


Departments of 1Oncology, 2Pathology, and 3Dermatology, West China Hospital, Sichuan University, No. 37, Guo Xue Xiang, Chengdu, Sichuan, 610041, China. *E-mail: hxlcyxy@163.com
Accepted Feb 7, 2019; E-published Feb 8, 2019
Blastic plasmacytoid dendritic cell neoplasm (BPDCN) is a rare haematological tumour that may infiltrate multiple sites, of which the skin is the most common. However, the pathogenesis of BPDCN remains largely unclear. Here, we report next-generation sequencing analysis of a case of BPDCN.
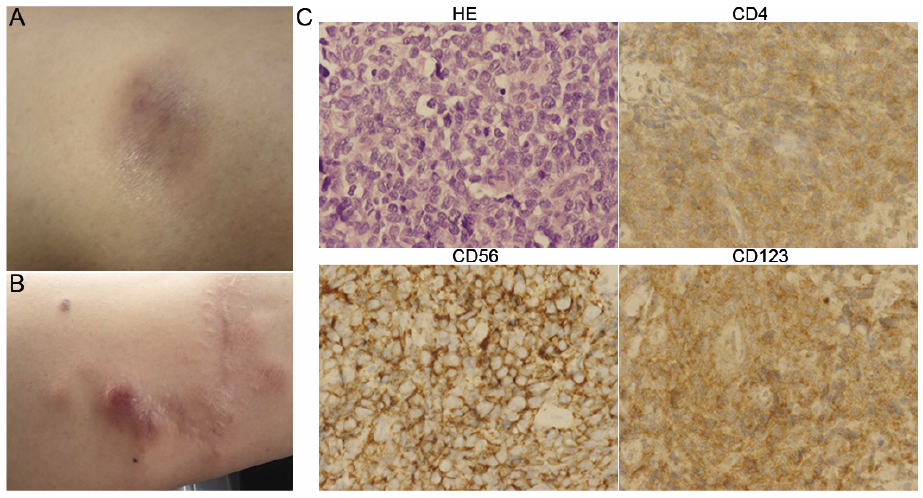
A 43-year-old man had experienced a honeybee sting on the left forearm, which was followed by a red rash, acute pain, swelling and local increased skin temperature; all symptoms were relieved by anti-inflammatory treatment. However, a small dark purple residual plaque with a size of 1.5 cm×1.8 cm remained (Fig. 1A), which was diagnosed as BPDCN by biopsy. The man presented no other symptoms, and peripheral blood tests were normal. Microscopic histology revealed a malignant neoplasm composed of blastoid differentiated tumour cells within the dermis, subcutaneously and in perivascular areas. Immunohistochemistry showed that the tumour cells were positive for CD4, CD56, and CD123 (Fig. 1C), supporting the diagnosis of BPDCN. Positron emission tomography-computed tomography (PET-CT) scan and bone marrow aspiration and biopsy revealed no other positive foci. After chemotherapy, the patient suffered disease relapsed with several new small subcutaneous nodules in the same area (left forearm) and the ipsilateral elbow fossa were found new lesions (Fig. 2); the largest size of skin nodule was 0.5 cm × 0.7 cm (Fig. 1B), which was confirmed as disease relapsed via re-biopsy. We chose 6 cycles of P-GEMOX (L-asparaginase, gemcitabine, oxaliplatin) plus dexamethasone, and local skin radiotherapy resulted in complete remission. Nonetheless, after only 6 months, progression was found in the skin, lymph node and bone marrow, and the patient is now receiving chemotherapy, which appears to be ineffective. To investigate the genetic aberration in this case, we performed deep sequencing of the patient’s two skin samples, targeting exon sequencing of a 413-gene panel of haematological malignancies (Table I), with oral mucosal cells as a germline control. The results showed the same mutation in the ALK and NOTCH1 genes in the primary and relapsed skin lesion sites.
Fig. 1. Clinical and pathological presentation of the lesion skin in blastic plasmacytoid dendritic cell neoplasm. A shows the primary skin lesion on the left arm. B depicts the relapse of the disease in the same area. C displays the morphology and immunohistochemistry staining of a skin biopsy sample. HE, CD4, CD56, and CD123 staining are shown (100×).
Fig. 2. PET-CT features of BPDCN. A and B is the negative control of C and D. C showed the disease’s relapse of the left forearm skin, D showed the lymph node involved in the ipsilateral elbow fossa.
Table I. Gene mutations identified by next-generation sequencing
There are currently no clues regarding the aetiology of BPDCN, and the pathogenesis also remains largely unknown. Alterations in some NOTCH pathway genes and abnormal activation of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) signalling have been indicated as having possible roles in tumour development (1, 2). However, none of the hotspot mutations reported for BPDCN were found in our patient. We did find 3.6-fold amplification of the TCL1A gene in the present patient’s primary skin lesion sample; this gene encodes a plasmacytoid dendritic cell-associated antigen expressed in 99% of BPDCN patients (3). In addition, by binding to and activating the cyclin-dependent kinases CDK4 and CDK6, CCND3, which was amplified 2.6-fold in the primary sample, promotes cell cycle progression from G1 to S phase (4). Furthermore, overexpression of DAXX, which was amplified 3.3-fold in the primary skin lesion sample, serves a caspase-dependent proapoptotic role in neoplastic lymphocytes (5, 6). In previous reports, HES6 and RUNX2 involved in Notch signalling were found to be more highly expressed in BPDCN than in normal pDC (2). In contrast, mutations in NOTCH1 genes have not yet been reported. In our case, such mutations were found in the both primary and relapsed skin lesion tissues, suggesting that Notch signalling plays a role in the pathogenesis of BPDCN.
In conclusion, to the best of our knowledge, this is the first report of a BPDCN case after a honeybee sting. DNA sequencing assisted us in determining the highly genetically heterogeneous nature of BPDCN.
The patient’s participation, cooperation, and devotion are highly appreciated by the research group, and his authorization for the publication of this report was obtained.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize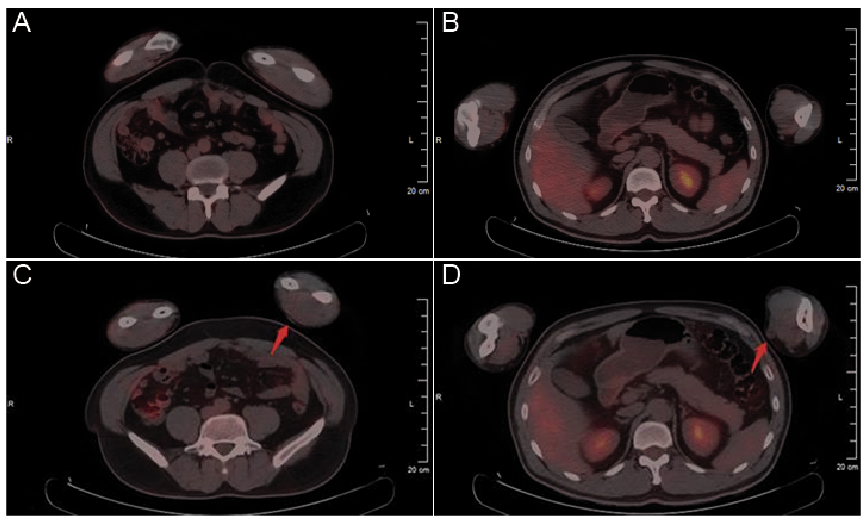 Click to show fullsize
Click to show fullsize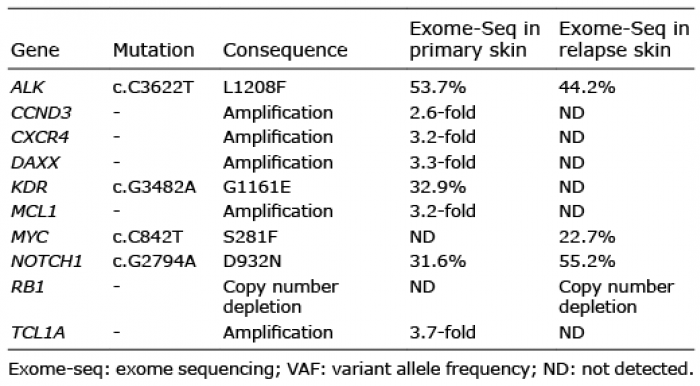 Click to show fullsize
Click to show fullsize