


1Institute for Environmental and Gender-Specific Medicine, Juntendo University Graduate School of Medicine, 2-1-1 Tomioka, Urayasu, Chiba 279-0021, 2Department of Gastroenterology, and 3Division of Clinical Laboratory, Juntendo University Urayasu Hospital, Chiba, Japan. *E-mail: ktakamor@juntendo.ac.jp
Accepted Feb 5, 2019; E-published Feb 6, 2019
Pruritus is a common comorbid symptom of chronic liver disease (CLD) and can reduce the quality of life. The pathogenesis of pruritus itself remains unclear, but includes the involvement of endogenous opioids (1). Previous studies have identified 3 major types of opioid receptors, μ-type (MOR, a receptor for β-endorphins), κ-type (KOR, a receptor for dynorphins), and δ-type (a receptor for enkephalins) (2). Activation of μ-opioid receptors is thought to induce pruritus, whereas activation of κ-opioid receptors is believed to have a suppressive effect (1, 3). We previously reported that the κ-opioid system was downregulated in the epidermis of patients with atopic dermatitis (AD) and that psoralen-ultraviolet A (PUVA) therapy downregulated the μ-opioid system and restored the κ-opioid system, concomitant with a decrease in visual analogue scale (VAS) score (4). Cholestasis increased plasma opioid levels in, both mice and humans (5, 6). In addition, the opioid antagonists, e.g. naloxone and naltrexone, have been extensively evaluated as the clinical treatment for patients with cholestasis-associated pruritus (7, 8). More recently, nalfurafine hydrochloride, a selective κ-opioid receptor agonist, was approved in Japan for the treatment of refractory pruritus in patients with CLD (3, 9). Despite many opioid peptide-opioid receptor treatments used clinically to alleviate pruritus in CLD, no studies to date have demonstrated any significant correlation between endogenous opioid levels and the presence or intensity of pruritus. This study therefore evaluated the concentrations of β-endorphin (μ-opioid) and dynorphin A (κ-opioid) and their correlations with pruritus in CLD patients.
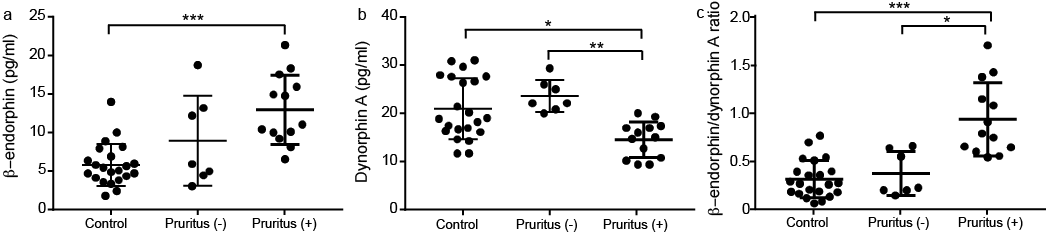
Clinical observations showed that, although pruritus occurs frequently in patients with CLD, some patients in the CLD group reported no symptoms of pruritus. The 20 CLD patients were divided into two groups, 13 with and 7 without pruritus. We then examined the endogenous opioid levels between the controls and CLD patients with or without pruritus. The CLD patients with pruritus showed plasma concentrations of β-endorphin and β-endorphin/dynorphin A ratio, which reflects the balance of endogenous opioids, to be significantly higher; while dynorphin A levels were significantly lower compared to the controls (Fig. 1). Importantly, a comparison of endogenous opioid levels showed that dynorphin A levels were significantly attenuated and β-endorphin/dynorphin A ratio significantly increased in CLD patients with pruritus than without. Notably, these levels were similar in the CLD patients without pruritus and the control group (Fig. 1b and c).
Fig. 1. Relationships of β-endorphin and dynorphin A concentrations and β-endorphin/dynorphin A ratios with pruritus in chronic liver disease (CLD) patients. Twenty patients with CLD were divided into those with (n = 13) and without (n = 7) pruritus and the concentrations of β-endorphin (a) and dynorphin A (b) and β-endorphin/dynorphin A ratios (c) were determined. *p < 0.05, **p < 0.01, ***p < 0.001.
Moreover, we examined the correlations among β-endorphin, dynorphin A, β-endorphin/dynorphin A ratio and VAS score. There was no correlation between β-endorphin level and VAS score (Fig. 2a). Meanwhile, dynorphin A level was negatively correlated and β-endorphin/dynorphin A ratio was positively correlated with the VAS score (Fig. 2b and c).
Fig. 2. Correlations of plasma β-endorphin, dynorphin A, and β-endorphin/dynorphin A ratio with VAS in chronic liver disease (CLD) patients. Scatterplots of correlations of (a) β-endorphin concentration, (b) dynorphin A concentration, (c) and β-endorphin/dynorphin A ratio with the VAS pruritus score in patients with CLD. p < 0.05 indicates statistical significance.
The present study showed that dynorphin A level and β-endorphin /dynorphin A ratio were consecutively attenuated and increased in plasma of CLD patients with pruritus compared to those without (Fig. 1), suggesting an imbalance of endogenous opioids in CLD patients with pruritus. In line with these findings, we discovered that dynorphin A concentrations and the β-endorphin/dynorphin A ratio correlated significantly with the VAS scores in CLD patients (Fig. 2b and c). These findings suggest that plasma levels of endogenous opioids, especially dynorphin A, may objectively reflect the pruritus intensity in CLD patients.
The endogenous opioid system has been shown to play a role in the mediation of pruritus of central origin (10) as well as in the periphery (4). Clinical and experimental evidences have suggested that liver may contribute to the alterations and enhancements in the opioid system in cholestasis. These findings suggest that, under pathologic conditions, the liver accumulates and excretes endogenous opioids (5, 6, 11). Alternatively, the availability of opioid peptides is increased in the periphery, facilitating the entrance of these peptides into the central nervous system (11). In addition, some endogenous opioids-processing enzyme activity was moderately detected in the liver (12), suggesting a possibility of a decreased plasma degradation of opioid peptides in liver disease under pathologic conditions. In line with these reports, we found that the CLD patients with pruritus, who exhibited alterations of β-endorphin/dynorphin A ratios, had more severe liver damage (significantly increased AST – aspartate transaminase, ALT – alanine transaminase, and total bilirubin, and higher GGT – gamma-glutamyl transferase levels), compared to the non-pruritus group (Table SI), although further studies are required to determine these correlations.
The present study reported that pruritus symptoms in CLD correlated with reduced dynorphin A plasma levels (Figs 1 and 2). Recently, dynorphin was shown to act as a neuromodulator, inhibiting pruritus in the dorsal horn of the spinal cord, probably, by directly inhibiting spinal interneurons that express gastrin-releasing peptide receptor (GRPR) or by targeting as-yet-unidentified interneurons or projection neurons that mediate itch (13). As the selective κ-opioid receptor agonists (3, 9) have been found clinically effective in relieving symptoms of pruritus in patients with liver disease, our data scientifically support the rationale for these treatments.
The present study has several limitations. The controls were sex-matched, but the age was lower than in the CLD patients. The number of samples in this study is relatively small and there is a different sex distribution between groups, hence a larger study with matched age and sex groups will be useful in the future. The CLD consists of different aetiologies, which may be a confounder for the levels of endogenous opioids and the pruritus intensity due to each specific pathological mechanism of the disease. Future studies may include patients with the same CLD to avoid possible disease-related confounders.
In conclusion, this study has shown that plasma dynorphin A level correlates with the severity of pruritus in patients with CLD and may reflect the degree of pruritus in CLD patients.
This work was partly supported by grants from the Strategic Research Foundation Grant-aided Project for Private Universities from MEXT (S1311011) and KAKENHI (17K16351).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize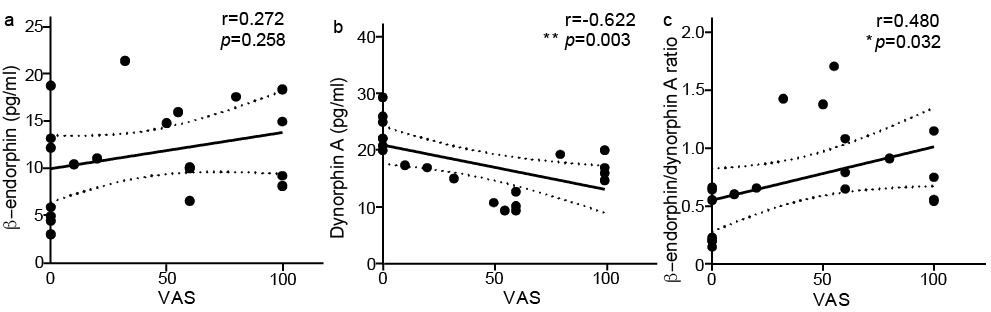 Click to show fullsize
Click to show fullsize