


1Department and Clinic of Dermatology, Venereology and Allergology, and 2Department and Clinic of Hematology, Blood Neoplasms and Bone Marrow Transplantation, Wroclaw Medical University, Wroc?aw, Poland
Aquagenic pruritus is one of the main clinical features of polycythemia vera. The aim of this study was to analyse the clinical characteristics of aquagenic pruritus. The study group comprised 102 patients with molecularly confirmed polycythemia vera. Demographic data, data on disease history, polycythemia vera status and treatment modalities were collected. Moreover, various clinical features of aquagenic pruritus (including intensity, localization, quality, descriptors) and the most common factors responsible for its aggravation or alleviation were examined. Aquagenic pruritus was observed in 41.2% of individuals, mean duration 6.6 ± 8.6 years, and its onset was noticed in the majority of patients (52.4%) before the diagnosis of polycythemia vera. The mean intensity of aquagenic pruritus was 4.8 ± 1.9 points (visual analogue scale). One-third of patients with aquagenic pruritus avoided any contact with water. Antipruritic treatment was received only by 3 patients. Aquagenic pruritus seems to be an important, but frequently neglected, symptom in patients with polycythemia vera.
Key words: aquagenic pruritus; polycythemia vera; itch.
Accepted Feb 13, 2018; Epub ahead of print Feb 13, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Jacek C. Szepietowski, Department and Clinic of Dermatology, Venereology and Allergology, Wroclaw Medical University, Cha?ubi?skiego 1, PL-50-368 Wroc?aw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
The causes, effects and treatment of polycythemia vera (PV)-associated pruritus and, more specifically, aquagenic pruritus (AP) are relatively unknown. The aim of this study was to broaden our understanding of this detrimental and life-inhibiting condition.
PV is one of the main clonal, BCR-ABL-negative, haematological malignant neoplasms caused by mutations of a cytoplasmic tyrosine kinase – Janus kinase 2 enzyme (either JAK2V617F or JAK2 exon 12) (1, 2). The homozygotic mutations of JAK2 were found to be significantly more often associated with AP (3).
AP was first reported as an important clinical feature of PV in 1985 (4), although the disease was described earlier, in 1970, by Shelley (5), who distinguished it from aquagenic urticaria. AP is characterized by the development of intense itching, stinging, tingling or burning sensations without visible skin lesions and is brought on by contact with water of any temperature (4). The estimated prevalence of PV-associated pruritus varies and, according to published data, is reported in 31–69% of patients (6–8). It has significant influence on patients’ quality of life and personal hygiene, as it can lead to patients abandoning bathing completely (9).
Although AP is recognized as the most excruciating aspect of PV, knowledge of its pathophysiology, frequency and precise character is limited. Moreover, the lack of insight into the mechanism of cutaneous induction of PV-associated AP makes treatment of this condition constantly challenging. Therefore, the aim of this study was to analyse the clinical features of AP.
The material for the study was collected between April 2015 and June 2016. The study group comprised 102 patients (65 women and 37 men) with confirmed PV according to the WHO criteria. All of the patients presented with JAK2V617F mutation. The age range of studied individuals was 30–90 years (mean 66.9 ± 12.7 years).
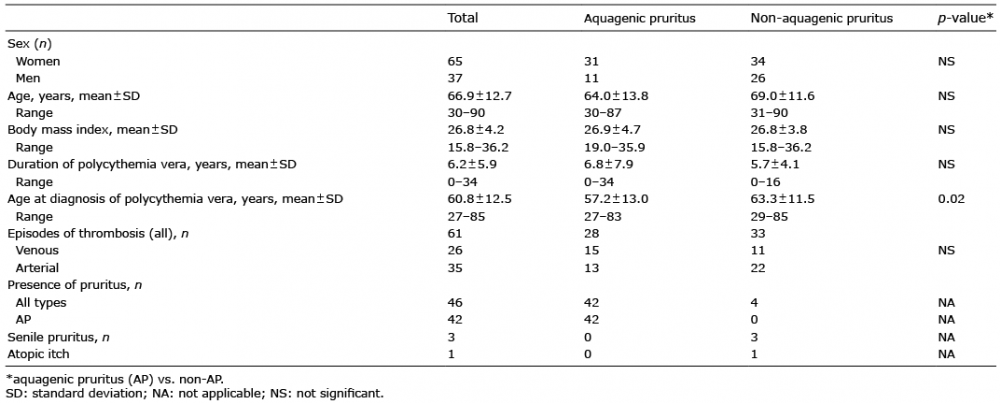
Individuals with AP constituted a group for further analysis, with a detailed examination of pruritus. Patients presenting other types of itching (4/102; 3.9%) were excluded. None of the patients reported the presence of pruritus previously or its spontaneous resolution. Detailed characteristics of the study group are given in Table I.
The study was approved by the ethics committee of Wroclaw Medical University (number 355/2016).
Table I. Characteristics of studied group
Demographic data, disease history, PV status and treatment modalities were collected from all participants. AP intensity was evaluated with a visual analogue scale (VAS), verbal rating scale (VRS) and a 4-item Itch Questionnaire (10–13).
Patients were asked to indicate on a 10-point VAS scale, the maximum and mean intensity of their pruritus during the last 3 days. Scores ranged from 0 (no itch) to 10 points (worst imaginable itch). VAS cut-off points are as follows: mild pruritus (0–< 3 points), moderate pruritus (≥ 3–7 points), severe pruritus (≥ 7–9 points), and very severe pruritus (≥ 9 points) (10).
Participants assessed their itch intensity on the VRS by selecting one of the following options: “none”, “mild”, “moderate”, “severe”, or “very severe”.
The 4-item Itch Questionnaire was used to estimate the extent (1–3 points), intensity (1–5 points), frequency (1–5 points) and sleep disturbances (0–6 points) caused by AP during the 3 days prior to the examination. Ratings ranged from 3 (mild pruritus) to 19 points (very severe pruritus). This instrument was used previously by our group to distinguish the various types of pruritus (14–16).
In addition to itch severity, various clinical features of pruritus were assessed, including its exact localization, quality and descriptors. Moreover, the onset of AP due to contact with water or changes in its temperature and other common factors, such as aggravation or alleviation of the sensation, were also examined.
All data were assessed for parametric or non-parametric distribution. Pearson’s χ2 test was applied to sets of categorical data. Differences between groups were determined using the Mann–Whitney U test and Kruskal–Wallis test, or Student’s t-test, and analysis of variance (ANOVA) with reference to the distribution of evaluated variables (abnormal or normal, respectively). Correlations were determined via Spearman’s correlation analysis. A p-value < 0.05 was considered statistically significant. Statistical analyses were performed using Statistica 12 software (StatSoft, Tulsa, OK, USA).
Pruritus was present in 45.1% (46/102) of patients with PV. In this group AP was observed in 41.2% (42/102), more commonly in women (31/42). The remaining patients had itch of another type, i.e. senile pruritus (2.9 %) or atopic itch (1%) (Table I). None of the patients reported the coexistence of AP with pruritus of another cause.
The range of duration of AP was 0–44 years (mean 6.6 ± 8.6 years). The onset of AP was noticed in the majority of patients prior to the diagnosis of PV (52.4%) and preceded it with a mean of 2.3 ± 2.9 years (range 0–10 years). More than half of the patients (52.4%) experienced AP every day, whilst the remaining patients experienced pruritus a few times per week (38.1%) or per month (9.5%).
According to VAS, the maximum intensity of AP was assessed as 5.2 ± 2.4 points (range 1.2–10 points), whereas mean VAS was 4.8 ± 1.9 points (range 2.5–8.7 points). Mild pruritus was observed in 23.8% of patients, moderate pruritus in 50% of patients, and severe or very severe pruritus in 26.2% of patients. With reference to VRS the AP was usually “moderate” or “mild” (38.1% and 28.6%, respectively), whilst “very severe” itching was experienced by 11.9%. The mean result for 4-item Itch Questionnaire in patients with AP was assessed as 6.0 ± 2.9 points (range 3–15 points) and correlated strongly with VAS and VRS (p < 0.0001, for both variables).
Contact with water provoked AP after > 5 min in 17 subjects (40.5%) and, in the remaining, within 1–5 min of contact (33.3%), or immediately (up to 1 min) (26.2%). It is worth noting that 33.3% of patients with AP avoided contact with water on an everyday basis. Moreover, the patients with higher VAS avoided contact with water significantly more often than those with lower VAS (p = 0.003). Worsening of itching was observed more frequently after contact with hot water (57.1%) than cold (1.9%). No changes in AP intensity were observed for the other aggravators/alleviators, including physical exercise, excessive sweating, stress, spicy food or a warm environment (data not shown).
The majority of patients with AP described pruritus as itching (54.7%) or burning (23.8%) sensations. Less commonly it was described as other sensations: prickling (14.3%), warming (11.9%), stinging (9.5%) or tingling (2.3%).
In the majority of patients with AP (45.2%), the pruritus was limited to a few regions of the body; most commonly to upper and lower limbs, less often to the torso. PV-associated pruritus specific to one part of the body occurred in 33.4% of patients, while whole-body pruritus was observed in 21.4%. AP requiring scratching was found in 42.8% of individuals and appeared mostly as short itch episodes with a duration of 1–10 min (61.9%).
Sleep disturbances, described as “waking during the night sleep due to itching”, were observed in 16.7% of patients with AP.
No dependences were found between methods of evaluation of AP intensity and sex, body mass index (BMI) or time of diagnosis of AP (before or after PV). In addition, no significant correlations were observed between intensity of itch and AP duration, nor time of itch occurrence after contact with water.
The majority of patients with PV were treated with phlebotomy (66.7%) and 5-hydroxyurea (5-HU) (71.6%). Acetylsalicylic acid (40.2%), clopidogrel (9.8%), anagrelide (7.8%) and pipobroman (2.9%) were used more rarely. Among participants receiving 5-HU, a higher intensity of pruritus according to VAS and VRS was revealed (p = 0.05 and p = 0.026, respectively). Antipruritic treatment sensu stricto (antihistamines) was received by only 3 patients (7.1%) and none experienced any clinical improvement.
AP, as a common feature of PV, has a significant influence on patients’ quality of life and can lead to the development of hydrophobia (17). However, there is a lack of published information on the extent of AP, its characteristics and treatment. There is only one prospective study with a representative group of patients (18).
The occurrence of AP in patients with PV varies from 31% to 68.2%, which is consistent with our findings (6, 18). In opposition to common skin diseases, such as atopic dermatitis (85%) (19) or chronic urticaria (97%) (20), the frequency of pruritus in patients with PV is much lower. However, in other internal disorders, such as diabetes mellitus (8%) (21) or uraemic pruritus (25–52.6%) (22, 23), itching occurs more rarely or equally with AP in PV. PV-associated pruritus puts an additional burden on patients with PV.
Despite the onset of AP preceding the diagnosis of PV in approximately half of studied cases, only a small percentage of the physicians consider a haematological condition as an underlying cause. This provides strong support for the need for improvement in medical knowledge among practitioners dealing with patients who report itching. Of course, it is also true that AP may also occur simultaneously with, or may follow the diagnosis of, PV (24).
In concordance with the study by Siegel et al. (18) PV-associated pruritus was recognized more often among women and described by patients as a moderate-to-strong itching sensation, and less often as burning or prickling of the skin.
The mean AP intensity evaluated with VAS (4.8 ± 1.9 points) was lower in comparison with pruritus observed in common dermatoses, such as atopic dermatitis (7.9 ± 2.2 points) (13), chronic urticaria (7.5 ± 1.8 points) (24) or lichen planus (6.5 ± 2.7 points) (25). However, with regard to other internal diseases, such as uraemic pruritus (4.1 ± 2.0 points) (26) or diabetes mellitus (4.7 ± 2.8 points) (27), the severity of AP appears to be comparable. Considering the assessments conducted with 4-item Itch Questionnaire, in opposition to other diseases presenting similar symptoms, such as atopic dermatitis (14.0 ± 4.4 points) (13) or uraemic pruritus (8.2 ± 4.5 points) (15), the mean results for AP were somewhat lower (6.0 ± 2.9 points).
Taking into account the treatment of PV (including phlebotomy, acetylsalicylic acid, clopidogrel, anagrelide and pipobroman), no significant associations were found with the intensity of AP. There is, however, some evidence that treatment with aspirin could alleviate pruritus in PV due to probable involvement of platelets (PLT) and prostaglandin (28). This phenomenon is, in some way, clarified by the research performed by Gangat et al. (7). In their study, the prevalence of PV-associated pruritus was lower in those with an arterial thrombosis due to possible qualitative or quantitative alterations in PLT-released products. Moreover, among patients who smoke or who have diabetes (groups with higher risk of arterial thrombosis), the prevalence of pruritus was also lower. This could be explained by a common pathogenetic mediator for pruritus and arterial thrombosis in PV, which is functionally vulnerable to both smoking and diabetes. The authors identified PLT and increased intraplatelet serotonin levels among smokers and diabetic patients as possible contributors (7). In contrast to this, amongst patients with PV, PLT-rich plasma serotonin levels are decreased (29), which could be somehow explained by the efficiency of serotonin-reuptake-inhibitors (SSRI) in the treatment of some cases of PV-associated pruritus. Further research into the morphological parameters and their associations with pruritus could contribute to better understanding of the pathophysiology of AP and its management.
Treatment of PV-associated pruritus is a constant challenge. The lack of insight into the pathogenesis of AP is arguably the main reason for inadequacy in earlier therapy. The most frequently prescribed drugs are antihistamines; however, their effectiveness in reduction of AP is variable; from no effect (30) to 47% response (4). Furthermore, it should be emphasized that the main issue regarding treatment of AP is not only the ineffectiveness of current therapies, but also the lack of prescription of any anti-pruritic treatment for patients with AP. Antipruritics were administered to only 7.1% of patients with AP in our study.
Other effective therapeutic options for PV-associated pruritus could include interferon alpha (IFN-α) (31–35), alkalization of bathing water with the addition of sodium bicarbonate (36), busulfan, danazol (8, 37), phlebotomy (38), narrow-band ultraviolet B (UVB) phototherapy and oral psoralen photochemotherapy (PUVA) (39, 40). Although the results were promising, the tested groups did not provide a sufficient demographic (from 2 to 22 patients). SSRIs (e.g. paroxetine), pregabalin and naltrexone also presented favourable results; however, in these studies also only small groups of patients were treated (41–43). Alkalization of bath water, PUVA, IFN-α, SSRI, busulfan or danazol were not utilized as therapy in our patients.
According to recent data, modern agents, such as JAK2-/JAK1-inhibitors and inhibitors of the mammalian target of rapamycin (mTOR), presented encouraging and promising outcomes (44, 45). Taking into account that JAK2V617F-homozygous patients with PV showed an increased frequency of pruritus compared with heterozygotes, drugs such as ruxolitinib could potentially serve a therapeutic approach for management of AP among patients with PV (46, 47).
Despite the correction of haematological parameters, during treatment with cytoreductive agents the severity of pruritus could be increased. This is explained by the symptomatic action of these drugs without, in fact, affecting the clinical course of disease (48). This phenomenon could also be explained by the recent data with regards to treatment with JAK2-/JAK1-inhibitors, which could bring relief in the general symptoms, such as fatigue, night sweats or itching, due to the targeting of the signal pathways of the erythropoietin (EPO) receptor.
In conclusion, AP is a frequent, although seemingly underestimated, problem among patients with PV. It should be highlighted that one-third of all patients with AP in our test group regularly avoided any contact with water. The findings of the current study have provided additional information regarding the characteristics of AP in polycythemia vera, especially in terms of the sensory and affective dimensions of the itching sensation.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize