistical significance.
The most commonly utilized quality of life (QoL) tool in psoriasis trials is the Dermatology Life Quality Index (DLQI), with an MCID of 4 points (8, 9). During this systematic review we noted that multiple MCID could provide a further aid to the results’ interpretation: we felt this novel concept deserved further exploration. We have therefore applied the 2MCID concept to data from that review (8).
A systematic review was presented by Ali et al. (8). We have introduced the concept of 2MCID to that dataset (i.e. DLQI score change of at least 8) to demonstrate comparative efficacy between interventions.
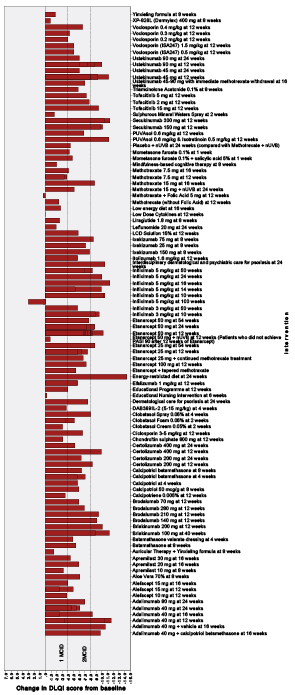
A total of 100 trials were identified by the systematic review, covering diverse interventions. As the DLQI was the most commonly used QoL measure (83% of studies), the 2MCID concept was tested on interventions with documented DLQI scores. Fig. 1 summarises all the interventions that met the different MCID thresholds.
Fig. 1. Mean Dermatology Life Quality Index (DLQI) score change in 83 clinical trials for psoriasis (8), showing those interventions that reached 1 minimal clinically important difference (MCID) and 2 MCID score change.
For topical treatments, clobetasol 0.05% spray showed the greatest improvement at 4 weeks (2MCID, 8 point improvement), followed by calcipotriol plus betamethasone at 8 weeks (6.4 points). These changes are comparable to ustekinumab 90 mg at 12 weeks (mean 2MCID (8 point) improvement) and ciclosporin 3–5 mg/kg at 12 weeks (6.6 point improvement). No other topical therapy reached 2MCID. However, it is important to consider the context of baseline psoriasis severity, treatment duration and long-term QoL maintenance.
Methotrexate 15 mg at 16 weeks was the only systemic intervention over the 2MCID threshold (8.7 points). This was comparable to several biologics, including etanercept 50 mg at 24 weeks and ustekinumab 90 mg at 12 weeks (8.7 points).
Infliximab 5 mg/kg at 16 weeks and secukinumab 300 mg at 12 weeks demonstrated the largest improvement in DLQI score of a mean of 11.4 (>2MCID), just short of 3MCID. Amongst other interventions, an energy-restricted diet with immunosuppressive therapy at 24 weeks recorded DLQI improvement of 14.4 (3MCID). DLQI at 12 weeks improved by 11.2 (>2MCID) with PUVAsol 0.6 mg/kg + isotretinoin 0.5 mg/kg: for PUVAsol alone, DLQI improvement was 6.8.
For studies with treatment endpoint and assessment at 12 weeks, the interventions with the greatest mean DLQI impact in each category were secukinumab 300 mg (2MCID, 11.4 points), ciclosporin 3–5 mg/kg (1MCID, 6.6 points), PUVAsol 0.6 mg/kg+isotretinoin 0.5 mg/kg (2MCID, 11.2 points), Liquor Carbonis Distillate solution 15% (1MCID, 5.8 points) and educational programme (1MCID, 4 points).
Previously, Leaf & Goldfarb (1) described the impact of erythropoiesis stimulating agents on HRQoL using Short-Form 36 and The Kidney Disease Questionnaire. However, the authors only infrequently arbitrarily refer to score changes using multiples of MCID without formal concept utilization. Similarly, Jones et al. (2) equate a change of ‘twice the MCID’ to a ‘large benefit’ when comparing active treatments for COPD against placebo using the St. George’s Respiratory Questionnaire. Neither study formally explored or stratified results.
Although score banding descriptors can be used (10) to describe patient numbers within score bands pre- and post-intervention, a method is needed to discriminate between the extent of the effect of interventions on QoL. The concept of ‘multiple-MCID’ could add meaning to score change when comparing therapies, or when comparing results across different QoL instruments as a ‘unit of change’. 2MCID appears to be a practical threshold providing a meaningful ‘hurdle’ that developers of new interventions might strive to achieve. In the systematic review analysis, only one data set from 83 RCTs demonstrated a change of 3MCID, indicating that a 3MCID ‘hurdle’ would be a difficult and impractical threshold.
This ‘pilot study’ of the ‘multiple-MCID’ concept demonstrates the potential benefit of comparing the extent of impact of different categories of interventions on QoL and interpreting change over time. We have demonstrated that some systemic interventions may impact QoL to the same extent as certain biologic treatments. Similarly, certain topical treatments may be as efficacious as systemic alternatives. However, the systematic review dataset is not homogenous and often patients have different baseline severities. Although MCID values are applied across a spectrum of scores in interpreting change in scores of a measure, in reality the MCID score value may be different if the score change is at the lower or upper end of a HRQoL measure score range. This criticism of the concept of MCID requires further investigation, possibly through meta-regression where the magnitude of effect on DLQI is regressed on baseline severity. The 2MCID concept may be too simplistic: ideally the identification and calculation of a multiple-MCID score should be based on prospective research based on patient assessment of a higher level of change, using an anchor question based on, say, “Major clinically important difference”.
Despite these reservations we believe ‘multiple-MCID’ provides additional meaningful information on clinical improvement and may be of value to clinicians, patients and the pharmaceutical industry. Medications that meet the ‘2MCID’ minimum threshold might be more readily approved by pharmaceutical regulatory authorities and health technology assessment agencies. This concept may also enable researchers to better distinguish between interventions and comparators in trials, potentially improving patients’ access to the most effective new medicines. Prospective longitudinal studies could aim to prove the usefulness of the concept before implementing it more widely. Further work is required before this novel concept is adopted in treatment decision-making and in reimbursement appraisals.


 Click to show fullsize
Click to show fullsize