


1Dr. Phillip Frost Department of Dermatology and Cutaneous Surgery, and 2Miami Itch Center, University of Miami Miller School of Medicine, Miami, USA
For decades, antihistamines have been the mainstay of treatment for chronic pruritus, yet they often only work by making patients drowsy and forgetful of their itch. A new era of antipruritic drugs is quickly approaching, presenting more effective treatments for patients suffering from chronic itch. Several treatments have been developed targeting specific receptors in the nervous system, such as the transient receptor potential channels, sodium channels, neurokinin-1 receptors, opioid receptors, and many more. Additionally, antipruritic therapies developed to work on the immune system have become more targeted, leading to greater safety and efficacy measures. These include crisaborole, several interleukin antagonists, and janus kinase inhibitors. The promising results presented with these new antipruritic therapies allow physicians to be better equipped to treat their itchy patients.
Key words: pruritus; antipruritics; cytokines; unmyelinated nerve fibers.
Accepted Oct 15, 2019; Published Jan 9, 2020
Acta Derm Venereol 2020; 100: adv00027.
Corr: Gil Yosipovitch, Dr. Phillip Frost Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine, 1600 NW 10th Ave, RMSB 2067B, Miami, FL 33136, USA. E-mail: gyosipovitch@med.miami.edu
Itch is a pesky sensation that can be difficult to eliminate. Although a mainstay of anti-itch therapy for many decades, antihistamines are not an effective therapy for patients with chronic, unrelenting itch. With a greater understanding of itch, newer treatments have been developed that are much more effective. These include drugs targeting the neural system and drugs that affect the immune system.
Chronic itch can negatively impact sleep, mood, and quality of life (1), causing patients to become desperate for relief. For decades, clinicians have resorted to antihistamines as a primary treatment for itch. However, the majority of chronic pruritus cases do not respond to antihistamines. In fact, they are not at all effective, and only make patients drowsy, forgetting that they are itchy.
With a more profound understanding of the patho-physiology of itch, newer and better targets for treatment have arisen. Medications working on the nerves, such as gabapentin and pregabalin, have improved symptoms, especially in cases of neuropathic itch such as brachioradial pruritus and notalgia paresthetica. Likewise, cases of inflammatory itch, such as psoriasis and recently atopic dermatitis (AD), have been dramatically improved by the advent of immunomodulating therapies.
New treatments for itch are continuously being developed. Herein, we will first discuss new antipruritic therapies working on the nervous system, and next we will discuss the antipruritic therapies targeting the immune system.
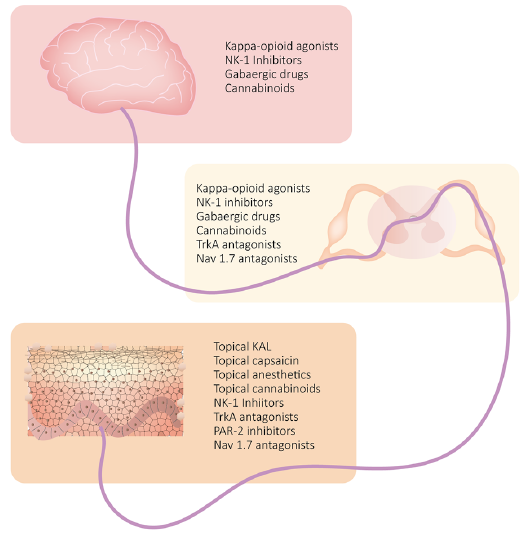
The sensation of itch is transmitted by unmyelinated C nerve fibers originating in the skin, synapsing in the spinal cord, and traversing the spinothalamic tract to the thalamus, before being further projected to various areas in the brain (2). Yet, the sensation of itch is not that simple. At the levels of the skin, spinal cord, and brain is an additional mechanism referred to as neural sensitization. This phenomenon causes the itch-selective neurons to become hypersensitive to pruritic stimuli (2). In the skin, neuronal sensitization is the result of inflammation, abnormal epidermal innervation, and dysfunction of cutaneous touch receptors. Dysfunction and attenuation of the inhibitory spinal circuits lead to neural sensitization at the level of the spinal cord. Finally, in the brain, chronic pruritus can lead to functional and structural changes in brain connectivity and activation, causing neural sensitization (2–4).
At each step of this pathway is an array of receptors involved in transmitting this pesky symptom. Discovery of the involvement of these receptors and their ligands in itch has led to development of novel targeted therapies. Fig. 1 diagrams where these antipruritic drugs targeting the nerves act in the skin, spinal cord, and brain.
Fig. 1. Site of action of new antipruritic drugs targeting the neural system. NK-1: meurokinin-1; TrkA: tropomyosin receptor kinase A; PAR-2: protease-activated receptor-2; KAL: ketamine-amitriptyline-lidocaine; Nav1.7: voltage-gated sodium channel 1.7.
Neurokinin-1 inhibitors
Neurokinin-1 (NK-1) serves as a receptor for substance P (SP), a known pruritic mediator. NK-1 is located throughout the central nervous system and skin. Activation of NK-1 by SP leads to pro-inflammatory cytokine production and mast cell release of pruritic mediators such as histamine, tumor necrosis factor (TNF)-α, prostaglandin D2, and leukotriene B4 (5).
Aprepitant, an NK-1 inhibitor originally developed to treat chemotherapy-induced nausea, is effective for treatment-refractory pruritus, as well as prurigo nodularis and cutaneous T-cell lymphoma (5, 6). Unfortunately, aprepitant is expensive and has a multitude of potential drug interactions, making it difficult to administer to patients (2, 7)
Serlopitant and tradipitant, newer NK-1 inhibitors, may be better alternatives and are currently being assessed in clinical trials (Table I). In randomized, placebo-controlled, phase II clinical trials, serlopitant exhibited a statistically significant decrease in pruritus in patients with treatment-refractory itch as well as prurigo nodularis (8, 9). In patients with AD, tradipitant showed a statistically significant decrease in itch in a randomized, placebo-controlled, phase II trial (10).
Table I. New antipruritic drugs targeting the neural system with corresponding ongoing clinical trials
Opioids
Opioids are classically thought of as highly effective pain medications, but more recently, opioids have also been shown to play a significant role in the treatment of pruritus. µ-, κ-, and δ-opioid receptors exist throughout the central and peripheral nervous systems, including the peripheral nerve fibers in the skin (11). In the spinal cord, imbalance in the activation status of µ- and κ-opioid receptors result in neuronal sensitization, which can lead to chronic itch (2). Similarly, an imbalance can occur in the periphery, for example a decrease in the expression of κ-opioid receptors seen in the epidermis of patients with AD (12).
µ- and κ-opioid receptors have been well-studied as they relate to pruritus, while the role of δ-opioid receptors in itch remains poorly understood (11). Specifically, µ-opioid antagonists and κ-opioid agonists are effective in treating itch.
Mixed µ-opioid antagonists and κ-opioid agonists. Butorphanol, both a µ-opioid antagonist and κ-opioid agonist, treats pruritus of varying etiologies with high efficacy. It is administered intranasally and has a rapid onset of action. Most importantly, it has little abuse potential (13). Butorphanol presents a great treatment option especially in cases of refractory chronic itch. However, its mode of intranasal administration is not something that dermatologists feel comfortable to use.
More recent developments are similar drugs like nalbuphine, a mixed µ-opioid antagonist and κ-opioid agonist. Clinical trials measuring its efficacy in treating uremic pruritus and prurigo nodularis have shown encouraging results (Table I) (14, 15).
Κ-opioid agonists. Nalfurafine, a κ-opioid agonist available in Japan, is an effective antipruritic agent in patients with uremic pruritus (16). In the United States, no κ-opioid agonists have yet been approved by the U.S. Food and Drug Administration (FDA) for the treatment of pruritus; however, clinical trials are underway. In a phase II clinical trial (17), intravenous (IV) CR845, a κ-opioid agonist, had significant antipruritic effects for pruritus associated with end-stage chronic kidney disease. Specifically, patients receiving CR845 three times a week after dialysis had a 68% greater reduction from baseline in worst itch scores compared to those receiving placebo (17). Clinical trials evaluating use of CR845 in other pruritic conditions are currently underway (Table I).
Asimadoline, a κ-opioid agonist originally developed for irritable bowel syndrome, completed phase II trials for pruritus associated with AD, but results have not yet been published (18). Likewise, SHR0410 and MR13A9 are undergoing phase I and II clinical trials, respectively, for treatment of pruritus in hemodialysis patients.
Tropomysin receptor kinase A antagonists
Epidermal keratinocytes and eosinophils release nerve growth factor (NGF), which binds to its receptor, tropomyosin receptor kinase A (TrkA). This leads to neural sensitization of transient receptor potential vanilloid 1 (TRPV1) and increased nerve sensitivity to SP, calcitonin gene-related peptide (CGRP), and brain-derived neurotrophic factor. Furthermore, NGF causes sensitization of the skin to nonhistaminergic cowhage-induced itch. Together, the TrkA-NGF pathway leads to hypersensitivity of peripheral sensory nerves to pruritic stimuli, and therefore presents a compelling target for antipruritic treatment (2).
In a phase IIb clinical trial of patients with psoriasis, CT327, a topical TrkA antagonist, demonstrated a statistically significant reduction in pruritus (19). Another Phase IIb trial with the same TrkA antagonist (SNA-120) also showed a robust reduction of pruritus, with 58% of patients receiving a meaningful itch reduction of 4.3 in Numerical Rating Scale (NRS). However, the vehicle also had significant anti-pruritic effects with 53% of patients receiving reduction in their itch, and the difference was not statistically significant (20).
Protease activated receptor-2 inhibitors
Protease-activated receptor-2 (PAR-2) is a type of G-protein coupled receptor activated by proteolytic cleavage of its extracellular N-terminus. For example, cowhage, the well-known inducer of nonhistaminergic itch, contains the protease mucunian, which activates PAR-2, as well as PAR-4, causing pruritus. Several other proteases can similarly activate PAR-2, causing symptoms of itch and making it a good target for treatment (2).
PZ-235, a pepducin that inhibits PAR-2, showed efficacy in the reduction of itching behaviors in a mouse model of AD (21). In humans, a one-time application of a different topical PAR-2 inhibitor led to a significant reduction in ratings of cowhage-induced itch intensities in a placebo-controlled study (22). Randomized, placebo-controlled clinical trials are warranted to determine whether the efficacy of PAR-2 inhibitors in treatment of various chronic itch conditions.
Interestingly, doxycycline, an antibiotic, has shown antipruritic properties in the treatment of acne vulgaris. In addition to its ability to reduce inflammation, its antipruritic mechanism is most likely due to its attenuation of the PAR-2 interleukin (IL)-8 pathway (23).
GABAergic drugs
Gabapentin and pregabalin, analogs of γ-aminobutyric acid (GABA) (an inhibitory neurotransmitter), have proven effective in treating various types of neuropathic itch (24). More specific GABAergic drugs are currently in development. In mice, targeting inhibitory α2 and α3 GABAA receptors reduced acute histaminergic and non-histaminergic pruritus. Furthermore, this α2/α3 GABAA modulator reduced chronic pruritus in a mouse model of AD and in dogs who were sensitized to house dust mites (25). Most importantly, these antipruritic effects seemed to come without any unwanted adverse effects (25).
Nav 1.7
An antibody inhibiting voltage-gated sodium channel (Nav) 1.7 with high selectivity suppressed chronic and acute itch in mice (26). This study indicated that Nav 1.7 is in fact involved in both histamine-dependent and -independent pruritus, and modulates spinal cord synaptic transmission for both itch and pain (26). Currently, Nav 1.7 antagonists are still in clinical development. Neu-P12, a Nav 1.7 antagonist, is currently being studied in phase I clinical trials for neuropathic pain (27), and will be interesting to see if it has an effect on itch.
The immune system plays an important role in itch, especially in inflammatory pruritic conditions. Classically, systemic immunosuppressive agents, such as glucocorticoids, methotrexate, cyclosporine, and azathioprine were the most effective therapeutic agents available, and although still often used as first-line treatment, can come with some potentially serious adverse effects.
Recently developed immunosuppressive treatments have a more specified mechanism of action, producing a higher level of efficacy and safety. Moreover, the era of biologic therapies is still ongoing and vastly expanding to include various itchy skin conditions, with clinical trials steadily underway (Table II) (28).
Table II. New antipruritic drugs targeting the immune system with corresponding ongoing clinical trials
Phosphodiesterase-4 inhibitors
Crisaborole is a topical non-steroidal phosphodiesterase-4 (PDE4) inhibitor approved for the treatment of moderate-to-severe AD. Applied as an ointment, crisaborole has proven to be effective in rapidly reducing pruritus in these patients. Pruritus relief was observed in significantly more patients receiving crisaborole ointment than vehicle in a post hoc analysis of two phase III clinical trials (29). This study showed that this rapid anti-pruritic effect was seen as early as day 2, and that 20% of patients receiving crisaborole experienced complete relief of their pruritus by day 6 (29).
Furthermore, a significant and strong link has been seen between pruritus and dermatology-specific quality of life scores. In a post hoc analysis of two phase III clinical trials, as patients’ itch improved with the help of crisaborole, so did their quality of life scores (30).
Similarly, improved quality of life scores and greater reductions in pruritus as measured by a visual analogue scale (VAS) were achieved in patients with plaque psoriasis receiving apremilast, an oral PDE4 inhibitor (31). The efficacy of apremilast as an antipruritic therapy in patients with scalp psoriasis is currently being studied in phase IV trials (Table II).
Interleukin antagonists
Interleukins (IL) are cytokines which help mediate immune responses and inflammation. Cytokines can act on a number of different targets including immune cells, keratinocytes, and even sensory nerves (Fig. 2) (32). Some of the newer cytokines used as targets in regard to treating itch are discussed below and include IL-4, IL-13, IL-31, and IL-17.
Fig. 2. Effect of interleukin (IL) antagonists on sensory nerves in the skin. OSMR: oncostatin M receptor.
IL-4. Dupilumab is a monoclonal antibody targeting the α subunit of the IL-4 receptor, blocking the signaling of cytokines IL-4 and IL-13, key cytokines involved in T-helper (Th) 2 immunity. Dupilumab has revolutionized the treatment of AD, significantly improving clinical symptoms of AD, rapidly reducing itch, and improving patients’ quality of life (33, 34).
Currently, the use of dupilumab in other pruritic conditions is of great interest. Case reports have shown that dupilumab can be helpful in the treatment of patients with prurigo nodularis (35–37), uremic pruritus (38), and bullous pemphigoid (39). However, randomized, placebo-controlled trials are necessary to evaluate its true efficacy in other pruritic conditions. Clinical trials assessing its efficacy in chronic spontaneous urticaria and cholinergic urticaria are currently underway (Table II).
Similar to dupilumab, pitrakinra also targets the IL-4 receptor α subunit, inhibiting IL-4 and IL-13 signaling (40). Pitrakinra has mostly been studied in the treatment of asthma (41). Subcutaneous administration of pitrakinra in moderate to severe AD was investigated in a phase II clinical trial, however results have not been published (40, 42).
IL-13. This cytokine produced by Th2 lymphocytes, is implicated in the pathway of AD. Development of therapies targeting this cytokine are of great interest in treating AD. Two biologic drugs targeting IL-13 that are under investigation for treatment of AD include lebrikizumab and tralokinumab.
Lebrikizumab targets soluble IL-13 and binds with high affinity, preventing binding to the IL-4 receptor α subunit and subsequent signaling (28, 43). In a phase II randomized, placebo-controlled trial (43), patients receiving lebrikizumab in combination with topical corticosteroids showed a significantly greater achievement of 50% reduction in eczema area and severity (EASI) score when compared to placebo. As for pruritus, mean percent reductions in baseline itch as assessed by VAS were not statistically significant when compared to placebo in this study (43). However, in a phase IIb study, lebrikizumab showed dose-dependent improvements in pruritus as early as day two, continuing until day 16 (44).
Tralokinumab potently binds to IL-13, prohibiting its binding to IL-13 receptor subunit α-1 and IL-13 receptor subunit α-2, neutralizing its effects (45). Results from a phase II study have indicated promising results for patients with moderate to severe AD treated with tralokinumab (46). At a dose of 300 mg administered subcutaneously every other week, patients received clinically significant improvements in EASI score, Scoring of Atopic Dermatitis (SCORAD), and the Dermatology Life Quality Index (DLQI). Additionally, a significant decrease in pruritus assessed by NRS was seen in patients treated with tralokizumab compared to placebo (46). Phase III trials are currently underway (Table II).
IL-31. This cytokine is heavily implicated in the patho-physiology of chronic pruritus. Increased levels of IL-31 have been associated with a variety of itchy conditions such as AD, prurigo nodularis, cutaneous T-cell lym-phoma, mastocytosis, chronic spontaneous urticaria, and bullous pemphigoid, making it a desirable pharmacological target for treatment of these patients (4, 47).
Nemolizumab, the first drug developed to inhibit IL-31 signaling, works by binding to IL-31 receptor A, which is located on a variety of cells including neurons, keratinocytes, macrophages, dendritic cells, and basophils (48). Thus far, nemolizumab has only been studied as a treatment for AD and prurigo nodularis. Pruritus was significantly improved in patients with moderate to severe AD in a phase II, randomized, double-blind, placebo-controlled clinical trial (49). As for prurigo nodularis, a phase II trial was recently completed with positive results (50).
BMS-981164, a monoclonal antibody targeting circulating IL-31, has completed a phase I clinical trial in AD, but no results have been published to date (51).
KPL-716, a monoclonal antibody against oncostatin M receptor beta (OSMR-beta), interferes with IL-31 and oncostatin M (OSM) signaling and has shown an antipruritic effect in patients with AD (52). A phase II clinical trial is currently recruiting patients with prurigo nodularis to assess the efficacy of KPL-716 in reducing their itch (53). Additionally, a pilot phase II study is assessing the efficacy of KPL-716 in reducing pruritus associated with chronic idiopathic urticaria, lichen planus lichen simplex chronicus, plaque psoriasis, and chronic idiopathic pruritus (Table II) (54).
IL-17. This is a pro-inflammatory cytokine that is primarily produced by Th17 cells, along with neutrophils and possibly mast cells. Keratinocytes are stimulated by IL-17A to secrete other pro-inflammatory mediators, which recruit neutrophils, Th17 cells, dendritic cells, and lymphoid cells (55). Drugs in this category are currently FDA-approved for the treatment of plaque psoriasis, and based on current studies, have shown the largest magnitude of effect in reducing psoriatic itch (5).
Secukinumab is a monoclonal antibody that selectively binds and neutralizes IL-17A (55). Two phase III, double-blind clinical trials assessing the efficacy of secukinumab in psoriasis showed that secukinumab was significantly more effective in reducing itch compared to placebo and etanercept, a TNF-α inhibitor (55, 56). In fact, in a pooled analysis of these two phase III trials, patients taking secukinumab achieved a significantly greater reduction in itching as early as the second week of treatment, demonstrating its rapid effect (57).
Phase II clinical trials assessing the role of secukinumab in treating AD are currently ongoing (Table II) (58, 59).
Ixekizumab is a high affinity monoclonal antibody also targeting IL-17A. Ixekizumab has proven to be effective in treating psoriasis, especially psoriatic itch in which phase III trials showed rapid, significant improvements. As early as the first week of treatment with ixekizumab, a significantly greater percentage of patients receiving the drug reported improvement of pruritus compared to those receiving etanercept or placebo (60).
In a long-term extension study of this trial, patients receiving ixekizumab maintained improvements in itch severity through the end of the study. By week 60, 48.2% of patients receiving ixekizumab every 4 weeks through-out the study achieved an itch NRS of 0. Similarly, after being switched to ixekizumab at 12 weeks, 45.1% and 45.3% of patients originally receiving placebo or etanercept, respectively, achieved an NRS of 0 at week 60 (61).
Additionally, ixekizumab is also effective in rapidly reducing genital pruritus. In a phase III, randomized, double-blind, placebo-controlled trial, a greater percentage of patients with genital psoriasis receiving ixekizumab achieved a significantly greater clinically meaningful itch reduction (greater than or equal to 3 point reduction on a numerical rating sale) than patients receiving placebo (59.7% versus 8.3%, p < 0.001) (62). Furthermore, a significant improvement in genital itch was seen as early as week 2 in those treated with ixekizumab (62).
Janus kinase inhibitors
Pruritus induced by cytokines is mediated at least partially by the janus kinase (JAK)/signal transducer and activation of transcription (STAT) pathway (2). JAK inhibitors block the JAK/ STAT pathway, which mediates signal transduction of cytokines and growth factors. When ligands bind to their receptors, JAKs are activated which lead to phosphorylation of STATs, which enter the cell nucleus to regulate transcription of target genes (63).
JAK inhibitors are commonly used in the treatment of inflammatory conditions such as rheumatoid arthritis. More recently, these medications are being investigated for use in chronic inflammatory skin conditions, such as AD and psoriasis (Table II).
Tofacitinib, an oral JAK inhibitor, works by blocking JAK1 and JAK3. It has been investigated for the treat-ment of psoriasis, with results from two randomized phase III trials showing that tofacitinib improved itch in patients with psoriasis, as soon as one day after treatment initiation (64, 65). Patients receiving tofacitinib also achieved a significant improvement in health-related quality of life, which were maintained through the end of the study at week 52 (64). Topical tofacitinib has also been effective for treating pruritus in both patients with psoriasis as well as AD (66, 67).
In a mouse model of psoriasis, tofacitinib significantly decreased mRNA expression of itchy cytokines IL-22, IL-23, and IL-31. This study also demonstrated that tofacitinib increased peptidergic epidermal nerve fiber density, which may aid in rescuing inhibitory itch mechanisms, proposing a novel mechanism for itch reduction by tofacitinib (68).
Additionally, JAK inhibitors may show promise in treating other cases of itch, even non-inflammatory causes of pruritus. In five patients with refractory, chronic idiopathic pruritus, oral tofacitinib led to marked improvement in their itch after only one month (69).
Baricitinib selectively inhibits JAK1 and JAK2. In a phase II, double-blind, randomized trial, baricitinib significantly improved AD and resulted in decreased pruritus (70). Phase III studies are currently underway (Table II).
Upadacitinib is a newer JAK inhibitor whose mechanism of action is selective for JAK1. In a phase II, randomized, placebo-controlled trial, upadacitinib significantly decreased ratings of itch in patients with AD (71). Phase III trials measuring the efficacy of upadacitinib in AD are currently in progress (Table II) (72).
Abrocitinib, another JAK inhibitor specifically targeting JAK1, has demonstrated excellent results in the treatment of AD. In a phase III randomized, double-blind, placebo-controlled trial, a statistically significant greater proportion of patients taking abrocitinib achieved a 4 point or larger reduction in itch NRS versus those taking placebo. Likewise, patients taking abrocitinib achieved a statistically significantly greater magnitude of decrease in the Pruritus and Symptoms Assessment for Atopic Dermatitis (PSAAD) compared to patients receiving placebo (73).
Histamine-4 receptor antagonists
Antihistamines, most of which are antagonists to the histamine-1 receptor, are often given to patients endorsing itch despite no clear evidence of their effectiveness as antipruritic therapies. Antihistamines specifically targeting the histamine-4 receptor (H4R), however, have shown some promise in treating itch (74). In a mouse model of AD, pretreatment with an H4R antagonist attenuated scratching responses in a dose-dependent manner (75).
ZPL389, an oral H4R antagonist, is currently being studied as a treatment for AD (Table II). However, results from a phase II randomized, double-blind, placebo-controlled study did not show a significant difference in pruritus reduction between patients taking ZPL389 and those receiving placebo (76).
Anti-IgE
A monoclonal anti-IgE antibody, ligelizumab, is undergoing phase III clinical trials to investigate its efficacy in treating chronic spontaneous urticaria (Table II). Studies have shown that ligelizumab has a much higher affinity to bind IgE in comparison to omalizumab (77), and thus it will be interesting to see its effect on pruritus in these patients.
New therapies for itch are continuously being developed. A new era of antipruritic drugs targeting specific neural receptors, itchy cytokines, and small molecules is swiftly approaching. Now that the pathophysiology of pruritus is better understood and research into new targets and mechanisms is perpetually underway, discovery and development of newer and better treatments for itch is ongoing. Unfortunately, treatment for chronic itch is not always simple and every patient requires individualized therapy. With education and development of new targets, clinicians can obtain a greater arsenal of treatment for their patients, to successfully treat them and improve their quality of life.
GY has been a consultant or Ad Board member of AbbVie, Kiniska, Menlo, TREVI, Sienna, Galderma, Sanofi, Regeneron, Novartis, Eli Lilly, Pfizer, Bayer, Cerave and received research grants from Sun Pharma, Pfizer, Leo, Kiniska, and Menlo.


 Click to show fullsize
Click to show fullsize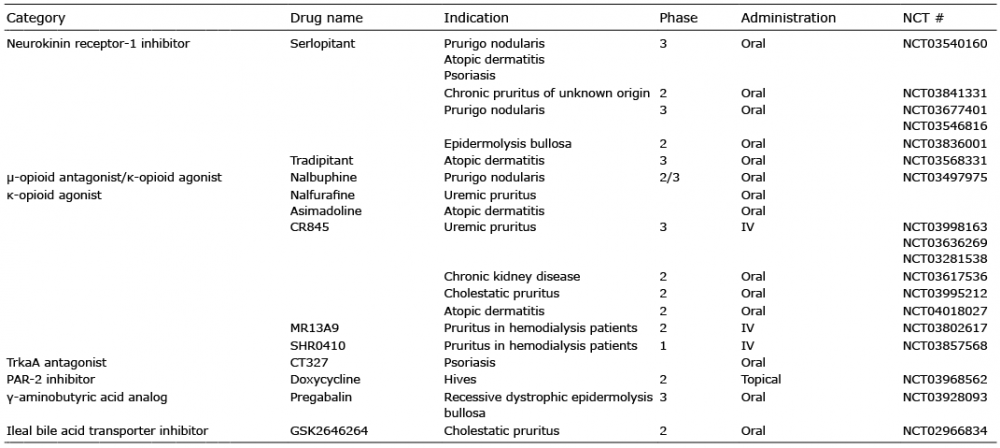 Click to show fullsize
Click to show fullsize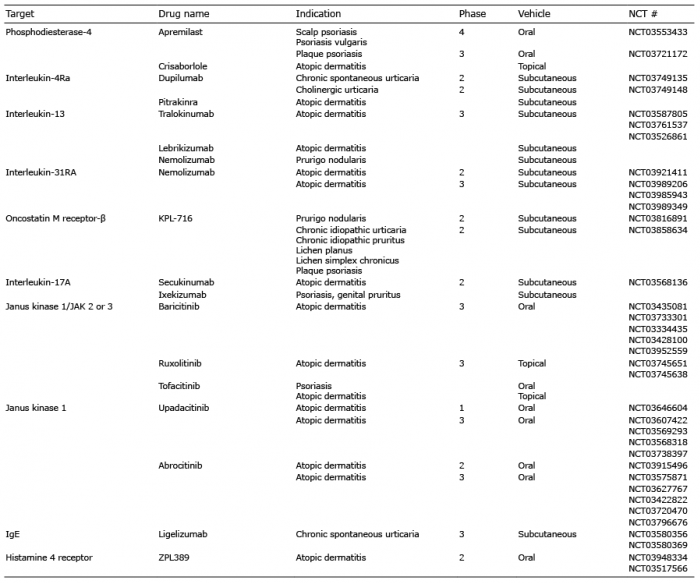 Click to show fullsize
Click to show fullsize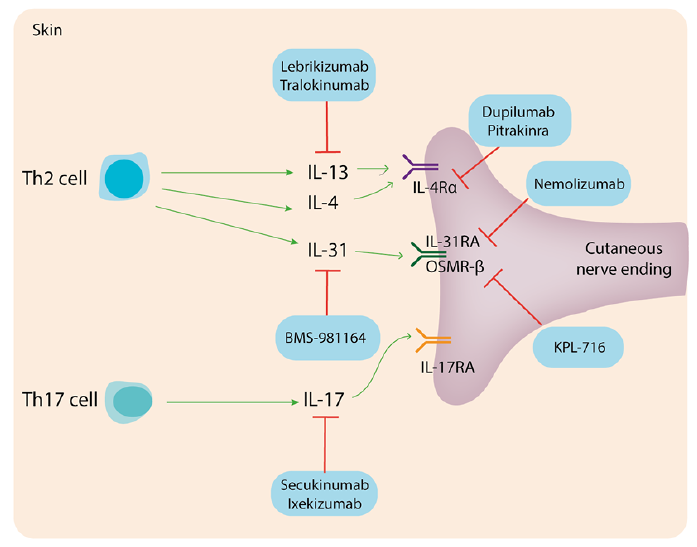 Click to show fullsize
Click to show fullsize