


Department of Dermatology and Pediatric Dermatology, National Centre for Rare Skin Disorders, Hôpital Saint-André, Bordeaux, France
Folliculitis decalvans (FD) is a chronic inflammatory disease leading to scarring alopecia with poorly defined pathogenesis. The aim of this study was to investigate the expression of markers associated with the activation of innate immune signals, such as inflammasome (NALP1 and NALP3), interleukin (IL)-1β and IL-8 and type I interferon (MxA). A retrospective monocentric study was conducted and included 17 patients with FD with available biopsies. Disease activity (stable vs. active) was defined clinically and histologically. Immunostaining was performed using antibodies directed against NALP1, NALP3, IL-1β, IL-8, and MxA on FD skin biopsies. Results were compared with normal controls and lichen planopilaris. Eleven patients had active disease and 6 had stable disease. NALP1, NALP3, and IL-1β expression were significantly increased in hair follicles in FD compared with controls and lichen planopilaris. This study highlights the predominant immune signal associated with inflammasome activation in FD, suggesting the use of IL-1β blockade in FD.
Folliculitis decalvans (FD) is a rare chronic inflammatory disease leading to scarring alopecia and major impact on patients’ quality of life. To date, FD could be seen as a near orphan disease because of the lack of effective therapies. Our study highlights the role of innate immune response involving the inflammasome and the Il-1β signalling path-way in FD supporting the potential use of IL-1β blockade therapies in FD.
Key words: folliculitis decalvans; cicatricial alopecia; inflammasome activation; treatment; immunomodulating therapy.
Accepted Mar 15, 2018; Epub ahead of print Mar 15, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Julien Seneschal, Department of Dermatology and Pediatric Dermatology, National Centre for Rare Skin Disorders, Hôpital Saint-André, 1 rue Jean Burguet, FR-33075 Bordeaux Cedex, France. E-mail: julien.seneschal@chu-bordeaux.fr
Folliculitis decalvans (FD) is a chronic inflammatory disease leading to primary cicatricial alopecia, with a long-standing course. FD is difficult to treat. It is the second cause of cicatricial alopecia after lichen plano-pilaris (1). This condition, occurring in middle-aged adults, is characterized by the development of alopecic patches with slowly centrifugal spread, predominantly in the vertex and occipital area of the scalp. FD is associated with recurrent perifollicular erythema, follicular pustules and haemorrhagic crusts, leading to discomfort, pain and pruritus (1–3). Understandably, the result is reduced self-esteem and psychological effects impacting patients’ quality of life (4). Histological findings include a dense perifollicular neutrophilic infiltrate, affecting the upper and middle part of the follicle in the acute phase of the disease, evolving to a lympho-plasmocytic nature extending to the advential dermis, with psoriasiform epidermal hyperplasia, deep follicular microcysts, polytrichia, disappearance of the sebaceous glands and dermal fibrosis in the late-stage (1, 5).
The pathogenesis of FD is unknown. Early studies evaluated the role of the microbiota in the pathogenesis of FD. In 1999, Powell et al. (2) hypothesized that FD could be the result of an abnormal response to toxins released from a straightforward infection with Staphylococcus aureus, with no defect in the T- or B-cell responses. The crucial role of bacterial biofilms, which can be present in the anaerobic part of the hair follicle, was suspected (6). On the other hand, antibacterial treatments have only a suspensive efficiency and several observations described improvement under immunomodulating treatments (7–9). Paradoxically, inflammatory pathways implicated in this condition remain unknown. The implication of inflammasome has already been demonstrated in keratinocytes and neutrophil-rich dermatitis (10). Thus, the presence of a neutrophilic infiltrate in FD skin, suggest a role of inflammasome in FD (which could be a consequence of microbiota dysbiosis), as has been demonstrated in other diseases, such as psoriasis or hidradenitis suppurativa (HS) (10).
Inflammasome is part of innate immunity and is activated under infectious trigger or stress, leading to the production of pro-inflammatory cytokines, such as IL-1β (11). Although previous studies have suggested a role of inflammation and microbiota in FD, no clear evaluation of the innate immune component has been performed. The aim of this study was to analyse, in skin lesions of stable and active FD, the presence and intensity of markers associated with the inflammasome: NALP1, NALP3, IL-1β, and the expression of IL-8, a cytokine induced in response to IL-1β, leading to the recruitment of neutrophils.
A retrospective monocentric study was conducted between November 2014 and May 2015 at the Department of Dermatology, Hôpital Saint-André, Bordeaux, France. All patients aged over 18 years, with a diagnosis of FD made on clinical criteria (history recurrent crops of pustular follicular inflammatory lesions on vertex, scarring alopecia, disease lasting more than 6 months), photography and pathology (scalp biopsies with perifollicular fibrosis and neutrophilic infiltrate) were included in the study. Information on age, sex, personal and family medical history, and comorbidities were obtained. Clinical photographs of the lesions were also analysed. All paraffin-embedded skin biopsies obtained for diagnosis purpose were re-evaluated independently by a pathologist to confirm the pathological diagnosis. Paraffin-embedded skin biopsies obtained from patients affected by lichen planopilaris (LPP) were obtained as control in another common chronic inflammatory hair disorder. Healthy hair scalp specimens were obtained from surgical excision of trichilemmal cysts.
The degree of activity of FD was evaluated retrospectively by analysing clinical records and photographys taken at the time of the skin biopsy. Mainly, we considered 2 distinct clinical subtypes of FD: (i) “active disease”, characterized by the presence of crusts and pustules associated with pruritus and/or pain; and (ii) “stable disease”, consisting of perifollicular hyperkeratosis and erythema at the edge of cicatricial lesions.
Sections 3 μm thick were prepared from formalin-fixed, paraffin-embedded skin biopsies. Standard haematoxylin and eosin staining was performed for pathological diagnosis and neutrophils counts. The inflammatory infiltrate was characterized by immunochemistry. T cells were stained using anti-CD3 (1:100, M7254, AGILENT, Santa Clara, CA, USA), plasma cells were stained using anti-CD138 (1:50, MI15, AGILENT) and neutrophils were stained using anti-CD15 (1:20, MMA, BD Biosciences, Franklin Lakes, NJ, USA). Labelling for NALP1 (naply1-4, 1:50, ab16091, Abcam, Cambridge, UK), NALP3 (1:1000, ab214185, Abcam), IL-1β (1:500, NB600-633, NovusBio, Littelton, CO, USA), IL-8 (1:20, NBP2-33819, NovusBio) and MxA (M143, dilution 1:100, from Professor Haller, University of Freiburg, Freiburg, Germany), was performed on paraffin-embedded tissue sections, as described previously (12, 13). Secondary labelling was performed using the LSAB2 kit (AGILENT). Appropriate isotype-matched controls were included. The stained slides were analysed independently by 2 investigators (AE, JS) in a blinded manner. Cells were counted per 3 high-power fields (HPF) with an original magnification × 400, and the mean number was calculated. Neutrophils, T cells and plasma cells were counted per 3 high-power fields (original magnification × 400) and the mean number was calculated. The expressions of NALP1, NALP3, IL-1β, IL-8 and MxA were scored using a semi-quantitative method (0 = no expression; 1 = weak expression; 2 = fair expression; 3 = strong expression).
The non-parametric Mann–Whitney U test was employed to compare the expression of NALP1, NALP3, IL-1β, IL-8 and MxA in different disease subsets and healthy controls in the skin. p < 0.05 was considered significant and p < 0.01 highly significant.
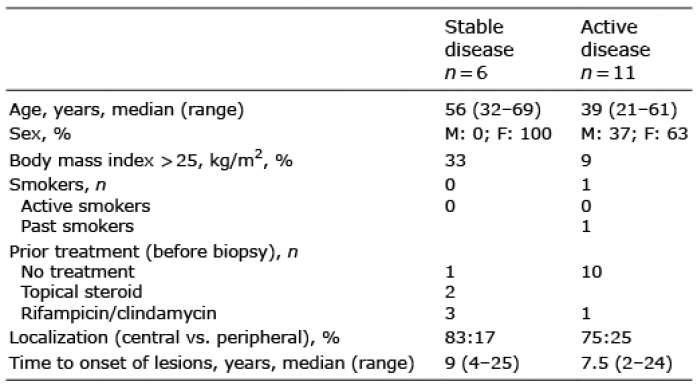
Patients’ characteristics are shown in Table I. Seventeen patients with FD were included, 4 men and 13 women, median age 46 years (range 21–69 years). Eleven patients were classified as active disease and 6 as stable disease. None of the patients were active smokers (only one patient was a past-smoker). Three patients had a body mass index (BMI) > 25. The most affected area was the vertex (88%) (Fig. 1a).
Table I. Clinical features of patients with folliculitis decalvans (FD)
Fig. 1. Clinical and histological characteristics of patients with active and stable folliculitis decalvans (FD). (a) Lefthand panel: stable disease characterized by the absence of pustules but a mild erythema and perifollicular hyperkeratosis at the edge of the plaque. Righthand panel: active disease characterized by erythema, crusts and pustules. (b) Haematoxylin and eosin staining and immunohistochemistry showing CD15+ neutrophils, CD3+ T cells and CD138+ plasma cells in active and stable FD. (c) Quantitative analysis of CD3+ T cells; (d) neutrophils; (e) CD138+ plasma cells. Cells were counted per 3 high-power field; original magnification ×400. Results of multiple donors are plotted and horizontal bars represent the mean (*p < 0.05).
Patients with active disease were mainly those who were referred to our department at the time of diagnosis and who had not previously received local or systemic therapies. Stable patients were mainly patients with a long-lasting evolution of the disease who had previously received therapies: local corticosteroids (2/6), and association of rifampicin and clindamycin (3/6), or no treatment prior to biopsy (1/6) (Table I).
Using immunohistochemistry, we first compared the nature of the inflammatory infiltrate within perilesional skin of patients with stable and active FD. Active FD showed a prominent infiltration of CD3+ T cells (Fig. 1b, c) and CD15+ neutrophils (Fig. 1b, d), compared with stable FD. No statistical difference was observed regarding infiltration of CD138+ plasma cells in both conditions (Fig. 1b, e). Altogether, clinical and histological analyses allowed us to classify patients into stable or active disease without difficulty.
As FD is associated with a strong neutrophilic infiltration, we first asked whether it could be associated with inflammasome activation. Expression of NALP1 and NALP3 were detected in the epidermal layer of both stable and active FD compared with controls (data not shown) and no difference was observed between FD and LPP. However, on examining the hair follicle more closely, we found a high follicular expression of NALP1 and NALP3 in FD compared with LPP (Fig. 2a, b, e, f). Importantly, we did not observe any difference between stable and active forms. IL-1β staining was positive in the epidermis and hair follicle at a similar level between active FD, stable FD and LPP (Fig. 2c, g).
Next, we evaluated expression of IL-8, a cytokine released in response to inflammasome activation and leading to the recruitment of neutrophils. As shown in Fig. 2 d, h, we found a high expression of IL-8 in the dermis of FD, mainly localized on the immune infiltrate in both active and stable FD, compared with no or minimal expression in controls and LPP.
Fig. 2. (a) Representative findings of the expression of NALP1, (b) NALP3, (c) interleukin (IL)1β and (d) IL-8, in healthy controls (n = 5), patients with stable folliculitis decalvans (FD) (n = 6), active FD (n = 11) and patients with lichen planopilaris (n = 5). (e–h) Overview of the expression of NALP1, NALP3, IL1β and IL-8. Semi-quantitative analysis of cells expressing the 3 markers. Cells were estimated per high-power field, original magnification ×200. The graph shows mean ± standard deviation (SD). (*p < 0.05).
As we observed inflammasome activation in FD, we wondered whether alternative activation of the innate immune system could be detected in patients with FD. Therefore, to investigate the involvement of type I interferon (IFN), we used a monoclonal antibody directed against MxA (an antiviral protein which is specifically induced by type I IFN). Compared with the high expression found in the epidermis in LPP, active or stable FD showed minimal expression of MxA, suggesting that a type I IFN signature is not the primary mechanism involved in the pathogenesis of FD, contrary to LPP (Fig. 3).
Fig. 3. Representative findings of the expression of MxA in (a) healthy controls (n = 5), patients with stable folliculitis decalvans (FD) (n = 6), active FD (n = 11), and patients with lichen planopilaris (n = 5). (b)Semi-quantitative analysis of cells expressing MxA. Cells were estimated per high-power field, original magnification ×200. The graph shows mean ± standard deviation (SD). *p < 0.05.
Our study included 17 patients with FD. Clinical characteristics were comparable to other FD studies, except that our cohort contains more women (76%). Of the females, 61.5% were over the age of 50 years, supporting the fact that the disease begins later in females. The most affected area was the vertex (88%), in concordance with previous reports (14–16).
Moreover, in our cohort, only one patient was a past-smoker and few of them had a high BMI, suggesting that FD does not share similar comorbidities with other chronic skin inflammatory diseases, such as psoriasis and HS. However, our cohort involved a low number of patients to allow epidemiological conclusions. Until now, in the largest multicentric cohort study on FD epidemiology involving 82 patients, smoking habits and BMI were not analysed (16).
We decided to separate 2 forms of evolutive and continuous FD, separating active and stable FD. We found that this grading was more clinically accurate. To compare the results obtained in patients with active vs. stable disease, we decided, due to the lack of currently severity score available, to define the activity of the disease based on clinical and pathological data, as described in our methodology section. The results of this comparison showed a real difference in the immune infiltrate between active and stable disease.
Our immunostaining studies revealed several new features that have not been described previously. First we demonstrate that FD is associated with increased expression of NALP1, NALP3 and IL1β, mainly in hair follicles, associated with increased expression of IL-8, leading to the recruitment of neutrophils into the skin. This immune response was not associated with a type I IFN signalling as classically observed in LPP (17). Importantly, no difference was found between patients defined as stable vs. active, suggesting that despite low clinical activity in stable disease, there is still a persistent cause of inflammation, as bacterial biofilms. Given the importance of inflammasome in FD demonstrated in our study, comparing inflammasome with persistence of biofilms could be interesting for further research studies.
Interestingly, a recent hypothesis highlighted similarities between HS and FD (5), both follicular, chronic diseases in which antibiotics are efficient, but always temporary, and both neutrophilic diseases. While cytokine expression is better known in HS, our study highlights new similarities, showing, as in HS, an inflammasome activation (18).
FD remains a difficult to treat condition. Current therapies are based mainly on topical steroid or antibiotics and systemic antibiotics (tetracyclines, combination of rifampicin and clindamycin (2)) or dapsone (19), with limited efficacy. Some reports have suggested the use of anti-tumour necrosis factor α in recalcitrant FD (7–9). Our study supports the use of IL1β blockade therapy in FD. Future studies will be important to decipher the role of the inflammasome in the pathogenesis of FD.
In conclusion, FD is a chronic hair disorder that leads to scarring alopecia and has a severe impact on patients’ quality of life. This is one of the most challenging to treat conditions for dermatologists. Increased expression of NALP1, NALP3 and IL1β in FD, demonstrated in our study, support the use of IL1β blockade therapy to improve the management of the disease.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize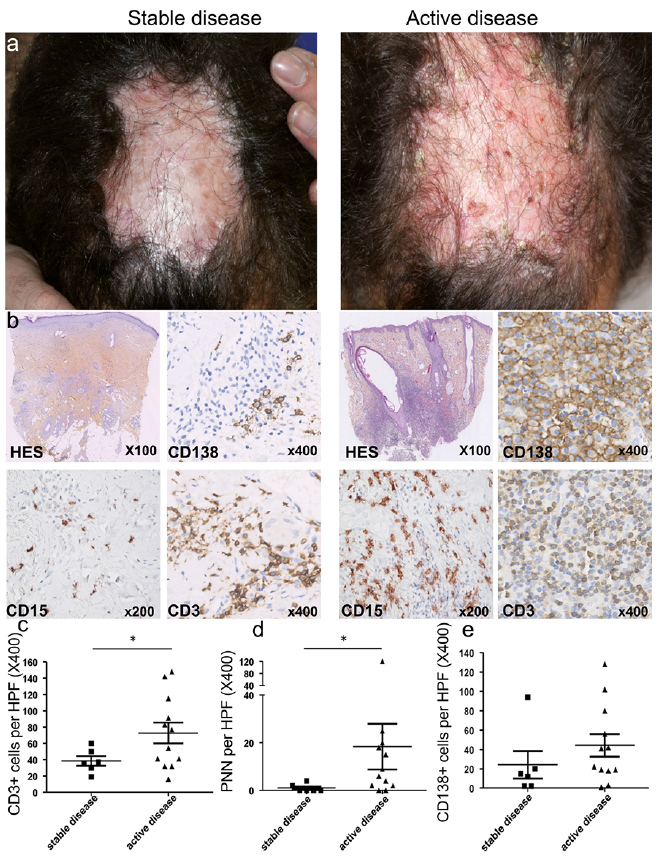 Click to show fullsize
Click to show fullsize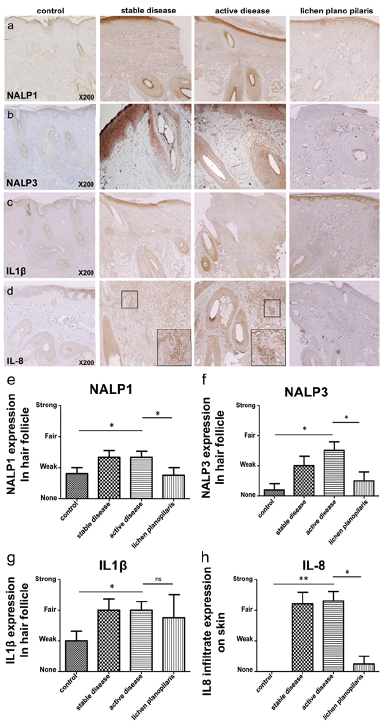 Click to show fullsize
Click to show fullsize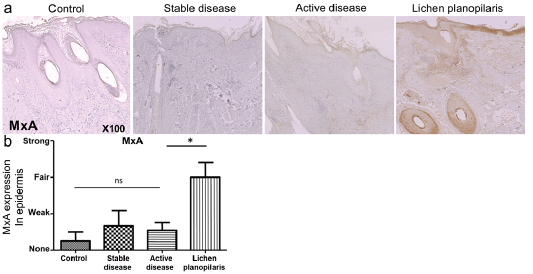 Click to show fullsize
Click to show fullsize