


1Department of Dermatology, Aarhus University Hospital, Aarhus, Denmark, 2Oslo Hudlegesenter, Oslo, Norway, 3Novartis Healthcare AB, Kemistvägen, Sweden, 4Novartis Norge AS, Oslo, Norway, 5Novartis Finland Oy, Espoo, Finland, 6Novartis Healthcare, Copenhagen, Denmark, and 7Department of Dermatology, Linköping University Hospital, Linköping, Sweden
Psoriasis is a stigmatizing chronic skin condition in which impairment of quality of life is associated with visibility of skin lesions, disease activity and severity. The ultimate goal of treatment is complete clearance of skin symptoms. The worldwide “Clear About Psoriasis” survey explored patients’ perspectives on clear/almost clear skin and the impact of psoriasis on daily life. We report here results from the Nordic countries (n = 609). Of respondents, 44% achieved clear/almost clear skin with their current treatment, of which 71% were comfortable discussing this expectation with their physician, compared with only 46% of patients who had not achieved clear/almost clear skin. Of patients who achieved clear/almost clear skin, 85% reported treatment satisfaction vs. 39% who had not. Psoriasis profoundly affected daily life, with 88% of respondents reporting discrimination/humiliation and 61% reporting an impact on their professional life. This report highlights stigmatization among Nordic patients with psoriasis and the potential to improve physician–patient communication.
Key words: psoriasis; clear skin; patient survey; Nordic countries.
Accepted Sep 23, 2018; Epub ahead of print Sep 24, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Rikke Dodge, Novartis Healthcare, DK-2300 Copenhagen, Denmark. E-mail: rikke.dodge@novartis.com
Psoriasis is a chronic, painful, disfiguring and disabling disease, currently without a cure. The disease can occur at any age, and at least 100 million people worldwide are affected, causing the WHO to consider psoriasis as a serious global problem. This article presents the Nordic results from the global patient survey “Clear About Psoriasis”, which was completed by 609 Nordic patients. This article illuminates the patients’ perspective on disease activity and how the disease affects their lives. It shows the importance of a well-defined treatment goal and good communication with healthcare professionals.
Psoriasis is a common inflammatory, immune-mediated disease that affects 2–4% of the population worldwide (1–3); higher prevalence rates have been reported in countries that are distant from the equator (e.g. in Northern Europe) compared with countries that are closer, due to environmental and genetic factors (4).
One of the key goals of psoriasis treatment is to achieve complete clearance of skin symptoms (5). Psoriasis Area and Severity Index (PASI) is the most commonly used metric to evaluate the extent of disease and lesions by their characteristics such as redness, thickness and scaliness (5, 6).
Traditional treatments for psoriasis, including topical medications and systemic therapy, are considered effective if they achieve ≥ 75% improvement in PASI (PASI 75) from baseline values (7). Biological therapies targeting the interleukin (IL)-17A or IL-23 pathways, or tumour necrosis factor-α, have demonstrated 90% improvement in skin lesions (i.e. PASI 90; clear/almost clear skin) in a significant proportion of patients (8–10). Results of a systematic review and meta-analysis suggest that patients who achieve clear/almost clear skin (i.e. PASI 90) may achieve improved quality of life (QoL) compared with patients who achieve lower PASI responses (11). PASI 90 has therefore gained wide recognition among dermatologists, who consider it the standard for optimal treatment efficacy (12).
The worldwide “Clear About Psoriasis” patient survey was conducted in more than 8,000 patients with moderate-to-severe psoriasis in order to understand patients’ views on clear/almost clear skin and how living with psoriasis affects their everyday life. Results from the global patient sample suggested that many patients with psoriasis are still not achieving clear/almost clear skin, and many are unaware that this might be possible (13).
This report explores the results of respondents from the Nordic countries (Denmark, Finland, Norway and Sweden) in order to understand if their perspectives regarding clear/almost clear skin and the impact of psoriasis are different from those of the global patient population.
The survey, sponsored by Novartis, was conducted in 31 countries worldwide. The findings for the Nordic countries (Denmark, Finland, Norway and Sweden) are presented in this report. The survey was translated into 32 languages, including Danish, Finnish, Norwegian and Swedish. A steering committee comprising medical experts, including dermatologists, general practitioners, and representatives of psoriasis patient advocacy organizations (the US National Psoriasis Foundation and the European Federation of Psoriasis Associations (EUROPSO)) advised on the selection of patient-reported outcome assessment tools to be used in the survey. Psoriasis patient advocacy organizations reviewed the survey to ensure ease of use and understanding; these included Psoriasisforeningen in Denmark, Psoriasisliitto in Finland, and Psoriasis - og eksemforbundet in Norway.
The survey was conducted primarily online, although some were completed as face-to-face interviews. It employed 4 validated scales that captured the impact of clear/almost clear skin on multiple aspects of disease, including skin lesions and health-related QoL, such as work productivity, sleep, and well-being. The multiple choice questions in the survey could be answered in approximately 20 min. No definition of clear skin was provided in the survey, and spontaneous feelings/perceptions were reported.
The assessment tools included the following:
Participants were recruited from Denmark, Finland, Norway and Sweden via online panels, as well as via national psoriasis patient organizations in Denmark, Norway and Finland. The survey was distributed by patient advocacy organizations via a number of different channels, including Twitter, Facebook and online/offline newsletters.
Study participants were aged ≥ 18 years with current plaque psoriasis that had been medically diagnosed by a general practitioner, dermatologist, rheumatologist, allergist, or other medical professional. Participants eligible for inclusion had moderate-to-severe psoriasis, as defined by the modified PASI criteria (i.e. SAPASI ≥ 10, a standard definition of moderate-to-severe psoriasis (17). An amendment to the inclusion criteria was made after approximately 40% of the enrolment target was reached. This amendment broadened the criteria to include a second patient group having SAPASI 5–9.9 with psoriasis affecting sensitive and/or prominent body parts: face, palms, hands, fingers, genitals, soles of feet, or nails). This broader definition acknowledged the potentially higher debilitating impact of psoriasis on such bodily locations (7) and was endorsed by a consensus of the expert dermatologists on the survey steering committee.
Respondents who currently had clear/almost clear skin under treatment were asked to retrospectively estimate the extent of their psoriasis at its worst, before the use of effective therapy. Participants were excluded from the survey if they had participated in an online survey about psoriasis in the preceding 4 weeks.
Ethics committee approval was not sought or required for this non-interventional study that invited members of the public to participate. Informed consent was obtained from patients at the beginning of the survey.
The survey was conducted between October 2015 and March 2016. A total of 398,230 patients was recruited to the global survey and directed to the landing page of the survey website. The survey was started by 154,000 patients, who were screened for eligibility during the first 19 questions. Of the screened sample, 8,338 met the eligibility criteria and participated in the survey. Among those patients who did not meet the eligibility criteria, most did not have plaque psoriasis or did not meet the PASI criteria.
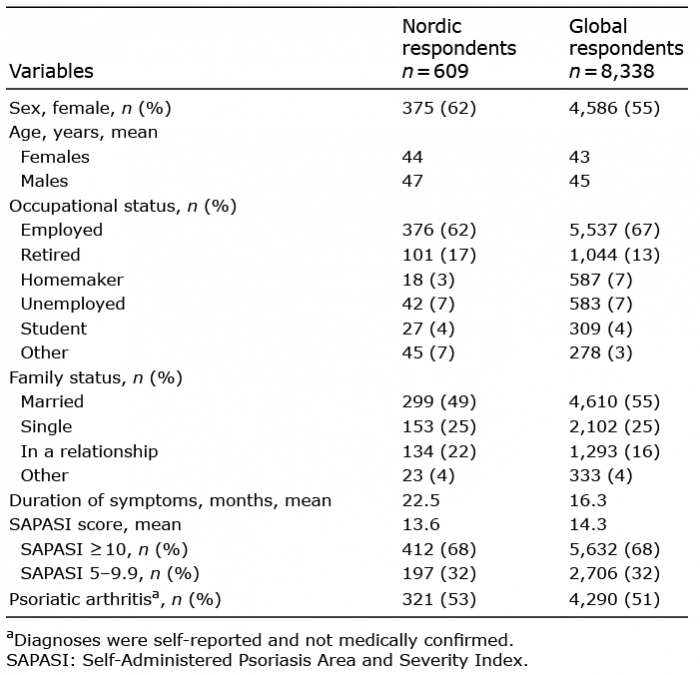
There were 609 completed responses in the Nordic countries, of which 91 were completed in Denmark, 227 in Finland, 221 in Norway and 70 in Sweden. The demographic and clinical characteristics of respondents were observed to be similar to those of the global population (Table I).
Table I. Respondent demographics and clinical characteristics
Feelings about clear skin and treatment. A total of 44% of respondents from the Nordic countries reported achieving clear/almost clear skin with their current treatment. Half of all of the Nordic respondents (52%) believed that achieving clear/almost clear skin was possible irrespective of their current status (patients who had achieved clear skin vs. those who did not). Of those patients who had achieved clear/almost clear skin, 50% believed that achieving clear/almost clear skin was possible before achieving it themselves, whereas this proportion was 53% among those who had not achieved clear/almost clear skin. A higher proportion of younger (aged 18–40 years) vs. older (aged ≥71 years) respondents believed that clear skin was achievable (Fig. 1).
Fig. 1. Proportion of Nordic respondents who believe that clear/almost clear skin is achievable (by age). Patients were asked if they thought it was achievable to have clear/almost clear skin (i.e. skin completely clear of psoriasis).
Many respondents (57%) felt comfortable speaking to their physician about wanting to achieve clear/almost clear skin, but 12% reported that they were not comfort-able having this discussion, and 31% had not spoken to their physician about wanting clear/almost clear skin. Among respondents who had achieved clear/almost clear skin, 71% were comfortable having a discussion with their physician, with 10% not comfortable having this discussion, and 19% who had not spoken to their physician about this objective. Among respondents who had not achieved clear/almost clear skin, 46% were comfortable having a discussion with their physician, with 13% not comfortable having this discussion, and 41% who had not spoken to their physician about wanting to achieve this outcome.
Almost two-thirds (59%) of all respondents were satisfied with their treatment; this included 85% of patients who had and 39% of patients who had not achieved clear/almost clear skin. The most important reasons for treatment satisfaction were reduced itching (50%), achievement of almost completely clear skin (38%) and fewer side-effects (33%). Not achieving clear skin was the major reason for dissatisfaction (62%), while 45% of dissatisfied respondents reported still experiencing pain and soreness.
Among all Nordic respondents, the top 3 goals of treatment among patients were reducing itching (39%), lessening the appearance of plaques (32%) and achieving clear/almost clear skin (29%; Fig. 2a). When analysed according to achievement of the clear/almost clear skin outcome, higher proportions of patients who had than who had not achieved clear/almost clear skin felt that maintaining/achieving clear/almost clear skin was important (Fig. 2b).
Among patients who achieved clear/almost clear skin, for 65% and 38% of patients, it took more than 1 year and more than 5 years, respectively, to be prescribed the treatment that resulted in clear/almost clear skin. Patients needed a mean of 4 different treatments and consulted 3 different medical professionals before achieving clear/almost clear skin.
Fig. 2. Main treatment goals of (a) all Nordic respondents and (b) Nordic respondents by achievement of clear/almost clear skin outcome. Patients were asked what treatment goal they agreed with their doctor.
In their everyday life, a large proportion (88%) of the Nordic respondents had experienced some form of discrimination or humiliation due to their disease across their personal and social life (Fig. 3a).
A total of 61% (63% with SAPASI scores 5–9.9 and 60% with SAPASI scores ≥ 10) felt that the disease affected their professional life, with the strongest impact (54%) attributed to skin flakes shed by respondents (Fig. 3b). In the previous 6 months, 35% of employed respondents (40% of women and 27% of men) reported taking at least one day off work because of their disease, while 8% took more than 14 days off (Fig. S1a). A higher proportion of patients who did than who did not achieve clear/almost clear skin (21.8% vs. 2.5%) reported taking 10–14 days off work because of their psoriasis (Fig. S1b).
Fig. 3. Effect of psoriasis on (a) everyday life and (b) work life for all Nordic respondents. aPatients were asked if they had ever experienced any of the following due to their psoriasis. bPatients were asked how psoriasis has impacted on their professional/working life.
Half of respondents (50%) felt unattractive because of their psoriasis, with many reporting feeling self-conscious (47%) and ashamed (36%) because of their skin condition (Fig. S2). Furthermore, 47% of respondents reported that their condition had affected past or current relationships, with as many as 37% avoiding having sex and 30% feeling inadequate as a spouse or partner (Fig. S3).
Patients reported spending a mean of 2.3 h a month online researching their condition, using a variety of media including online medical websites and health magazines, Google and Facebook groups (Fig. S4).
The Clear About Psoriasis patient survey was a worldwide survey that explored how psoriasis affected the lives of patients with psoriasis and assessed how patients felt about achieving clear/almost clear skin (13). As there are differences in clinical practice between countries and regions, this report sought to specifically explore the perceptions of patients from the Nordic countries.
The proportion achieving clear/almost clear skin with their current treatment was similar in the Nordic respondents compared with the respondents globally (44% and 43% (n = 8,338), respectively –) (13). Respondents from the Nordic countries appear to have higher expectations, with 52% of survey respondents in the Nordic countries believing that clear/almost clear skin was achievable, compared with 45% in the global study population.
Among those individuals who did and did not achieve clear/almost clear skin, the proportion who reported feeling comfortable talking to their physician about wanting to achieve clear/almost clear skin was 71% and 46% in the Nordic population of respondents, respectively, compared with 79% and 63%, respectively, in the global sample. These findings indicate that, despite the fact that individuals who do not achieve clear/almost clear skin have high expectations, these individuals do not feel comfortable talking to their clinician about their treatment goals. In addition, these findings, particularly among the Nordic patients who did not achieve clear/almost clear skin, suggest a lack of awareness of treatment options and achievable outcomes among psoriasis patients, a finding that has been highlighted previously (18). The patients may also be experiencing challenges in reaching a dermatologist, or a lack of consultation time in which the available treatment options can be discussed. Furthermore, previous studies have highlighted that patients’ perceptions of disease and treatment do not necessarily align with those of their physician (9, 10); this may, in part, explain why patients are uncomfortable having a discussion with their physician.
The patients who reported clear/almost clear skin were much more likely to be satisfied with their current treatment than those who did not report achieving clear/almost clear skin (85% vs 39%, respectively), a finding that also aligns with that of the global patient sample (83% vs 35%, respectively). The satisfaction rates among patients in this survey who achieved clear/almost clear skin are higher than those previously reported in a telephone survey conducted by Vaidya et al. (19), in which only 20% of the study population who met the criteria of “well-controlled” disease were satisfied with their current treatments. These findings indicate that psoriasis care is working well for those respondents from the Nordic countries who achieve clear/almost clear skin. Similar to the global survey, the main goal of treatment for Nordic patients was relief of itching (39% in Nordic patients vs. 42% globally). This is consistent with the findings from other international patient surveys (e.g. Multinational Assessment of Psoriasis and Psoriatic Arthritis) (20). However, when the data was analysed according to achievement of clear/almost clear skin, it was evident that achievement/maintenance of this outcome was a higher priority among patients who did than who did not achieve clear/almost clear skin.
Among patients who achieved clear/almost clear skin, 36% of Nordic patients received a treatment that lead to clear skin in less than one year, compared with only 28% of global patients. A substantial proportion (38%) of the Nordic patients had to wait more than 5 years to receive a treatment that lead to clear skin, while only 28% of global patients did. In both the Nordic and global samples, it was observed that, on average, patients needed 4 different treatments and consulted 3 different medical professionals before achieving clear/almost clear skin.
Discrimination or humiliation was reported by 88% of the Nordic respondents compared with 84% of global respondents. Almost half of the respondents (47%) felt that their psoriasis has influenced past or current relationships compared with 43% of the global sample, and psoriasis had a negative impact on participants’ capacity for intimacy. The latter finding aligns with results of a recently published European study that reported impairment of sexual well-being in patients with skin conditions (21). The emotional well-being of participants in the current survey was also affected by their condition, with negative feelings, such as unattractiveness and self-consciousness, being associated with psoriasis. A recent survey in patients with psoriasis demonstrated variability in the psychological health impact of psoriasis among patients from different European countries, with the lowest impact on anxiety and depression being observed in patients from Denmark (22).
Compared with the global sample (54%), a higher proportion (61%) of the Nordic sample felt that psoriasis affected their work life. A lower proportion of the Nordic than the global sample (36% vs. 41%, respectively) took at least one day off work in the previous 6 months because of their psoriasis. The finding that psoriasis imposes a significant burden on the daily lives of patients, including impacting their personal and professional relationship, is consistent with other research involving individuals with psoriasis (23–26). There were considerably more patients who did than who did not achieve clear/almost clear skin who had 10–14 days off work because of their psoriasis. The reasons for this difference are unclear and warrant further study.
This analysis had a number of limitations, including potential bias resulting from respondents’ self-selection and a relatively small sample size; therefore, the survey population may not provide a true reflection of the perspectives of all patients with psoriasis in the Nordic countries. It should also be noted that there was potential for inaccurate interpretation of questions. For instance, there were differences in the terminology used between the Nordic countries (e.g. “clear skin” has been translated as “clean skin” in Finnish), which may have influenced the results. Also, since treatment efficacy was self-reported, the patient understanding of clear/almost clear skin may not be aligned with the high level of improvement required for the clinical definition of this goal, i.e. a PASI 90 response. However, because the survey pertains to symptom-free skin, it is hoped that patients have interpreted the terminology as it was intended. Another limitation is that although the PASI is a validated scoring method with good reproducibility in trained individuals, it has a number of limitations, the most notable to this survey being that it can be difficult to interpret (27). Consequently, the patients’ scores may not necessarily correlate with those of experienced clinicians, and the patients’ understanding of clear/almost clear skin may not align with the clinical definition of this goal (i.e. PASI 90 response).
Despite these limitations, this report provides interesting findings regarding the prospect of achieving clear/almost clear skin that are specific to psoriasis patients in the Nordic countries. It highlights that Nordic patients with psoriasis feel stigmatized in their daily lives and that there is a potential need to improve communication between physicians and patients to ensure better alignment on treatment goals. Although a slightly higher proportion of respondents from the Nordic countries than their global counterparts reported satisfaction with their treatment, the proportion that were not satisfied is considerable and suggest that there is room for improvement in this area.
The Clear About Psoriasis study was sponsored by Novartis Pharma AG. The authors thank Aisling O’Keeffe, PhD of Novartis Ireland Ltd, Dublin, Ireland and Aafrin Khan, Novartis Healthcare Pvt. Ltd, Hyderabad, India for providing medical writing support, which was funded by Novartis Pharma AG in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Conflicts of interest and funding: CE: lecturer and has received consultancy/honoraria and/or research funding from Novartis, LEO Pharma and Amgen. ME: has served as consultant for Novartis. A-KD: Employee of Novartis Healthcare AB, Kemistvägen, Sweden. SJ: employee of Novartis Norge AS, Oslo, Norway. LF: employee of Novartis Finland Oy, Espoo, Finland. RD: employee of Novartis Healthcare A/S, Copenhagen, Denmark. MKR: has been a consultant or served on Advisory Boards with Janssen Cilag, Abbvie and Novartis, and has had paid consultancies and lectures from Abbvie, Eli Lilly, Novartis and LEO Pharma. He reports carrying out clinical trials for Eli Lilly.


 Click to show fullsize
Click to show fullsize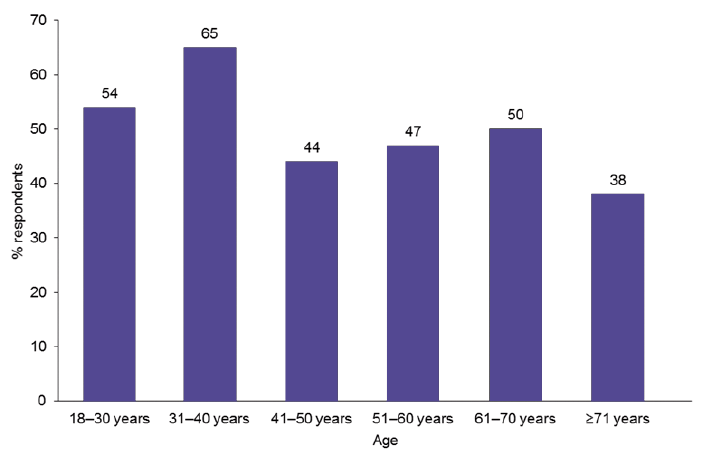 Click to show fullsize
Click to show fullsize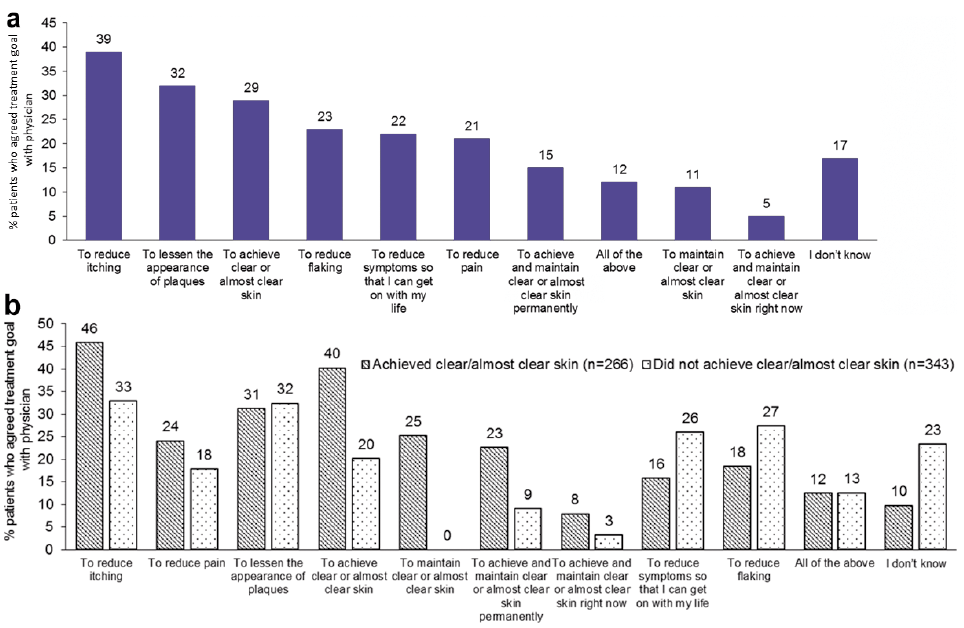 Click to show fullsize
Click to show fullsize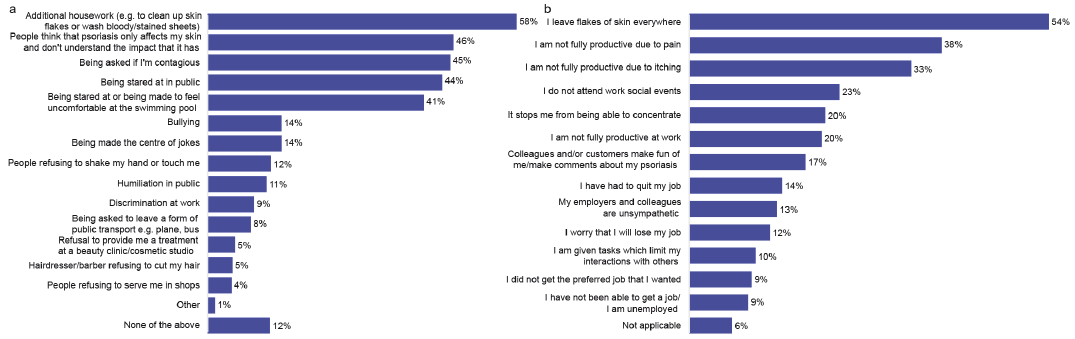 Click to show fullsize
Click to show fullsize