


1University of Tours, 2Department of Dermatology, 3IBiSA Electron Microscopy Facility, 4INSERM U1259, and 5Pediatric Intensive Care Unit, CHRU Tours, Avenue de la République, FR-37044 Tours Cedex 9, France. E-mail: soleducq@gmail.com
A 5-month-old male infant was examined for heterochromia of scalp hair that had occurred 3 months previously. He was born at 39 weeks’ gestation from a primigravida Chinese mother and a French father. From birth, he was admitted to a paediatric intensive care unit because of multiple congenital malformations (tetralogy of Fallot and oesophageal atresia) with no identified syndrome. His foetal karyotype was normal, but no further genetic analyses were performed. His height was 58 cm and weight 5.330 kg. During hospitalization, several bacterial and fungal infections occurred. The infant underwent surgical treatment of oesophageal atresia at age 4 months and received numerous drugs to treat cardiac insufficiency (spironolactone, propranolol, furosemide) and infections (amoxicillin, cefotaxime, gentamycin, cefazolin, tazocillin, fluconazole).
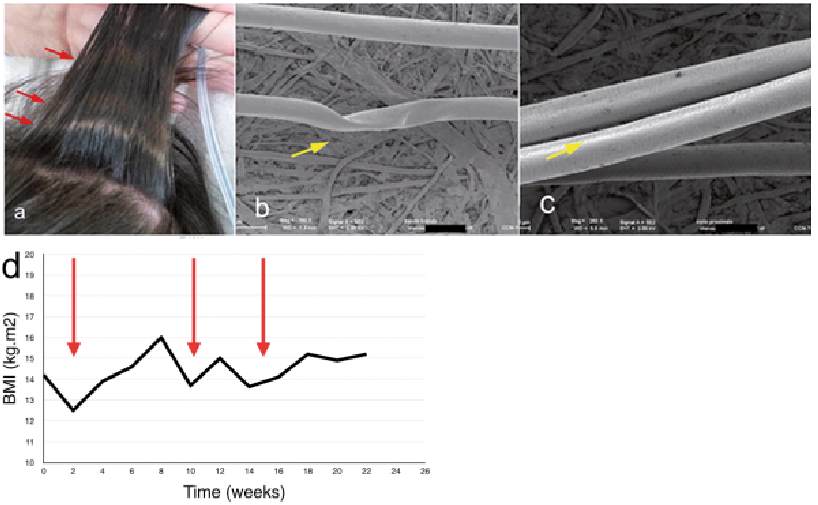
Cutaneous examination was normal. There were no mucosal lesions. The infant had straight dark-brown hair of normal density. The hair featured 3 lighter-coloured bands (Fig. 1a) and the hair shafts were otherwise of normal diameter, with no fragile hair and no alopecia. Laboratory tests demonstrated normal complete blood count, albumin level was 42 g/l (normal >35 g/l) and liver tests gave normal results. Values for vitamins and thyroid function were normal. However, the infant had experienced periods of protein deficiency. Hair samples were obtained for analysis by scanning electron microscopy (SEM), which revealed normal and homogeneous diameter of hair shafts (56 µm) with a well-preserved cuticular pattern. Moderate hair dysplasia with incomplete twisted hair (Fig. 1b), flattening and longitudinal fluting (Fig. 1c) were evidenced in both hypopigmented and normally pigmented areas.
The infant died at age 9 months of Serratia marcescens respiratory tract infection.
What is your diagnosis? See next page for answer.
Fig. 1. (a) Clinical image: 3 bands of lighter-coloured scalp hair in a 5-month-old male. Scanning electron microscopy at magnification (b) ×250 and (c) ×150 showing hair dysplasia (twisted hair and longitudinal fluting). (d) Body mass index curve showing 3 inflections related to the periods of lighter hair lines.
Acta Derm Venereol 2018; XX: XX–XX.
Diagnosis: Flag sign associated with severe malnutrition
Alternating bands of lighter hair and normal hair are called the “flag sign,” which is mainly a consequence of drugs or severe malnutrition/protein deficiency. Hair colour changes might be an adverse event with tyrosine kinase inhibitor treatment, but also chloroquine or propofol (1). One case of flag sign was reported after methotrexate treatment (2). The flag sign has never been specifically reported in children with congenital malformations, but might be due to severe chronic malnutrition, which is mostly described in underdeveloped countries in children with Kwashiorkor syndrome (3). Hair colour changes are associated with other signs, such as oedema, loss of muscle tissue, diarrhoea, vomiting, bloated abdomen, and irritability (4).
Our patient did not receive any drugs that could cause hair lightening. When checking his body mass index (BMI), we observed 3 periods of BMI inflections since birth (Fig. 1d), due to oesophageal atresia and bacterial infections. Retrospectively, these lines of hypopigmentation were related to these periodic episodes of malnutrition. The hair dysplasia observed on SEM was probably related to a malformative syndrome and not malnutrition.
The mechanism of this lightening of hair colour in nutritional deficiency is not fully understood and could be associated with reduced total melanin content of scalp hair, with reduced intake of tyrosine, a key substrate in melanin synthesis (5).


 Click to show fullsize
Click to show fullsize