


Departments of 1Dermatology, 2Pathology, and 3Human Genetics, Hadassah-Hebrew University Medical Center, Kiryat Hadassah, POB 12000, Jerusalem, 9112001, Israel. *E-mail: Rverem@hadassah.org.il
A 20-month-old boy was brought for examination due to numerous ulcers over his upper trunk, of 6 months duration. He was a single child to first-degree cousins of Arab Palestinian descent. The parents denied any trauma preceding the appearance of the ulcers. Treatment with emollients, topical corticosteroids and topical antibiotics had not resulted in clinical improvement. The child had history of neonatal stridor and chronic hoarseness, but was otherwise healthy. Fiber optic laryngoscopy did not reveal any structural abnormalities in the vocal cords or larynx.
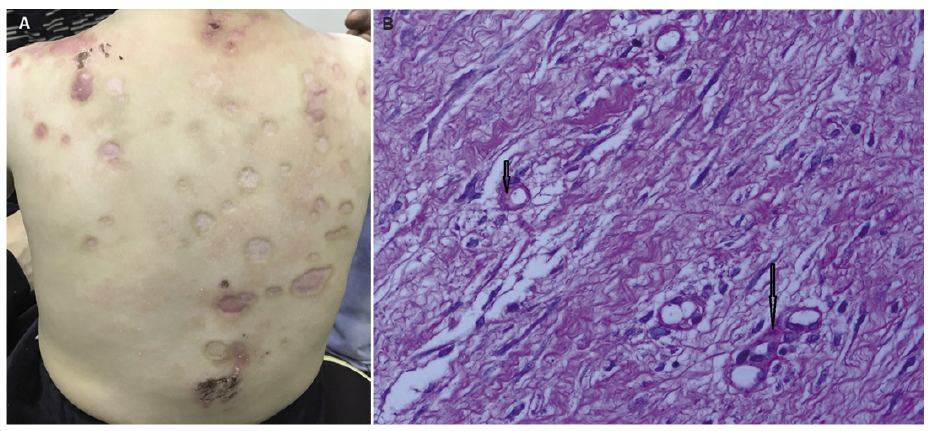
Physical examination revealed numerous symmetrically distributed, round-oval, punched-out ulcers, as well as depressed erythematous and skin-coloured scars on the mid- and upper back, shoulders and thorax (Fig. 1A). Thin hair and dry skin were also noted. A 3-mm punch biopsy was obtained from a lesion on the left shoulder.
Histopathological evaluation demonstrated a hypertrophic scar, composed mainly of fibroblasts and myofibroblasts (which stained positively for actin), as well as a Periodic acid–Schiff (PAS)-positive hyaline thickening of a capillary wall in the superficial dermis (Fig. 1B).
What is your diagnosis? See next page for answer.
Fig. 1. (A) Multiple symmetrically distributed, round-oval, depressed scars on the back of a 20-month-old boy. (B) Histopathological examination of a skin biopsy specimen (haematoxylin-eosin, original magnification ×600) showing Periodic acid–Schiff (PAS)-positive hyaline material around small blood vessels (arrows) in the superficial dermis.
Acta Derm Venereol 2019; XX: XX–XX.
Diagnosis: Lipoid proteinosis
Lipoid proteinosis is a rare, autosomal recessive disorder, characterized by skin and mucous membrane scarring with deposition of hyaline (1, 2). The disease has a very early onset, usually manifesting in early infancy with hoarseness and vocal cord thickening. During childhood, the skin is highly prone to damage by minor trauma or friction, which can cause blisters and varicelliform or acneiform scars. With time, dermal infiltration may manifest as grouped warty plaques on the dorsal aspect of the hands and elbows. Beaded eyelid papules are typical. Mucosal involvement is characterized by infiltration of the larynx, leading to hoarseness, and infiltration of the tongue and its frenulum, limiting lingual movements and causing speech difficulties (3).
The disease can also involve internal organs and the central nervous system, in the form of calcified spots in the temporal lobes or in the regions of the hippocampus and the amygdala. Epileptic seizures and psychiatric abnormalities may occur (4).
Lipoid proteinosis is characterized histologically by deposits of PAS-positive, diastase-resistant, homogenous, hyaline-like, material in the dermo–epidermal junction and in the dermis. This pale eosinophilic material is initially localized around blood vessels, eccrine sweat glands and pilosebaceous units. With time, the deposits around blood vessels develop an “onion-skin” appearance. There is also progressive atrophy of sweat glands associated with increasing hyaline deposition (5, 6).
The disorder has been shown to result from biallelic mutations in the extracellular matrix protein 1 (ECM1) gene (4). ECM1 is a secreted glycoprotein that binds to perlecan, the major heparan sulphate proteoglycan of the basement membrane, as well as to growth factors and fibrillar proteins. It is thought to act as a dermal biological glue regulating basement membrane and interstitial collagen fibril macro-assembly and growth factor binding (7). Loss of functioning ECM1 in the dermis negatively affects dermal homeostasis, leading to skin infiltration and scarring (8).
The prognosis of lipoid proteinosis is relatively good, despite the progressive nature of the disease until early adulthood (3).
Further investigation in our patient, revealed that 3 of the mother’s nephews had chronic hoarseness and scarred facial skin. Their clinical and genetic evaluations have been reported previously (1). Genetic analysis of DNA extracted from the patient’s peripheral blood revealed a homozygous missense splice-site mutation in the ECM1 gene (IVS1 + 1G–>C), identical to that identified years ago in the mother’s nephews.
To the best of our knowledge, the patient presented in our case is the youngest patient with lipoid proteinosis with histological confirmation to be reported to date. Spontaneous skin ulceration with infantile hoarseness are highly suspicious for lipoid proteinosis. It should be noted that the histopathological findings of the disease at such a young age are delicate and subtle, therefore, the dermopathologist should be alert for these findings when there is a high degree of clinical suspicion.


 Click to show fullsize
Click to show fullsize