


1Dermatology and Venereology Unit, Department of Medicine Solna, Karolinska Institutet, 2Dermatological and Venereal Clinic, Södersjukhuset, 3Institute of Environmental Medicine, Karolinska Institutet, 4Department of Occupational and Environmental Medicine, Stockholm County Council; Unit of Environmental Epidemiology, Institute of Environmental Medicine, Karolinska Institutet, 5Department of Clinical Science and Education, Södersjukhuset, Karolinska Institutet, 6Sachs’ Children and Youth Hospital, Södersjukhuset, 7Department of Women’s and Children’s Health, Karolinska Institutet, 8Department of Biosciences and Nutrition, Karolinska Institutet, 9Department of Molecular Medicine, Karolinska Institutet at Karolinska University Hospital, 10Department of Dermatology, Karolinska University Hospital Solna, Stockholm, Sweden, and 11St John’s Institute of Dermatology, King’s College London, London, UK
Information on factors of importance for remission of eczema is scarce. This study explored factors related to the remission and course of preschool eczema (PSE) (eczema at 1, 2 and/or 4 years of age) to 16 years of age (n = 889) in a Swedish cohort. Half of the children were in complete remission by school age (at age 8, 12, and 16 years). In multivariate prognostic models, persistent PSE (eczema at 1, 2 and 4 years of age) (odds ratio 0.27 (95% confidence interval 0.18–0.41)), PSE with sleep disturbance (due to itch at least once a week at 1, 2 and/or 4 years of age) (0.59 (0.43–0.81)), parental allergy (0.73 (0.55–0.96)), parental smoking at child’s birth (0.70 (0.50–0.99)) and filaggrin mutation (R501X, R2447X, 2282del4) (0.47 (0.26–0.85)) were inversely associated with complete remission by school age. Male sex (1.37 (1.03–1.82)) and exclusive breastfeeding ≥4 months (1.44 (1.01–2.05)) were positively associated with complete remission by school age. In conclusion, half of the children with PSE were in complete remission by school age. The most important prognostic factors were persistent PSE and PSE with sleep disturbance due to itch.
Parents, patients, and health care providers often request information on eczema prognosis. In this study, we show the natural course of preschool eczema (onset before age 4) up to age 16 years among children in the general population. By school age (from 4 to 16 years), half of the children were free of eczema symptoms (complete remission), 8% had persistent eczema, and 41% had periods with and without eczema. Persistent preschool eczema, preschool eczema with sleep disturbance due to itch, and filaggrin gene mutations were strongly associated with reduced likelihood of complete remission by school age.
Key words: atopic dermatitis; birth cohort; breastfeeding; filaggrin mutations; natural course.
Accepted Mar 1, 2018; Epub ahead of print Mar 2, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Emma Johansson, Department of Dermatology and Venereology, Södersjukhuset, Sjukhusbacken 10, SE-118 83 Stockholm, Sweden. E-mail: emma.k.johansson@sll.se
Eczema (atopic dermatitis (1)) is an itchy inflammatory skin disease that has a considerable impact on health-related quality of life (2). Eczema affects approximately 20% of children worldwide (2), and can debut at any age, but in most cases appears before 2 years of age (3). With increasing age, eczema becomes less common. The prevalence of eczema among adolescents is approximately 10% (4) and among adults 2–10% (5, 6). The course of eczema is sometimes intermittent, with episodes of exacerbations followed by disease-free periods. In 3 birth cohort studies, approximately half of all children with eczema at 0–2 years of age were in remission by age 7, 12 and 18 years, respectively (7–9). Furthermore, a systematic review and meta-analysis showed that only 1 in 5 children with eczema had disease persistence for a period longer than 8 years (10).
Factors of importance regarding the persistence of eczema have been well studied. In a recent systematic review and meta-analysis, Kim et al. (10) concluded that most childhood eczema remitted by adulthood. In the pooled analysis, 80% of childhood eczema had remitted 8 years after diagnosis and more than 95% had remitted 20 years after diagnosis. Persistent eczema in childhood, individuals with more severe eczema, older age at onset (after age 2 years), and female sex were all associated with disease persistence. IgE sensitization to one or more allergens was not associated with disease persistence (10). Other studies have shown that filaggrin (FLG) mutation is associated with persistence of childhood eczema (11, 12).
However, knowledge regarding factors of importance for the remission of childhood eczema is deficient. In a systematic review from 2015, von Kobyletzki et al. (14) explored factors that predicted the remission of infant eczema, but only 2 studies (7, 13) were suitable for inclusion. In 1 of these studies (7), it was shown that having fewer than 2 atopic family members was associated with remission within 6–7 years. Strong atopic heredity, IgE sensitization, severe eczema, and early wheeze were associated with non-remission. In the same study, no association was found with having older siblings, breastfeeding, parental smoking, maternal smoking during pregnancy, or parental level of education (7). Still, it is largely unknown which factors predict the remission of eczema, and since information on disease prognosis is often requested by parents, patients, and healthcare providers, further studies are highly warranted.
The aims of this study were: (i) to explore the natural course of preschool eczema (PSE) from birth to age 16 years using data from the Swedish population-based Children Allergy Milieu Stockholm Epidemiology (BAMSE) birth cohort; (ii) to identify factors of importance for the remission of PSE with a particular interest in complete remission by school age; and (iii) to explore whether prognostic models could be useful to predict the remission of PSE.
The BAMSE project is a population-based birth cohort. Parents of all children born in pre-defined areas of Stockholm County between February 1994 and November 1996 were asked to participate (n = 7,221). The final study cohort (n = 4,089) comprised 75% of the eligible children (15). At inclusion, the parents completed a baseline questionnaire covering detailed data on residential characteristics, environmental factors, and parental allergy. When the children were 1, 2, 4, 8, 12 and 16 years old, the parents completed questionnaires regarding symptoms of eczema, rhinitis and asthma in the last 12 months, as did the adolescents at ages 12 and 16 years. At age 16 years, 3,115 (76%) subjects remained in the cohort. All children were invited to clinical examinations, including blood sampling, at ages 4, 8 and 16 years.
Blood was collected for analysis of serum IgE antibodies to common airborne and food allergens at 4 years of age. Airborne allergens were analysed with Phadiatop® (cat, dog, horse, birch, timothy, mugwort, house dust mite, and mold), and food allergens with fx5® (cow’s milk, hen’s egg, cod, soy, peanut, and wheat) using the ImmunoCAP System (Thermo Fisher Scientific, Uppsala, Sweden). The results were expressed as positive (≥ 0.35 kUA/l) or negative (<0.35 kUA/l). All samples were analysed at the Department of Clinical Immunology, Karolinska University Hospital Solna, Stockholm, Sweden, and in accordance with the manufacturer’s instructions.
Genotyping for the FLG mutations common in Scandinavia was carried out among children who provided blood at 8 years of age (16). Successful analysis was performed on 1,940 of 2,025 (95.8%) of the children. Genotyping was performed using TaqMan allelic discrimination for R501X and R2447X on the ABI Prism 7500 detection system in accordance with the manufacturer’s protocol (Applied Biosystems, CA, USA) and MALDI-TOF (matrix-assisted laser desorption/ionization-time of flight; Sequenom GmbH, Hamburg, Germany) for 2282del4. Primer sequences, amplification conditions, and allele sizes are available on request. Additional genotyping was performed among children who provided blood at 16 years of age. The success rate was 99.8% (2,126 of 2,130). TaqMan SNP Genotyping Assays for all 3 mutations were used (obtained from Applied Biosystems, CA, USA). Genotyping was performed in 384-well microtitre plates containing a minimum of 10 ng DNA and TaqMan Mastermix (Applied Biosystems) in a total 10 µl reaction. Thermal cycling conditions were set according to the manufacturer’s protocol. All samples were analysed in triplicate. Analysis of sample genotypes was performed using the QuantStudio™ 6 and 7 Flex real-time PCR system software v1.0 (Applied Biosystems). Children with a mutation in any of the positions 2282del4, R501X, or R2447X were classified as having a FLG mutation.
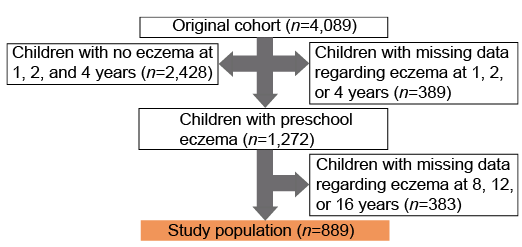
Children with PSE (n = 889) and with data on eczema at ages 8, 12 and 16 years constituted the study population (Fig. 1). FLG mutation analyses at ages 8 and 16 years and IgE sensitization at age 4 years were available for a subset of children (n = 764 and n = 671, respectively).
Fig. 1. Study flowchart.
The definition of PSE was based on parental-reported eczema at ages 1, 2 and/or 4 years. Children with PSE who were classified as having no eczema at ages 8, 12 and 16 years were defined as being in complete remission by school age (children with eczema at 8, 12, and/or 16 years were controls). Definitions of eczema and remission are listed in Table I, and background factors and possible predictive factors in Table SI.
Table I. Definitions of eczema and remission
Background characteristics were expressed as percentages of the total number of individuals observed and 95% confidence interval (95% CI). The prevalence of eczema, asthma and rhinitis were assessed over a 12-month period. Univariate logistic regression was performed for evaluation of the association between possible predictive factors and the dichotomous outcome complete remission by school age, and presented as crude odds ratio (OR) with 95% CI. As a second step, multivariate models were created. It was decided a priori to include sex, socioeconomic factors, parental smoking, heredity, older sibling in household, preschool asthma, and preschool rhinitis in the multivariate model, and other potential predictive factors were included if the crude univariate logistic regression was significant. Backwards selection was performed and variables with p > 0.15 were excluded from the model. Factors that remained in the model were tested for interaction. Each factor was tested pairwise with all other factors. The likelihood ratio test was used to compare models with and without the interaction terms and the interaction was considered significant if p < 0.05. The correct classification rate was calculated as the number of correctly classified individuals divided by the total number of individuals. All statistical calculations were performed with Stata statistical software (release 12.1; StataCorp, College Station, TX, USA).
This study was approved by the Regional Ethical Review Board at Karolinska Institutet, Stockholm. Informed consent was provided by teenagers and guardians.
Of the 3,700 children participating in the BAMSE birth cohort up to 4 years of age, 1,272 (34.4%) had eczema at 1, 2 and/or 4 years of age (PSE). Of these, 889 participated at all follow-ups until age 16 years and were included in the present study (Fig. 1). Background characteristics are shown in Table II. In the study population, 46.1% had onset of PSE before age 1 year, 31.7% between ages 1 and 2 years, and 22.2% between ages 2 and 4 years. Among all children with PSE (n = 889), persistent PSE (eczema at ages 1, 2 and 4 years) was reported by 18.7% (n = 166), while 33.2% (n = 295) of the children reported PSE with sleep disturbance. DNA samples were avail-able for 776 of the children in the study population, and analysis for FLG mutations was successfully performed on 764 of 776 subjects (98.5%).
Table II. Association between risk factors and protective factors in the first 4 years of life and complete remission of preschool eczema (PSE) at ages 8, 12 and 16 years
By school age, half of the children with PSE (50.8%, n = 452) had complete remission of PSE, 8.2% (n = 73) had persistent eczema and 40.9% (n = 364) had eczema at 1 or 2 occasions (intermittent eczema) (Fig. 2). In the group of children with persistent PSE, only 23.5% were in complete remission by school age (no eczema at 8, 12 and 16 years). Complete remission was most common (66.4%) in the group of children with eczema onset in the first year of life (those with persistent PSE excluded, 166 of 410) (Table III). Among children with a history of PSE, 82.2% (n = 731) were in remission at age 16 years (no eczema at 16 years).
Fig. 2. The natural course of preschool eczema (PSE) in the study population (n = 889). Children with PSE (eczema at ages 1, 2 and/or 4 years) in the Swedish population-based Children Allergy Milieu Stockholm Epidemiology (BAMSE) birth cohort were followed up to age 16 years. Children with PSE were classified into complete remission by school age (n = 452), intermittent eczema at school age (n = 364), and persistent eczema at school age (n = 73), based on reported symptoms of eczema and/or reported doctor’s diagnosis of eczema.
Table III. The course of different phenotypes of preschool eczema (PSE)a up to age 16 years
The background factors and other factors possibly associated with complete remission of PSE are shown in Table II, with corresponding crude ORs and 95% CIs. Persistent PSE, PSE with sleep disturbance, FLG mutation, parental allergy, parental smoking at birth, preschool rhinitis, and IgE sensitization to food and/or aeroallergens were all inversely associated with complete remission of PSE by school age. In contrast, exclusive breastfeeding ≥ 4 months and overweight at age 4 years were positively associated with complete remission.
Significant factors from the univariate analyses, and factors of possible importance based on the literature (sex, socioeconomic status, older sibling in household and asthma) were included in a multivariate prognostic model. First, we analysed factors based on questionnaire data; significant factors are shown in Table IV, Prognostic model 1. The following factors were excluded from the prognostic model: preschool asthma (p = 0.79), low socioeconomic status (p = 0.52), preschool rhinitis (p = 0.43), and older sibling in household (p = 0.20). To determine whether the association between exclusive breastfeeding ≥ 4 months and complete remission was affected by disease modification of exposure, the analysis was restricted by excluding children with their first symptom of eczema during exclusive breastfeeding in the first 4 months of life. The multivariate model did not change following this exclusion, and the point estimates in the full model and the restricted model were comparable (data not shown).
Table IV. Multivariate modela of prognostic factors for complete remission of preschool eczema (PSE)
Another prognostic model was created for children with data on IgE sensitization and FLG mutation. All factors explored in Prognostic model 1 were included and data were added from the clinical and laboratory examinations (Prognostic model 2, Table IV). From this new multivariate model, the following factors (with p > 0.15) were excluded: preschool asthma (p = 0.92), overweight at age 4 years (p = 0.78), low socioeconomic status (p = 0.73), preschool rhinitis (p = 0.57), IgE sensitization to aeroallergens at age 4 years (p = 0.81), older sibling in household (p = 0.47) exclusive breastfeeding ≥ 4 months (p = 0.16) and parental allergy (p = 0.19). The point estimates in Prognostic model 2 were comparable with and without inclusion of exclusive breastfeeding ≥ 4 months and parental allergy (data not shown).
The developed Prognostic model 1 exhibited sensitivity of 78%, specificity of 49%, positive predictive value (PPV) of 61% and negative predictive value (NPV) of 68%. The efficacy of the prognostic model (correct classification rate) was 63%. The corresponding results for Prognostic model 2 were: sensitivity 75%, specificity 54%, PPV 62%, NPV 69% and efficacy 65%.
Persistent PSE, PSE with sleep disturbance, FLG mutation, female sex, parental smoking, exclusive breastfeeding < 4 months and parental allergy were all significantly inversely associated with complete remission of PSE in Prognostic model 1 and/or Prognostic model 2. In the study population, none of the children had all 7 risk factors. Boys without any of these factors had a probability of 71% to be in complete remission by school age, and the corresponding probability for girls was 60%. The probability for complete remission was 68% among children with 0–1 factors (n = 273), 49% among children with 2–3 factors (n = 475), and 25% among children with 4–6 factors (n = 141).
Out of the children with PSE, recruited from the general population, approximately half were in complete remission by school age and by age 16 years more than 80% were in remission. In multivariate Prognostic model 1 (based on questionnaire data), exclusive breastfeeding ≥4 months and male sex were significantly associated with complete remission of PSE by school age. Furthermore, persistent PSE and PSE with sleep disturbance (indicating a more severe PSE), as well as parental allergy and parental smoking, were significantly associated with reduced likelihood of complete remission by school age. In Prognostic model 2 (including children with data on IgE sensitization and FLG mutation), having a FLG mutation was significantly associated with reduced likelihood of complete remission by school age. The developed prognostic models had correct classification rates of 63% (Prognostic model 1) and 65% (Prognostic model 2), respectively. Thus, the factors included in these models were insufficient for full prediction of complete remission.
Two modifiable prognostic factors (Prognostic model 1) were identified. First, exclusive breastfeeding ≥4 months was associated with complete remission, also in the restricted model excluding children who had symptoms of eczema during breastfeeding. Other studies have not found an association between breastfeeding and remission of eczema (7, 17). In the current study, exclusive breastfeeding was no longer a significant prognostic factor when data from laboratory examinations were included in the prognostic model (Prognostic model 2). However, the point estimate was comparable and the non-significant result from Prognostic model 2 could be due to lack of power. Both our Prognostic model 2 and previous studies (7, 17) had smaller study populations compared with our model based on questionnaire data (Prognostic model 1). Furthermore, parental smoking in infancy (median at age 2 months) was associated with a reduced likelihood of complete remission. Parental smoking has not been associated with remission or with non-remission of eczema in other studies (7, 17). Parental smoking is significantly more common among children from households with low socioeconomic status. However, the associations between complete remission of PSE and parental smoking were not affected when the final prognostic models were adjusted for socioeconomic status. Since our definition of socioeconomic status is based on profession, we cannot rule out that parent’s education level or the income of the household is a confounder for this association or that any other residual confounding could explain these findings. Encouraging exclusive breastfeeding for 4 months or longer and recommending parents to refrain from smoking might improve the prognosis for a child with PSE and contribute to higher rates of complete remission of PSE.
To our knowledge, the current study encompasses the largest cohort of children (n = 889), recruited from the general population, with early childhood eczema and with data from birth to adolescence. The prevalence of complete remission after age 4 years was 51% based on measurements from 3 follow-ups covering a period of 12 years. This finding is comparable with those of other studies (7, 9). In a population-based setting with yearly follow-ups to age 7 years (n = 192), 43% of children with infantile eczema (eczema ≤ age 2 years) were in complete remission from age 2 years (7). In the Isle of Wight birth cohort, in the UK, 42% of 169 children with eczema at 1 or 2 years of age went into complete remission by age 18 years (9). The higher proportion of remission in the current study could be because the other studies were based on prognosis of infantile eczema (eczema at age 1 and/or 2 years). We have previously shown that 39% of children with infantile eczema were in complete remission by age 12 years (13), which is comparable.
IgE sensitization to food allergens at age 4 years tended to be inversely associated with complete remission, but did not reach significance. Early IgE sensitization to foods has been shown to be associated with persistence of eczema in other studies (7, 18), but IgE sensitization to one or more allergens was not associated with persistence in a systematic review (10). Further studies with large sample sizes are necessary to analyse the association between IgE sensitization and remission of eczema.
In this large population-based material, we show that FLG mutation is associated with reduced likelihood of complete remission of PSE, which is consistent with previous findings (11, 12, 19). However, FLG mutations are population specific (20), which might influence the results and applicability of FLG mutations as a predictive factor.
This study has several strengths. Firstly, the large number of participants recruited from the general population with follow-up from birth to 16 years. The eczema criteria in the questionnaire have been validated with a sensitivity and specificity of 92% and 100%, respectively (21). Thus, the risk of misclassification of PSE is probably low. The longitudinal design with a high follow-up rate allowed us to analyse remission throughout school age. However, it is possible that the participants had symptoms of eczema in time periods not covered by the questionnaires, which is a limitation. Another limitation is that data on FLG mutation and IgE sensitization were available only for a subset of the study population, which resulted in limited power for analyses including these factors. Since this is a secondary analysis of the BAMSE birth cohort, we could only explore possible prognostic factors from already collected material. Therefore, there was little opportunity to choose which prognostic factors to explore. For example, it would have been interesting to study if effectiveness of disease treatment was associated with remission of eczema, but we could not evaluate this issue further. On the other hand, it is a strength that the BAMSE dataset is substantial and that we could analyse most factors previously known as risk factors, including FLG mutation, for both incident and persistent eczema.
The understanding of prognostic factors for remission of PSE is of major importance for affected families, as well as for healthcare professionals providing information and guidance. The findings of the current study contribute to the knowledge of factors important for prediction of remission of eczema, including at least 2 modifiable factors. Healthcare providers can convey this information to parents of children with eczema. In our study, both persistent PSE and PSE with sleep disturbance were strongly associated with reduced likelihood of PSE remission. This finding is in line with a previous systematic review and meta-analysis (10). It has been shown that frequent use of emollients can delay onset of eczema among infants at high risk for eczema (22, 23). However, it is unknown whether treatment of eczema early in life affects long-term prognosis. Hypothetically, the factors persistent PSE and PSE with sleep disturbance, which in our study were negatively associated with remission of PSE, could be modified by early and effective treatment of eczema. To speculate further, it is possible that promising new and more effective treatments (24) can interfere with early disease persistence resulting in a better long-term disease control and a higher degree of remission.
More than 50% (452 of 889) children with PSE in this Swedish cohort were in complete remission by school age, and more than 80% were in remission at age 16 years. The prognostic models created, which included factors based on questionnaires and laboratory findings, were insufficient for prediction of complete remission of PSE by school age. Persistent PSE and PSE with sleep disturbance were strongly associated with reduced likelihood of complete remission by school age. The findings of the current study highlight the need for future research focusing on disease-modifying therapies and their consequences for disease prognosis.
The authors would like to thank all the children and parents who have participated in the BAMSE project.


 Click to show fullsize
Click to show fullsize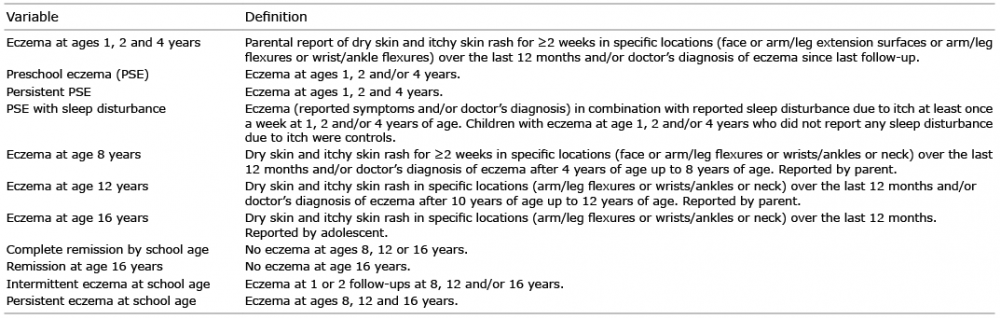 Click to show fullsize
Click to show fullsize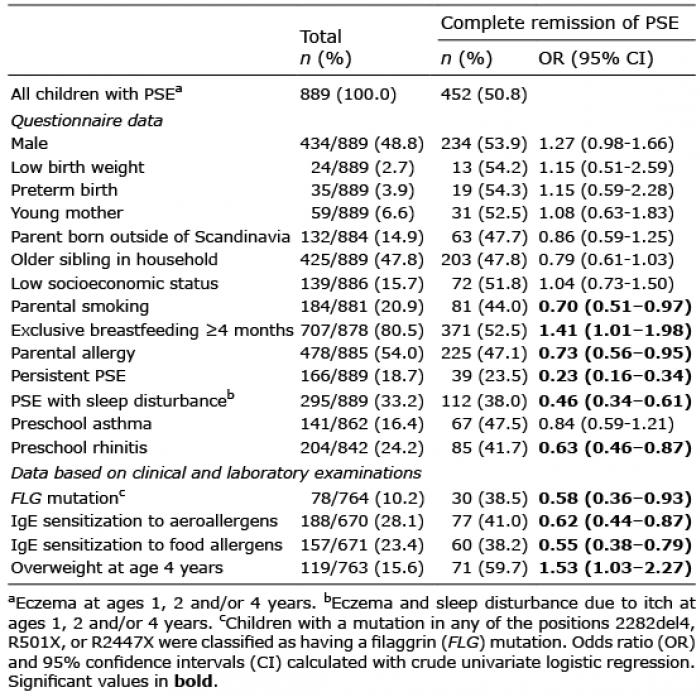 Click to show fullsize
Click to show fullsize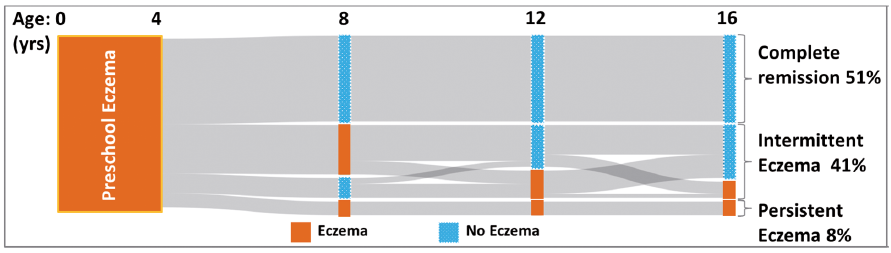 Click to show fullsize
Click to show fullsize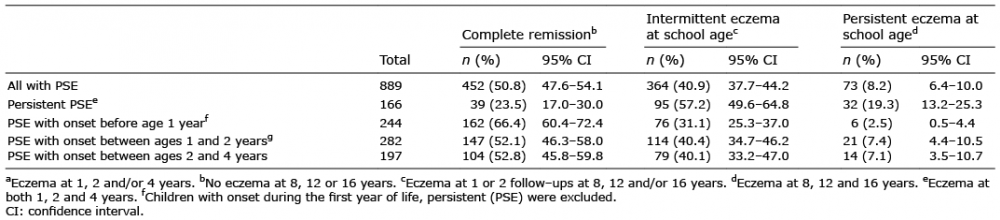 Click to show fullsize
Click to show fullsize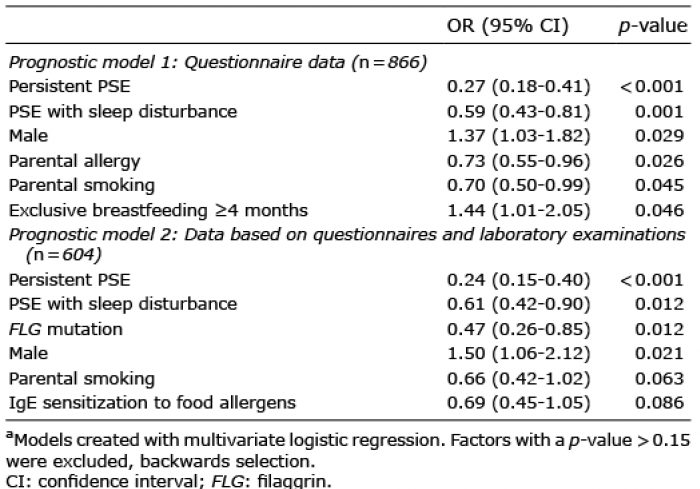 Click to show fullsize
Click to show fullsize