


1Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, 2Institute of Medical Informatics, University of Münster, Münster, 3Faculty of Health, University Witten/Herdecke, and 4Department of Dermatology and Allergy, School of Medicine, Technical University of Munich, Munich, Germany
Chronic pruritus is a frequent global condition. The pathophysiology, underlying aetiology, clinical manifestation, associated burden and response to therapy of chronic pruritus varies from patient to patient, making clinical research and management of this condition challenging. There are still several unmet needs, such as the need to standardize translational research protocols, diagnostic and therapeutic procedures and to enhance the knowledge of the humanistic and economic burden associated with chronic pruritus. Basic and clinical research is of the utmost importance to target these matters. Clinical research has the potential to identify new relevant mechanisms in affected patients, which may lead to identification of novel therapy targets. This article discusses in depth current shortcomings in the daily care of patients with chronic pruritus and the challenges clinical researchers and physicians treating chronic pruritus face in addressing these matters.
Key words: itch; patient-reported outcome; guideline; clinical trials; clinical research.
Accepted Oct 15, 2019; Published Jan 9, 2020
Acta Derm Venereol 2020; 100: adv00028.
Corr: Sonja Ständer, Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: Sonja.Staender@ukmuenster.de
Itch lasting for 6 weeks or more is considered chronic and represents a high burden for those affected. Various aspects of chronic itch, including the underlying origin of the itch, symptoms, skin manifestations, response to therapies and impairment of quality of life vary from patient to patient, constituting a challenge for clinicians and clinical researchers. Unmet needs, such as the standardization of experimental and clinical research protocols, diagnostic procedures and therapeutic regimens, as well as a better understanding of associated burdens and the development of novel effective therapies should be targeted by physicians and researchers dealing with chronic itch.
Chronic pruritus (CP), defined as pruritus lasting for 6 weeks or longer, is highly prevalent, affecting approximately one-sixth of the population in Germany (1). Population-based analyses of the nationwide search volume of pruritus on Google suggest an even larger number of individuals suffering from CP within Germany and the USA (2–4). Those affected often report a substantial burden and a relevant impairment of their quality of life (QoL) (5, 6). The aetiology, clinical manifestation, diagnostic measures and therapeutic response to CP vary from patient to patient, which contributes to the challenging management of CP (7). Although recent years have witnessed a marked increase in basic and clinical research efforts in this field, CP researchers and physicians treating CP currently face several challenges when targeting unmet needs that impact on clinical routine. The aim of this review is to highlight and discuss methodologies used in CP research, as well as current challenges and unmet needs in clinical care.
CP is a heterogeneous condition in terms of demogra-phics, clinical presentation and underlying origin. Al-though the prevalence of CP increases with age, patients of all age groups, including children, may be affected (8). Moreover, patients of both sexes and all ethnic backgrounds may suffer from CP. According to the International Forum for the Study of Itch (IFSI), CP may present on inflamed skin (IFSI I), on normal appearing skin (IFSI II), or accompanied by chronic scratch lesions, such as chronic prurigo or lichen simplex chronicus (IFSI III) (9). As for the underlying aetiology, CP may arise from dermatological, systemic, neurological or psychiatric/psychosomatic conditions. Some patients show multiple causes for the pruritus (multifactorial CP), while in few cases the origin of the pruritus remains unknown despite extensive diagnostic work-up (9). Recent studies have further suggested a substantial impact of climate and weather on the prevalence of pruritus, especially involving specific localizations on the body, but these issues have yet to be examined in epidemiological studies (2–4). Adding to these factors, patients with CP vary in terms of medical history, comorbidities, co-medication, socio-economic backgrounds and therapy goals, contributing to the complexity of the management of these patients.
Due to the complexity and multidimensional nature of CP, clinical research investigating several aspects of pruritic diseases and its management is needed. In particular, clinical research contributes to a better understanding of pathophysiological mechanisms involved in the development and chronicity of CP in humans. Moreover, clinical researchers should focus on various aspects of clinical management, such as standardizing diagnostic and therapeutic procedures, and assessing the humanistic burden and impact of CP on affected patients. Another important area is the performance of longitudinal translational studies, clinical trials investigating novel agents for the treatment of CP, and psychometric research. It should also be investigated how the care of patients with CP is integrated into the health system in order to identify shortcomings and to adopt innovative strategies, as, for example, digital tools to improve care. The next section of this article discusses the challenges and difficulties with regard to these issues.
Understanding the pathophysiology
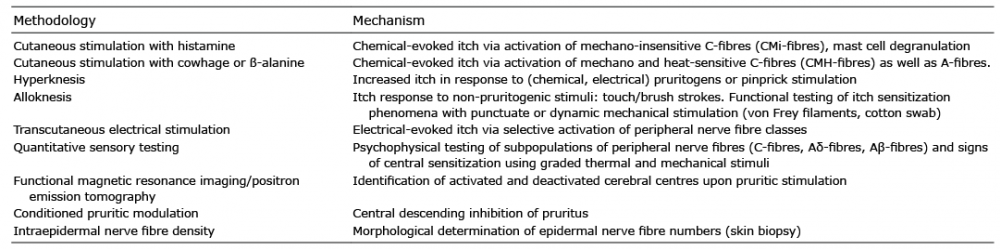
Basic and clinical research has led in recent decades to a better understanding of the mechanisms underlying CP. In clinical-translational research, different methods investigating specific pathophysiological features that augment data obtained from morphological and molecular biological research have been established and validated. The collaboration with biostatisticians and experts of medical informatics is essential for the interpretation of data and for obtaining a comprehensive understanding of the results. An overview of these methods is given in Table I.
Table I. Clinical research methodologies used in itch research
Several methodologies have been developed in order to investigate the functions of peripheral nerves. Skin stimulation with pruritogens (e.g. histamine, capsaicin, cowhage, β-alanine) has led to the characterization of several subpopulations of C-fibres. Histamine activates mechano-insensitive C-fibres (CMi-fibres), while cowhage and β-alanine activate heat and mechano-sensitive C-fibres (CMH-fibres) (10). Hyperknesis related to cowhage-induced pruritus, but not histaminergic pruritus, is present in several types of CP compared with controls, arguing for sensitization of CMH-fibres in CP (11). One limitation of this methodology is the high inter-individual variability, while intra-individual variability is low (12). Another method, transcutaneous electrical stimulation, allows the selective activation of subpopulations of peripheral nerve fibres. For example, using the Neurometer® C, Aδ and Aβ fibres are activated by electrical stimulation at a frequency of 5, 250 and 2,000 Hz, respectively (13). Higher itch intensities could be induced upon stimulation at 5 and 2,000 Hz in patients with CP of different origins compared with healthy individuals, arguing for hyperknesis in patients with CP (14). Of note, patients are often anxious when undergoing experimental procedures with electrical stimulation, which leads to biased ratings of evoked sensory symptoms, thus constituting a limitation of this method. Another functional well-established diagnostic tool that is used for clinical itch research is quantitative sensory testing (QST). It is a battery of psychophysical tests, in which response to graded thermal and mechanical stimuli is assessed (15). This procedure, originally developed for determination of neuropathic pain, informs about gain or loss of function of different peripheral nerve fibre subpopulations and hints at possible signs of central sensitization. In itch research it could be shown that patients with CP of different origins have an altered QST profile, arguing for disordered peripheral neuronal mechanisms (11). Although QST is widely used in neurological routine care, it has some limitations. It is time-consuming, requires highly qualified personnel, as well as the collaboration of patients. Morphological methodologies for investigation of the anatomy of cutaneous cells and expression of receptors and mediators are essential in clinical itch research. In particular, determination of the intraepidermal nerve fibre density is useful in order to reveal potential epidermal neuroanatomical alterations (16). In this examination, a skin biopsy is obtained and intraepidermal nerves are stained with the axonal marker protein gene product 9.5 (17). This simple method, which is also used in routine care, has some limitations. The skin probe is sensitive to the fixative and needs to be processed in a timely manner in the laboratory. In addition, reference values are available only for the distal lower leg (18, 19), thus interpretation of values from other body sites is difficult. It is a purely morphological examination, which does not inform on functional alterations of peripheral nerve fibres.
Central processing of pruritus is very challenging. Most current knowledge on spinal transmission of itch was obtained from animal studies (20). Functional magnetic resonance imaging (fMRI) and positron emission tomography (PET) studies have been used to investigate transmission and processing of pruritus in upper centres. Most studies have been performed on healthy volunteers exposed to pruritic stimulation during the scans. Brain regions associated with sensory recognition, cognition, motor response and emotional states are activated in response to pruritus (21). Interestingly, both overlapping and distinct brain areas are activated upon histaminergic and non-histaminergic pruritic stimulation, pointing to differences in cerebral processing of distinct pruritus types (22). Patients with CP also show differences in brain activation upon stimulation with histamine compared with healthy individuals, arguing for central sensitization in CP (23). Also, structural changes in grey matter have been observed in patients with CP, showing the neuroplasticity in chronic states (24). Although functional imaging studies have enhanced our understanding of cerebral processing of pruritus, this methodology has some pitfalls. fMRI and PET are very expensive methodologies, which are available only in specialized centres. In addition, patients with claustrophobia, ferromagnetic prostheses or implanted devices (e.g. defibrillator) cannot undergo an MRI examination, while others (e.g. children) have difficulty lying still during the procedure, leading to poor imaging quality. More imaging studies, enrolling patients with CP of different origins, are needed in order to establish similarities and differences in cerebral brain processing of pruritus across distinct CP conditions.
Upper centres exert a descending inhibitory modulation via a noradrenergic and a serotonergic pathway, as shown by imaging studies (21, 25). The paradigm of conditioned pain modulation (CPM), in which a noxious stimulus inhibits pain elsewhere in the body, can be used experimentally to assess descending inhibition (26). In patients with CP, as in those with chronic pain, CPM is impaired, which may contribute to the chronicity of the pruritus (11). An analogous paradigm of conditioned pruritic modulation, in which a pruritic stimulus inhibits pruritus elsewhere in the body, has also been investigated, with conflicting results regarding its effect (27, 28). More studies are needed to enhance the understanding of the mechanisms of descending modulation in CP and its role in the chronicity of the disease.
Standardization of assessment instruments
Since pruritus has a subjective dimension, patient-reported outcomes (PRO) play a pivotal role. A plethora of standardized questionnaires and scales have been developed in order to gather information on several aspects of CP, including pruritus characteristics, course of the disease, QoL, reactive disorders, such as anxiety, depression and sleep impairment, and therapy goals.
Pruritus characteristics (e.g. onset, duration and distribution of pruritus, as well as accompanying sensory symptoms and scratching behaviour) can be assessed using general patient-oriented itch questionnaires (29, 30). Mono-dimensional scales, namely the visual analogue scale, the numerical rating scale and the verbal rating scale, have been validated to assess the intensity of pruritus (31). Intensity scales are also validated for the use in electronic diary applications (32). The interpretation of itch intensity scales is challenging, since scores vary from patient to patient according to external factors, such as sex or ethnic background (1, 33). Some efforts have been put into understanding the minimal clinical relevant difference of itch intensity change, e.g. after initiating a therapy (34). However, many factors (e.g. the aetiology of the pruritus, recall period, socioeconomic background) may influence the minimal clinical relevant difference, making the interpretation of results difficult. An overview of other instruments for the assessment of itch is shown in Table II.
Table II. Examples of instruments for itch assessment
As for secondary conditions arising due to CP, standardized questionnaires are used to screen for anxiety and depression (e.g. Hospital Anxiety and Depression Scale (35)), to assess sleep disorders (36, 37) and to measure the impairment of QoL (e.g. Dermatological Life Quality Index (38) and pruritus-specific ItchyQol (39)).
PRO measures are usually collected via paper and pencil questionnaires, but electronic PRO systems are emerging. Computerized collection of PRO measures offers a couple of advantages compared with paper questionnaires: reduction of errors emerging through typewriting, reduction of missing data by requiring completion, and reduction of invalid data by implementation of skip patterns (40). Furthermore, electronic assessment can increase the compliance of completing questionnaires at home by up to 70%, using, for example, computerized reminder functionality (40). To overcome the drawbacks of paper questionnaires, an electronic PRO system, enabling the patient to complete the PRO measures via digital survey, may be implemented (41–43). Since most PRO measures have been validated as paper tools, it cannot be assumed that the electronic version of the same PRO measures deliver the same results for a patient encounter. Gwaltney et al. (40) showed that “as long as substantial changes are not made to the item text or response scales, equivalence studies should not be necessary to demonstrate anew the equivalence or validity of a computerized measure”. However, in order to ensure the validity of electronic measures, it would be preferable if the concrete implementations were examined using test–retest or alternate-forms reliability.
Standardization of itch assessment instruments across centres treating patients with CP is of great importance, since it would allow the comparability of data. A first step was already taken by the Task Force Pruritus of the European Academy of Dermatology and Venereology. In a consensus conference, it was agreed that pruritus intensity and QoL should be regarded as the 2 most important parameters to be assessed in routine care. The visual analogue scale and the ItchyQol were regarded as the instruments of choice (44). Another important task is the validation of the assessment tools into various languages in order to be used in clinical trials and routine care across different countries. Future clinical research should focus on showing which instruments have better utility for the clinical practice and which tools are better accepted by patients and physicians.
Understanding the humanistic and economic burden
CP, similarly to chronic pain, can lead to a severe impairment of QoL (45–47) and has negative effects on mood, ability to concentrate, quality of sleep, everyday life and work productivity (48, 49). Some patients have mental health problems, such as depression, in response to CP, and are at significantly higher risk of suicide (50, 51). QoL is a highly subjective construct and is influenced by various factors, such as pruritus intensity, but also duration, frequency and localization of pruritus. Another challenge in understanding the impact of pruritic conditions on affected patients is that cross-cultural factors influence the reported intensity of pruritus and QoL rather than the specific dermatological diagnosis. This could be found in a study in 9 European countries enrolling more than 500 patients with CP due to different dermatoses (6). Clinical research should take the cultural background of patients with CP into account when investigating the humanistic burden of pruritic conditions.
In addition to limiting QoL, there are often psychiatric complications. Patients with CP and with a psychosomatic/psychiatric comorbidity suffer more from CP and its consequences. Interestingly, even if their symptoms improve, psychological suffering is higher in these patients (52). In order to cope with these associated disorders, individual multimodal medical care is needed, not only for diagnosing the underlying disease of CP and for symptomatic antipruritic therapy, but also for adjunct therapy against, for example, sleep disorders or mental health conditions. An important challenge for clinical researchers is to detect risk factors for developing mental diseases in patients with CP and thus identify patients at risk. This would aid attending physicians in redirecting vulnerable patients to mental health professionals and ultimately to improve care.
Definition of treatment goals
As a multifactorial chronic disease, CP requires complex and cost-intensive therapy. Knowledge of the treatment goals of patients with CP is therefore of great importance in order to plan an efficient therapy regimen. Therapy goals were recorded and evaluated in 2,474 patients with CP using the Patient Benefit Index – Pruritus (PBI-P), which was validated in 2009 for patients with CP and consists of 27 items, including various aspects, such as physical and mental well-being, professional and everyday performance, social and leisure activities, and QoL in general. The relevance of these items is calculated on the basis of a 5-step Likert scale (0=”not at all important” to 4=”very important”) (53). It was shown that, in addition to demographic data such as sex and age, the CP IFSI group, pruritus intensity and QoL had a significant impact on different patient needs. Women considered the reduction in physical and psychological symptoms, such as depressive feeling, nervousness, or burning sensations, as more important (54). For men, an important goal was the improvement in aspects of social life, such as social contacts, partnership, and sex life. Patients with CP on inflamed skin (IFSI I) or pruritus with chronic scratch lesions (IFSI III) considered the healing of the skin lesions as a very important treatment goal (54). Overall, it has been shown that therapeutic goals relate to the diagnosis and medical therapy. Reduction in pruritus or confidence in therapy were considered important or very important by the majority of patients with CP. However, patients with CP focus not only on symptom relief, but also on trustworthy and efficient medical action. Their overall need level seems to be higher than in other dermatological patients as, for example, patients with atopic dermatitis (54). The complexity of patients’ needs constitute a challenge for clinical researchers, since patients’ needs and goals influence how they perceive their disease and the efficacy of a therapy. Patients’ needs should thus be taken into consideration when planning studies involving patients with CP.
Standardization of diagnostic and therapeutic procedures
Owing to the heterogeneity of CP conditions, it is difficult to achieve a standardized diagnostic and therapeutic approach across specialized centres and physicians treating patients with CP. The first guideline addressing CP was published in Germany in 2006 (55) and constituted an important first step in this regard. Since then, the German guideline has been regularly updated (56), while a European guideline was also developed and recently updated (57).
There is still a lack of randomized controlled trials investigating anti-pruritic drugs, and therefore many of the recommendations of current guidelines are based on case series, case reports and expert opinion. Another challenge that guidelines face is the heterogeneity of CP aetiologies. For instance, while antihistamines are effective in the treatment of urticaria, they do not reduce pruritus in other diseases, such as atopic dermatitis or systemic pruritic conditions (58). Therefore specific therapeutic recommendations are needed for the various pruritic conditions. Clinical trials targeting different pruritic diseases (e.g. atopic dermatitis, uraemic pruritus, cholestatic pruritus, paraneoplastic pruritus) are of the utmost importance in order to generate quality data on which to base therapeutic recommendations.
Dermatologists are usually the first specialists consulted for CP and play a key role in the management of CP. Their job is not only to treat the CP, but also to assign the patient to local physicians of other specialties for specific diagnostic procedures (e.g. medical imaging). However, due to time constraints, taking a comprehensive medical history in patients with CP is challenging in a dermatological practice. Reactive disorders of CP, such as depression and anxiety, need to be considered, as possible causative factors and skin findings, comorbidities and medication must be well documented. The consultation of patients with CP in specialized pruritus centres can offer an important advantage in the management of CP, especially when refractory to basic therapeutic measures, such as antihistamines, topical steroids and the use of emollients. However, the centres are scarce and more are needed for the current demand (7). Pruritus centres should work on an interdisciplinary basis together with medical specialties other than dermatology, such as internal medicine, neurology, pain medicine, psychosomatics, radiology, and medical informatics (59). In addition to outpatient care, specialized centres should also offer the possibility of inpatient care for highly complex patients who require extensive diagnostic procedures or who have relevant psychosocial factors, such as suicidal ideation or severe sleep impairment (59).
Guideline-based treatment of patients with CP at specialized centres can significantly reduce costs, both in the inpatient and outpatient sectors. This is the result of a recent study in which data from 300 patients with CP were analysed regarding their QoL, health economic burden and therapeutic benefits. Six months after the start of treatment at a specialized pruritus centre there was not only a significant improvement in the pruritus intensity, QoL and therapeutic benefit (PBI-P), but also a significant reduction in all costs (60).
Need for novel effective therapies
Owing to a better understanding of the mechanisms underlying CP, new promising agents with an anti-pruritic effect have been identified and are being tested in randomized controlled trials. These include monoclonal antibodies (e.g. nemolizumab, tralokinumab), neurokinin-1 receptor antagonists (e.g. serlopitant, aprepitant), opioid modulators (e.g. nalbuphine, nalfurafine), phosphodiesterase-4 inhibitors (e.g. apremilast, crisaborole), janus kinase inhibitors (e.g. tofacitinib) among other novel agents.
The development of innovative drugs faces important challenges. So far, clinical trials have been performed only for a few indications, especially atopic dermatitis, chronic prurigo, uraemic and cholestatic pruritus. For many other pruritic conditions clinical trials are lacking, and thus no novel drugs are available.
Since these new agents represent a high cost for the healthcare system, it is important to select the patients who can profit the most from them. Clinical trials and observations from routine care should inform which target population is suitable for each drug.
At present, innovative drugs being tested in clinical trials are available in only a few centres and thus not all patients have access to them. Licensing of these drugs is needed in order to extend the availability of these promising agents to patients in need. Hence, clinical research should focus on producing high-quality data on the safety and efficacy of novel anti-pruritic drugs, so that regulatory agencies can approve these medications.
Clinical research efforts in CP have increased in recent years, leading to better understanding of this condition, and ultimately to better care. However, the multidimensional nature of this condition and the heterogeneous population affected by CP pose a challenge for clinical researchers and attending physicians. Unmet needs, such as the shortage of knowledge on chronicity mechanisms, insufficient standardization of a diagnostic and therapeutic approach to CP patients, and the development of novel promising drugs for refractory CP, ought to be targeted by researchers and physicians dealing with CP.
This article was supported by the German Research Foundation (DFG, No. FOR2690 to KA and SST) and by the European Academy of Dermatology and Venereology (EADV, No. 2016-012 to MP and SST).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize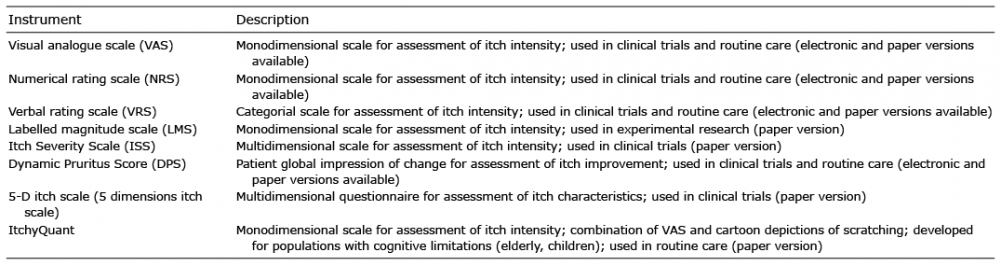 Click to show fullsize
Click to show fullsize