


1Department of Dermatology, Hospital del Mar – Institut Mar d’Investigacions, Mèdiques (IMIM), Universitat Autònoma de Barcelona (UAB), and 2Adknoma Health Research, Barcelona, Spain
Chronic spontaneous urticaria (CSU) is characterized by heterogeneous activity, evolution, associated comorbidities and response to treatment. The aim of this study was to identify prognostic factors in patients with CSU that predict disease course and response to standard treatments. An observational retrospective study was conducted in a cohort of 549 patients with CSU, comparing patients with isolated CSU and those with CSU with concomitant inducible urticaria (CSU-CIndU). The factors associated with a worse prognosis in terms of duration and/or CSU activity and its episodes were: multiple episodes of CSU (19.2% had more than one lifetime episode of CSU), late-onset (63.6% of patients developed first onset of CSU after the age of 45 years), concomitant CIndU (20.2%) and functional serum auto-reactivity. Patients with CSU-CIndU required more frequent therapy after 5 years and higher doses of 2nd-generation H1-antihistamines. Of patients with a baseline Urticaria Activity Score 7 (UAS7) between 16 and 42, 84.6% required cyclosporine or omalizumab to achieve symptom control, compared with 15.4% of patients with a baseline UAS7 between 0 and 15 (p = 0.0013). Baseline CSU activity is the only factor found to be predictive for refractoriness to treat-ment with H1-antihistamines.
Key words: chronic spontaneous urticaria; disease activity; prognosis; serum autoreactivity; antihistamine refractoriness.
Accepted Apr 12, 2018; Epub ahead of print Apr 12, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Ana M. Giménez-Arnau, Department of Dermatology, Hospital del Mar – Institut Mar d’Investigacions Mèdiques (IMIM), Universitat Autònoma de Barcelona (UAB), Passeig Marítim 25–29, ES-08003 Barcelona, Spain. E-mail: anamariagimenezarnau@gmail.com, 22505aga@gmail.com
Chronic urticaria (CU) is a condition characterized by wheals, angioedema or both, lasting for more than 6 weeks, and sometimes persisting for years. Spontaneous CU (CSU) has unpredictable symptoms, while inducible CU (CIndU) is provoked by, for example, cold, heat, pressure, friction, or contact e.g with proteins, among other factors. Both types can be present concomitantly. The prevalence of CSU in the general population ranges between 0.5% and 1% (1–4). CSU has a significant negative impact on patients’ quality of life, and is a considerable social and healthcare burden (5–7). Some clinical and laboratory parameters have been suggested to be predictive of more persistent and treatment-resistant CSU (4, 8). Autoimmunity may be involved in CSU with higher activity and longer duration (9–14). However, the significance of such observations is controversial (15).
The aim of this study was to identify specific demographic and phenotypic features in a large cohort of patients with CSU that may help to define prognostic factors, and predict disease course and the response to standard treatments, especially H1-antihistamines. The recognition of distinctive characteristics in the patients treated in our clinics would be of value in our daily practice.
This observational study retrospectively reviewed the medical records of 1,056 patients who were registered with the Urticaria Unit of the Hospital del Mar, Barcelona, Spain, from 2001 to 2014. From a total of 997 patients aged over 16 years with a diagnosis of urticaria (acute urticaria, CSU or CIndU), data for 549 patients with CSU were included in the statistical analysis. Clinical features (Table SI), laboratory parameters and extended complementary studies (Table SII), prescribed drugs, response to treatment and evolution data were systematically entered in an electronic case-report form (www.adknoma.com/URTICARIA/login.aspx). CSU features involving activity, diagnostic tools, complementary exploratory tests, comorbidities and therapeutic recommendations were assessed according the EAACI/GA2LEN/WAO/EDF guideline recommendations (1, 2). Serum autoreactivity was tested with the Autologous Serum Skin Test (ASST), Autologous Plasma Skin Test (APST) and Basophil Activation Test (BAT) through CD63 expression (9, 16, 17). Tables SI and SII list the variables recorded in the electronic case-report form (1–3, 9, 18, 19). The Clinical Research-Ethics Committee (CREC) from the Hospital del Mar granted ethical approval for the study (2013/5363/I).
Descriptive statistics are provided for all CSU variables. Data for patients with isolated CSU (is-CSU) and patients with CSU with concomitant CIndU (CSU-CIndU) were compared. Quantitative variables were described using means and standard deviations (SD), and categorical variables using absolute and relative frequencies. Variables were compared between groups using non parametric Mann-Whitney or Kruskal-Wallis test for quantitative variables. Multivariate analysis was also performed using a binomial logistic regression model adjusting for all factors (Table SIII) to assess their joint effect on refractoriness to H1-antihistamines. A p-value < 0.05 was considered statistically significant.
Relevant demographic features. The interval between the first CSU symptom and the baseline visit to the specialized urticaria centre was 4.2 ± 6.8 years (mean ± standard deviation (SD)) (n = 549), revealing a delay in establishing the correct treatment in some patients. Of the total 549 patients, 402 (73%) were female, the mean age at baseline visit was 51.5 ± 15.8 years, and mean age of onset of symptoms 47.3 ± 16.2 years. It is notable that 63.6% (314/494) of patients with CSU were > 45 years of age at the time of first episode of CSU. Of these patients, 74.5% had had urticaria continuously for more than 3 years; a higher percentage compared with the 60% of patients < 45 years of age at first episode of CSU (p = 0.0174). It is notable that 21.7% of patients with CSU were over 65 years of age at the baseline visit. Angioedema was reported in 89/549 of patients with CSU (being present in 16.4% of patients with is-CSU and 15.3% of those with CSU-CIndU).
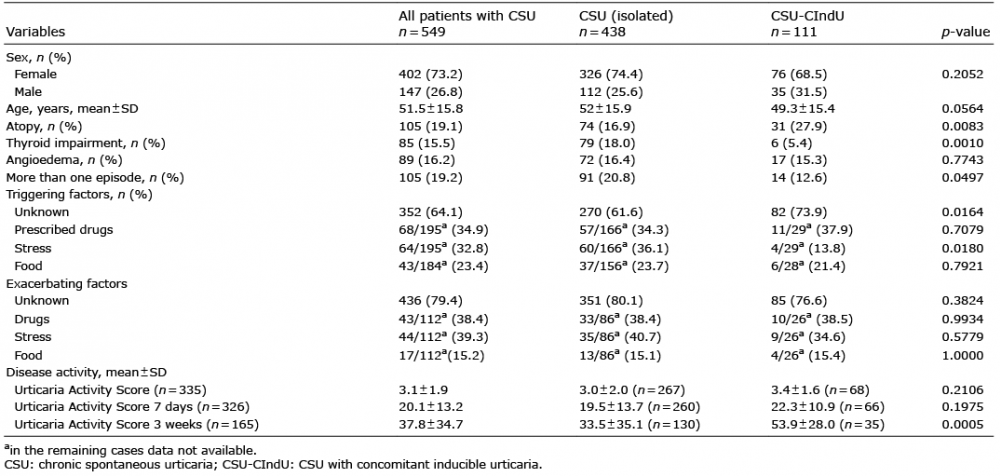
Of 549 patients with CSU, 438 (79.8%) had is-CSU and 111 (20.2%) CSU-CIndU, the most frequent CIndU associated was symptomatic dermographism (SyD) followed by delayed pressure urticaria (DPU) and cholinergic urticaria (ChU) (74.7%, 33.2% and 17.8% respectively; p < 0.0001). Patients with CSU-CIndU were younger than those with is-CSU, but the difference was not statistically significant (49.3 ± 15.4 vs. 52.0 ± 15.9 years; p = 0.0564). The overall demographic and clinical characteristics of patients with CSU, is-CSU and CSU-CIndU are summarized in Table I.
Table I. Clinical variables of the study population
Disease course. Almost 20.0% of patients had had more than one episode of CSU during their lifetime, with long periods completely free of symptoms; 5.8% of them had more than 2 episodes, showing a longer course of CSU. Patients with the is-CSU form had had more recurrences than those with concomitant CIndU (27.0% vs. 17.1%; p = 0.0429) (Table II). Approximately 64% of patients with CSU still needed medical care after 1 year, but this percentage decreased to 32.4% and 17.3% by the 3rd and 5th years, respectively. After 5 years, 8.4% of patients were still visiting our department (Fig. 1). Patients with CSU-CIndU required more frequent therapy after 5 years of follow-up than patients with is-CSU (19.8% vs. 15.1%; p < 0.05).
Table II. Summary table showing the main characteristics of chronic spontaneous urticaria (CSU) related to worse prognosis of the disease in terms of duration and activity
Fig. 1. Evolution of chronic spontaneous urticaria (CSU). Number and proportion of patients with symptomatic CSU (itch and hives) at the different time-points.
Comorbidities associated with CSU. Associated thyroid impairment was recorded in 15.5% of patients with CSU (85/549), mainly corresponding to subclinical hypothyroidism (83.2%). A clear-cut difference regarding thyroid abnormalities was detected between is-CSU (18.0%) and CSU-CIndU (5.4%) patients (p = 0.001). Personal history of atopy was more frequently recorded in patients with CSU-CIndU compared with those with is-CSU (27.9% vs. 16.9%; p = 0.0083). Psychiatric comorbidities were recorded in 4.6% of patients with CSU (25/549), depression being the most frequent comorbidity (72.0%).
Factors triggering/exacerbating episodes of CSU. In a high proportion of the 549 patients with CSU, no clear-cut triggering (64.1%) or exacerbating factors (79.6%) were identified. When present, the most common triggering/exacerbating factors were non-steroidal anti-inflammatory drugs (NSAIDs) and stressful life events. Stress was identified as an important trigger, especially in is-CSU (31.1% in is-CSU vs. 13.8% in CSU-CIndU; p = 0.018). NSAIDs were reported as responsible for exacerbations in all types of CSU.
CSU activity. The Urticaria Activity Score the day before (UAS) and the week before (UAS7) were 3.1 ± 1.9 (range 0–6; n = 335) and 20.1 ± 13.2 (range 0–42; n = 326), respectively, regardless of the treatment followed at this time-point. The UAS were performed once daily. CSU patients with CIndU showed a significantly higher UAS considering the sum of the UAS of the previous 3 weeks (UAS3w) (UAS3w was 53.9 ± 28.0 in CSU-CIndU (n = 35) vs. 33.5 ± 35.1 in is-CSU (n = 130); p = 0.0005) (range UAS3w: 0–120) (1, 15). Despite treatment at the baseline consultation, most of the patients had moderate CSU according to the Disease Activity Categories proposed by Stull et al. (20).
Complementary exploratory tests in CSU. Extended diagnostic measures were carried out routinely in 527 patients (96.0%) (1–3, 19, 21). Any notable laboratory findings are summarized in Table SIV.
High levels of serum alkaline phosphatase (sALP) were detected in 31.9% (n = 129) of patients. Antinuclear-antibodies (ANA) were positive in 31% (n = 48) of patients. Anti-thyroid antibodies, specifically anti-thyroid peroxidase (anti-TPO), were positive in 20.4% (n = 77) of patients, especially in is-CSU (22.0% in patients with is-CSU (n = 65) vs. 14.6% in those with CSU-CIndU (n = 12); however, this difference did not reach statistical significance.
Serum IgE was slightly elevated in 44.3% of patients with CSU (n = 185), but there were no significant differences between is-CSU and CSU-CIndU. Thirty percent of patients with CSU had high serum levels of D-dimer (n = 92). No differences regarding additional exploratory tests (Table SII) were found between is-CSU and CSU-CIndU patients (1–3).
Autoreactive CSU. The ASST was performed in 64.5% of patients with CSU (n = 354), with a positive result in 192 (54.2%). The APST was performed in 41.9% (n = 230) of patients, and was positive in 106 (46.1%). When both tests were performed (n = 227), 39.6% of the sample showed ASST+/APST+, 20.3% ASST+/APST– and only 6.6% showed ASST–/APST+ (p < 0.0001). BAT (CD63 expression) and ASST were assessed in 139 patients, and those with ASST+/CD63+ (n = 25) showed significantly higher UAS7 than patients with ASST+/CD63– (n = 54) (26.57 ± 10.56 vs. 18.40 ± 12.05, p = 0.004) (16). With regard to the positivity of ASST or APST, no significant differences were found between is-CSU and CSU-CIndU patients (53.9% vs. 58.2%, p = 0.4939 and 45.7% vs. 47.4%, p = 0.8229, respectively) (Table II).
Prior to the baseline visit, 88.2% (484/549) of patients had been treated for urticaria. A licensed dose of 2nd-generation H1-antihistamines was the most frequently prescribed first-step treatment, followed by a combination of 1st- and 2nd-generation H1-antihistamines (27.0% and 19.3%, respectively). A further 18.7% had been previously treated with high doses of 2nd-generation H1-antihistamines, and 8.8% had been treated exclusively with 1st-generation H1-antihistamines, which is not a recommended practice due to frequent adverse events (1, 2).
Patients with CSU were treated according to the current published guidelines (1, 2, 19, 21). In our series, 77.7% (332/427) were symptomatic despite being treated with licensed doses of 2nd-generation H1-antihistamines. Refractory patients showed significantly higher baseline UAS7 compared with non-refractory patients (21.3 ± 13.3 vs. 17.7 ± 12.2; p = 0.0359). According to the step protocol recommended by the EAACI/GA2LEN/WAO/EDF urticaria guidelines, 31.8% (n = 164) of patients with CSU achieved complete control with licensed doses of 2nd-generation H1-antihistamines, and 33.7% (n = 174) required an increased dose. Patients with CSU-CIndU required higher doses of 2nd-generation H1-antihistamines more frequently than patients with is-CSU (43.0% vs. 31.3%; p < 0.05) (1, 2). Such patients who were refractory to antihistamines had a third-line treatment added, which, at that time, was cyclosporine A (CyA) (9.5%, n = 49) or omalizumab (2.1%, n = 11 (drug licensed 2014)) (Fig. S1). Omalizumab resulted in the best complete response compared with the other systemic treatments (Table SV). The remaining 22.9% were controlled with other treatments not recommended in the European guidelines such as 1st generation H1-antihistamines (9.9%) or other treatments (13.0%). Approximately 20% of all patients with CSU required short courses of oral corticosteroids.
The most frequent adverse events reported were somnolence (7.0%) and sedation (4.7%), mostly caused by high-dose 1st-generation H1-antihistamines. Muscle spasms and fatigue were observed in 5% of patients on CyA, but no severe renal impairment was recorded. This low rate of renal impairment could be explained by the low doses used and the short duration of treatments. No adverse effects were reported with omalizumab.
Patients were defined as refractory to a certain therapy based on the last drug registered in the medical records that forced a move to the next treatment line, as defined by EAACI/GA2LEN/WAO/EDF guidelines (1, 2). Refractoriness to treatment was analysed when 1st- and 2nd-generation H1 antihistamines were used in monotherapy or combined (Fig. 2). Most of the patients treated with licensed doses of 1st-generation H1-antihistamines were refractory to treatment (73/80, 91%). Some of the refractory patients (21/73, 28.8%) received 4-fold doses of 1st-generation H1-antihistamines, but 95% of them remained refractory. With 2nd-generation H1-antihistamines, the rates of refractoriness were lower. Even so, 78% of patients were refractory to licensed doses (332/427) and of those who received 4-fold 2nd-generation H1-antihistamine doses (181/332), 77% still had wheals and/or angioedema. No advantages were seen in treatment with a combination of 1st- and 2nd-generation H1-antihistamines.
Fig. 2. Refractoriness to 1st- and 2nd-generation H1-antihistamines. The patients refractory to 4-fold H1-antihistamine doses were previously refractory to licensed doses.
Multivariate analysis including 42 variables (Table SIII) was performed to assess factors potentially involved in refractoriness to any H1-antihistamine at any dose. Only baseline UAS7 appeared to be useful to predict refractoriness to H1-antihistamine. The mean baseline UAS7 was 15.1 ± 12.0 in well-controlled patients on first-line treatments, 21.8 ± 11.8 in patients controlled with second-line treatments, and 29.5 ± 11.1 in patients who required third-line treatments to achieve disease control (p < 0.0001). According to the UAS7, 84.6% of patients with a baseline UAS7 between 16 and 42 required cyclosporine or omalizumab to achieve symptom control, in contrast to 15.4% of patients with a baseline UAS7 between 0 and 15 (p = 0.0013) (Fig. 3).
Fig. 3. Chronic spontaneous urticaria (CSU) treatment ladder and relationship with the baseline Urticaria Activity Score 7 (UAS7), based on the EAACI/GA2LEN/WAO/EDF guideline. UAS7 = mean ± standard deviation (SD); UAS7 0–15: Well-controlled to mild urticaria activity; UAS7 16–42: moderate to severe urticaria activity.
CSU is not a rare disease, but there is often a significant delay in accurate diagnosis. In this analysis the time for patients to get specialized attendance was more than 4 years. This fact highlights the need to train general practitioners and emergency units in the initial identification and treatment of the disease, so that they can provide the correct information about the disease, and suggest complementary explorations and specialized management. A correct initial approach is crucial, because 5 years after disease onset at least 8.4% of patients with CSU (46/549) had experienced hives and itch, requiring healthcare. This data is in agreement with the percentage described by Gaig et al., which showed 11.3% of patients with CSU were symptomatic for more than 5 years (22). Even longer symptomatic periods have been described (4, 8, 23).
As described previously, all types of urticaria are more common in females than males (4, 22) . Some distinctive findings were helpful to define potential prognostic factors and establish a therapeutic plan. Although classically CSU occurs mostly at 20–40 years of age (24–28), in the current series the mean age of patients was higher (47.3 ± 16.2 years). Twenty-two percent of cases in our series were 65 years of age or older at the onset of CSU. CSU episodes were longer with worse prognosis when they started at or over the age of 45 years, requiring effective and safe treatments for a longer period.
Of the 549 patients with CSU, 19.2% had had more than one episode. This particular phenotype of patients prone to CSU has shorter episodes, but a longer duration of complete disease than patients who have a single episode of CSU.
These results suggest an underestimation of angioedema (16.2% of patients with CSU in the current study). This could be partially explained because this type of data was not recorded in their medical records. This finding is consistent with the results of the ASSURE study, in which angioedema was reported more frequently by patients than by physicians (28, 29). Nevertheless, in our series angioedema did not correlate with a worse prognosis in terms of high activity, longer duration or antihistamine refractoriness of the disease; however, these results should be interpreted with caution since the current sample size is very small (n = 83).
Concomitant subtypes of urticaria in CSU vary from 10% to 50% depending on the series (25–27, 30, 31). Of CSU-CIndU patients, 20.2% showed more active and longer episodes of CSU. CSU patients with CIndU were also the most frequently treated after 5 years of follow-up. Furthermore, they required higher doses of 2nd-generation H1-antihistamines to control the disease. This is consistent with Kozel et al. (25); in a series of 220 patients with CSU only 20.8% of patients with the CSU-CIndU subtype were symptom-free after 1 year of treatment compared with 47.4% of patients with is-CSU. Patients with CSU-CIndU showed a significantly lower number of episodes and longer periods with active disease compared with patients with is-CSU in the current study.
More than half of the patients in this series had a positive ASST result (14). Patients with positive ASST and positive CD63 expression showed significantly higher UAS7 (16), in concordance with previous studies (32, 33).
Some complementary exploratory tests need careful interpretation regarding their relationship with disease activity and prognosis. Serum levels of D-dimer tended to be high in patients with more active CSU refractory to anti H1-antihistamines, but the sample size makes this result inconclusive. Significantly high levels of sALP were found with no other associated diseases. A possible relationship between this observation and vitamin D deficiency can be hypothesized (34–36). Vitamin D has recently been suggested to play a role in the pathogenesis of more active and longer-lasting cases of CSU (37–39). However, no clear-cut relationship was found in our study between sALP levels and UAS7.
The use of a licenced dose of 2nd-generation H1-antihistamines and an increased dose is recommended in current urticaria guidelines (1, 2). Nevertheless, looking at data for the heterogeneous treatments prescribed prior to the baseline consultation in our department, it is clear that, in practice, the guidelines are not followed completely (1–3, 40). Although 1st-generation H1-antihistamines, and the combination of antihistamines, are no longer recommended (1, 2), almost 20% of patients were treated previously with this combination. These patients showed higher percentages of refractoriness to the treatment compared with patients treated with 2nd-generation H1-antihistamines, at licensed and increased doses. Thus, we agree with and support the European guidelines that 1st-generation H1-antihistamines and the combination of 1st- and 2nd-generation H1-antihistamines should not be used in treatment of CSU.
It is important to note that 77.7% of patients with CSU in our series were symptomatic despite the use of licensed doses of 2nd-generation H1-antihistamines. Although it has been reported that 63.2% of patients who are non-respondent to licensed doses of H1-antihistamines can benefit from increased doses, immunomodulation was required quite frequently in our series (41).
Baseline UAS7 has been shown to be the only parameter able to predict refractoriness to H1-antihistamines. Almost 90% of patients with CSU with a baseline UAS7 >16 needed CyA or omalizumab combined with antihistamines in order to control their symptoms.
Despite some limitations based on the retrospective and single-centre character of this study, we conclude that the following factors indicate the worst prognosis, in terms of duration and/or activity of the disease and its episodes: multiple episodes of CSU; late-onset; concomitant CIndU; and functional serum autoreactivity. We recommend the routine use of validated patient-reported outcomes, such as the UAS7, as this has a predictive therapeutic value that will be of use in daily clinical practice.
This paper is based on a research project supported by Novartis Grant. The authors thank Mariana Lacentra for work as data manager and Monica Giménez for assistance in drafting the manuscript.
Funding sources. Novartis grant.
Conflicts of interest. AMG-A is a medical advisor for Uriach Pharma, Genentech and Novartis. She has received research grants from Intendis-Bayer, Uriach Pharma and Novartis, and has participated in educational activities sponsored by Uriach Pharma, Novartis, Genentech, Menarini, Glaxo Smith & Kline, Merck MSD, Almirall and Leo Pharma. The other authors declare no conflicts of interests.


 Click to show fullsize
Click to show fullsize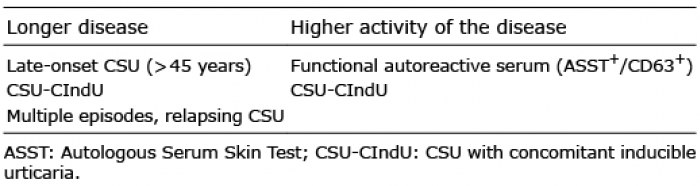 Click to show fullsize
Click to show fullsize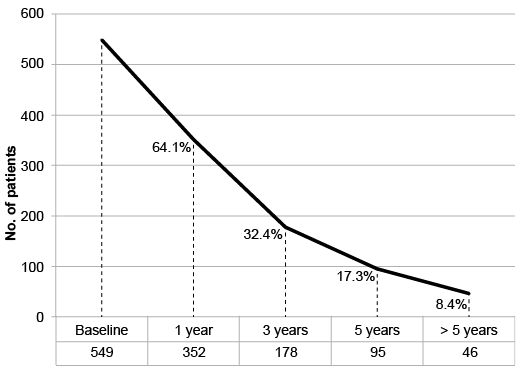 Click to show fullsize
Click to show fullsize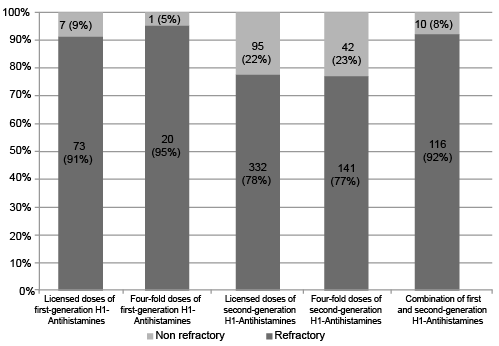 Click to show fullsize
Click to show fullsize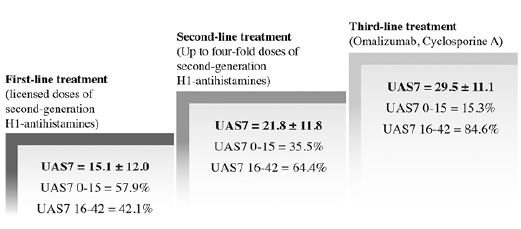 Click to show fullsize
Click to show fullsize