


1Reference Centre of Rare Skin Diseases, Larrey Hospital, Paul Sabatier University, Toulouse, 2Department of Paediatric Dermatology, Bordeaux, Departments of Dermatology: 3Timone Hospital, Marseille, 5Hôtel-Dieu Hospital, Nantes, 6Saint-Vincent-de-Paul Hospital, Lille, 7CHU Nice University Hospital, Nice, 8Fréjus Hospital, Fréjus, 9Argenteuil Hospital, Argenteuil, 10CH de Pontoise University Hospital, Pontoise, 13CHU de Rouen University Hospital, Rouen and 14CHU Rennes University Hospital, Rennes, 4Department of Paediatric Nephrology, Rheumatology & Dermatology, Femme-Mère-Enfant Hospital, Lyon, RAISE referee centre, Lyon, Departments of Paediatric Dermatology, 11Robert-Debré Hospital, Paris and 12Necker-Enfants Malades Hospital, Paris, and 15Department of Paediatric Rheumatology, Bicêtre Hospital, AP-HP, University Paris Sud, Le Kremlin-Bicêtre, France
Methotrexate has demonstrated its efficiency for the treatment of juvenile localized scleroderma but some patients may be resistant. The aim of our study was to define the profile of such patients. We performed an observational retrospective multicenter study between 2007 and 2016 and included all children seen in the French Paediatric Dermatology and Rheumatology departments with active localized scleroderma treated by methotrexate for a minimum of 4 months. Metho-trexate efficacy was assessed clinically and/or by imaging between the fourth to twelfth months of treatment. A total of 57 patients were included. Metho-trexate dosage ranged from 7 to 15 mg/m2/week. Only 4 patients were resistant. No common features could be identified between these 4 patients. Children with localized scleroderma are rarely resistant to metho-trexate and we did not identify a clinical profile for those resistant patients.
Key words: localized scleroderma; morphoea; scleroderma; treatment; methotrexate.
Accepted Feb 26, 2019; E-published Feb 27, 2019
Acta Derm Venereol
Corr: Dr. Juliette Hardy, Reference Centre of Rare Skin Diseases, Larrey Hospital, Paul Sabatier University, FR-31400 Toulouse, France. E-mail: juliette.marie.hardy@gmail.com
Morphea is a rare skin condition due, in part, to an unusual reaction of the immune system. Disease generally affects the outermost layers of the skin which becomes hard and thickened. In severe cases underlying tissue and bones can be affected resulting in functional disabilities. Metho-trexate in association with systemic corticosteroids are the most frequent drugs prescribed for severe form of the disease. However some patient will not respond to these treatments. The aim of our study was to better define the clinical profile of these resistant patients in order to help clinicians in their therapeutic choice.
Localised scleroderma (LS) or morphoea, is a connective tissue disorder of unknown aetiology characterised by fibrosis of the skin and subcutaneous tissues (1). It is a rare disease more commonly affecting children than adults. The annual incidence rate in childhood is estimated at 1 to 2.7 per 100,000 individuals (2). Juvenile LS has been classified by Laxer & Zulian into 5 subtypes (3): linear involving the torso, limbs (most commonly) or the head (“en coup de sabre” and Parry–Romberg syndrome); plaque-type; generalised; disabling pansclerotic mor-phoea; and mixed morphoea. Early lesions commonly present as erythematous patches that evolve into sclerotic plaques. Parry–Romberg syndrome is characterised by hemifacial atrophy involving the subcutis and bone with mobile overlying skin without sclerosis. In contrast to systemic sclerosis, LS is considered a benign disease but can be complicated by joint contractures and limitations, limb length discrepancy and deformities. Neurological (4) (epilepsy, migraine, neuralgia and/or paraesthesia of cranial nerves) and ophthalmological (adnexa abnormalities, uveitis, episcleritis) (5) anomalies may be associated with LS localised to the head. LS usually last for several years, sometimes up to 20 years, with long stretches of quiescence interrupted by unpredictable reactivations (6). Disease activity is difficult to evaluate because of a lack of specific biomarkers. Imaging is performed in some centres. Doppler ultrasound may identify areas of increased blood flow related to inflammation (7). Magnetic resonance imaging reveals a thickening of the dermis and infiltration of the subcutaneous fatty tissue with an increased signal intensity (8). Assessment Tool (LoSCAT) and Computerized Skin Score (CSS) have also been proposed for disease activity monitoring as well as imaging techniques such infrared thermography (IRT), laser doppler flowmeter and, more recently, Cone Beam Computed Tomography (CBCT) (9–11).
Many topical and systemic therapies have been reported in the literature for juvenile LS, with variable efficiency (12). A few randomised controlled studies are available and management of LS depends, in clinical practice, on the standards of care at the time of diagnosis, the severity of the disease, its location, the extent of the lesions, and the physician’s experience (13).
The effectiveness of methotrexate (MTX), in association with systemic corticosteroids (CS) upon initiation, has been reported in 11 studies (4 uncontrolled prospective and 7 retrospective with 7 to 88 children) and in a unique randomized, double-blind, controlled trial of 46 children (4, 9, 14–23). Martini et al. published the largest study to date, describing both clinical course and long-term outcome of 126 children with JLS. Among their patients, 88 were treated with MTX (23). Nevertheless, none of these studies have focused on MTX’s resistance. Little is known about the frequency of such resistance and the clinical features of these non-responder patients. The aim of our study was to better define the clinical profile of these patients in order to help clinicians in their therapeutic choice.
We performed a retrospective multicentre observational study including all children (< 18 years) with active LS treated by MTX for a minimum of 4 months, seen between May 2007 and January 2016 in the French paediatric dermatology and rheumatology departments. A total of 25 departments were contacted with the help of the French Group of Paediatric Dermatology (SDFP) and the French-speaking paediatric rheumatology society (SOFREMIP). Clinical subtypes of LS were based on Laxer and Zulian’s classification (3). LS was considered active in cases of inflammatory lesions, occurrence of new lesions or an increase in size of pre-existing lesions. LS was considered severe in cases of deep sclerosis, extensive disease (> 50% of body surface area (BSA)) or ulcerations. Data was collected from medical records and photographs, using a standardised questionnaire. Evolution was assessed clinically and by imaging for some children (MRI and/or ultrasounds) between the 4th and 12th months of treatment. Evolution was classified into 3 categories: improvement (decrease in size of the initial lesions and/or skin softening without new lesions or enlargement of pre-existing lesions), stability (absence of new lesions, no enlargement of pre-existing lesions), or resistance (enlarging or worsening of pre-existing lesions or new lesions).
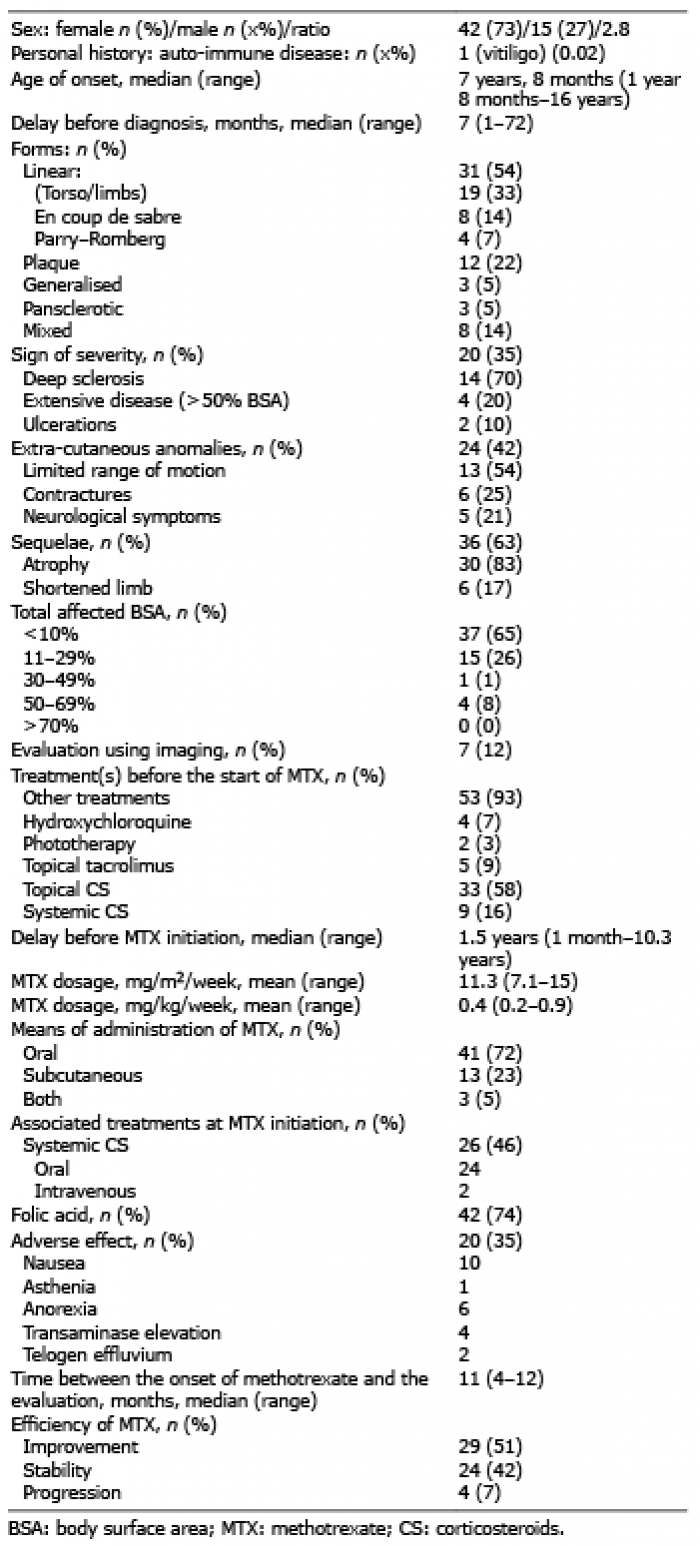
Sixty-one patients were included from 16 centres, among which 57 for whom complete data could be analysed. Their characteristics are shown in Table I. Most of them were female (n = 42; 73%). Only one had a personal history of auto-immune disease (vitiligo). The age of onset was variable and may be very early, before the age of 2 years. The delay in diagnosis was also variable, but ranged up to 6 years. Linear morphoea was the most common form, especially involving the torso and limbs (24). Approximately one third of the patients had a severe disease, mainly related to deep sclerosis. Half of the patients had extra-cutaneous manifestations, of which limited range of motion was the most common anomaly.
Table I. Characteristics of the 57 patients with juvenile localized scleroderma (LS)
Almost all patients (n = 53; 93%) had been administered another treatment before starting MTX: topical CS or systemic CS for 33 (58%) and 9 (16%) of them, respectively. The duration of the disease upon MTX initiation varied from 1 month to over 10 years, with a median duration of 1.5 years. MTX dosage ranged from 7.1 to 15 mg/m2/week (mean dosage of 11.3). Nearly half were given oral corticosteroids (1 mg/kg/day) upon MTX initiation, for a median duration of 3 months (range: 1–18 months). Two patients were administered intravenous CS (1 g daily given during 3 consecutive days every month for 3 months). Twenty patients (35%) suffered adverse events, with none being serious, and the most frequent being nausea.
At evaluation, performed at a median time of 11 months after MTX initiation, 29 (51%) of the 57 patients improved, 24 (42%) remained stable and 4 (7%) were resistant. Responses according to clinical form are reported in Table II and the characteristics of the 4 patients resistant to MTX are detailed in Table III.
No common features could be identified in particular, as each patient had a different form of LS (Parry–Romberg, disabling pansclerotic, plaque, and mixed mor-phoea). None were affected by linear morphoea.
Regarding the outcomes of our 4 patients, the child with pansclerotic morphoea suffered a fatal outcome (24), one was treated with mycophenolate (with no efficacy), another was given ciclosporin (with no efficacy) and the last one was lost to follow-up.
Table II. Responses of the 57 children to methotrexate, according to the clinical form
Table III. Characteristics of the 4 patients resistant to methotrexate (MTX)
Fig. 1. The 4 patients resistant to methotrexate A: Patient (1) with pansclerotic morphoea. B: Patient (2) with plaque morphoea. C1 and C2: Patient (3) with mixed morphoea (plaque and linear morphoea). D: Patient (4) with Parry-Romberg morphoea.
We present here the first study focused on the drug’s resistance. This study reveals that resistance to MTX is a rare event but does seem to be related to a particular profile.
The multicentric nature of the study and therefore the heterogeneity of treatment schemes and modalities of patients’ evaluation represent the main limitations of our study. This study also included patients from expert centres where the most severe patients are more likely to be referred.
Comparison with other studies is difficult, due to the different treatment schemes and outcome measurements. Nevertheless, the low percentage of resistance to MTX was similar to those previously reported in the literature (6 to 10% vs. 7% in our study) (9, 14–17,19). This reinforces the fact that MTX is indeed recommended as first-choice therapy for active LS.
There is other data on MTX resistance in the literature. Martini et al. reported 10 children treated by mycophenolate mofetil because of a LS considered active, despite therapy with MTX (25). None displayed any particular clinical features. In the randomised, double-blind, placebo-controlled trial by Zulian (9), 3 out of 46 patients in the MTX group (6.5%) developed new lesions during treatment, but their clinical characteristics were not detailed. In the retrospective series of 34 patients by Weibel et al. (17), active disease during MTX therapy was significantly associated with a younger age at the onset of the disease.
The interesting finding of our study was the absence of resistance for torso or limb linear morphoea, en coup de sabre morphoea, and the generalised form. Therefore, these 3 forms could be better responders than other forms.
In adult LS, in the retrospective cohort of 107 patients by Mertens et al. (26), patients with more severe subtypes (i.e. linear and deep subtypes) and a longer delay in MTX initiation were 2 situations presenting a significantly higher risk of treatment failure.
The reasons for resistance to MTX are unknown. One hypothesis could be insufficient dosage. The Childhood Arthritis and Rheumatology Research Alliance (CARRA) published a consensus treatment plan for juvenile LS in 2012 (27). This consensus recommends the use of MTX at a dosage of 1 mg/kg/week (up to 25 mg), alone or in association with CS. This dosage is notably higher than the mean dosage administered to our patients (0.4 or 0.5 mg/kg/week or 11 mg/m2/week for our resistant patients, 15 mg/m2 as a maximum) or in other studies in children (15 mg/m2/week, 20 mg as a maximum in the prospective study by Zulian (9)). The influence of MTX dosage on the outcomes of the disease was not demonstrated in children but in adults suffering from inflammatory diseases such as rheumatoid arthritis (28). We can suggest that there are pharmacokinetic variations between individuals. It was demonstrated that MTX blood levels are variable and largely unpredictable, even if the renal and hepatic functions are normal. Yokooji et al. (29) found that a variation in intestinal luminal pH and the involvement of multiple transporters in MTX absorption may cause variations in oral bioavailability among patients. Thus, the dosage should be adjusted individually, but such measurements are not available in clinical practice. The absence of an adequate course of corticosteroids in 3 out of 4 resistant patients may also be a cause for resistance to MTX.
Even if the delay for introducing MTX was not demonstrated to be associated with more resistance, it seems reasonable to advise starting MTX as soon as possible in order to avoid irreversible sequelae.
In conclusion, children with LS are rarely resistant to MTX and we did not identify a clinical profile for those resistant patients. Further prospective studies assessing MTX (in particular at higher dosages) and other systemic agents in juvenile LS are necessary.


 Click to show fullsize
Click to show fullsize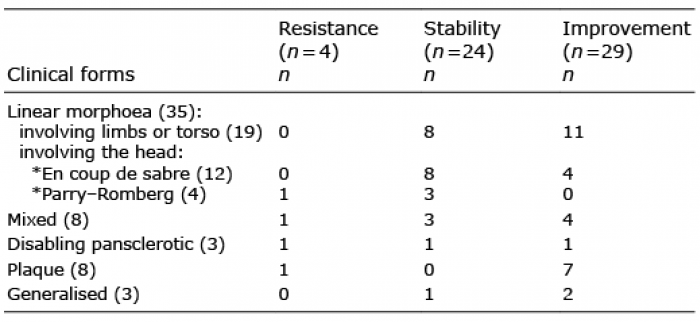 Click to show fullsize
Click to show fullsize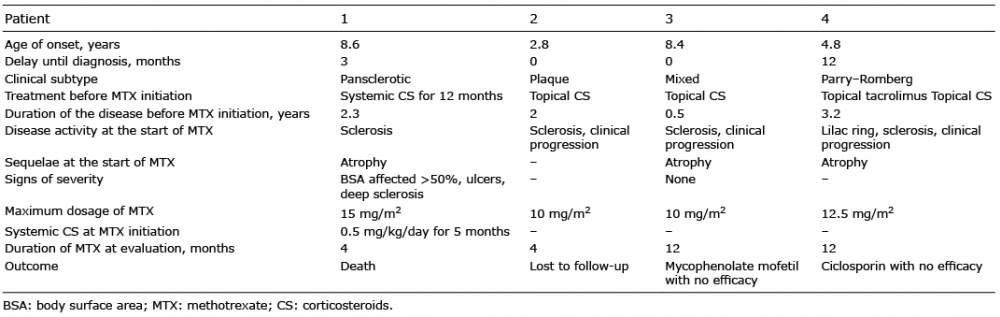 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize