


1Dermatology and Venereology Division, Department of Medicine (Solna), Karolinska Institutet, 2Dermato-Venereology Clinic, Karolinska University Hospital, Karolinska vägen 6, SE-176 71 Stockholm, 3Department of Laboratory Medicine, H5 Pathology, Karolinska Institutet, and 4Department of Pathology and Cytology, Karolinska University Laboratories, Stockholm, Sweden. *E-mail: jakob.wikstrom@ki.se
Accepted Dec 12, 2019; Epub ahead of print Jan 2, 2020
Acta Derm Venereol 2020; 100: adv00082
Amelanotic melanoma (AM) is a rare subtype of cutaneous melanoma that lacks melanin pigment. Clinical diagnosis of AM is challenging because it may mimic benign or malignant melanocytic and non-melanocytic neoplasms and inflammatory skin diseases. Completely amelanotic melanomas are rare, but approximately 2–8% of all melanomas lack pigment or are sparsely pigmented (1, 2). AM often present a particular diagnostic challenge due to their inconspicuous appearance and lack of the classical, well-recognized characteristics and clues found in pigmented lesions (3). In particular, when concealed by an inflammatory dermatosis, such as psoriasis, AM can remain undiagnosed for a long time (4). We describe here, to our knowledge, the first case of AM concealed by psoriasis.
A woman in her mid-20s presented with psoriasis treated with topical glucocorticoids and oral methotrexate (MTX), 15 mg/week. She had never received ultraviolet (UV) treatment and there was no history of skin malignancies in her family. She had recently experienced an exacerbation due to discontinuation of her systemic treatment. At clinical examination erythemato-squamous plaques were observed on the legs, arms and trunk. She had recently noticed a new plaque on her lower left leg (Fig. 1A, B), while the rest of her psoriasis had remained stationary for a long time. Upon intensive treatment with glucocorticoid creams and resumed MTX all plaques gradually disappeared, except the new lesion, which measured 1.5 cm in diameter (Fig. 1C, D). A punch biopsy and histopathology showed invasive melanoma. The remaining lesion was excised with a 2-mm margin for full assessment and staging. Histopathology of the tumour and re-examination of the punch biopsy led to a final diagnosis of AM, Breslow thickness 0.9 mm, Clark level IV, tumour stage pT1b (Fig. 2). A wide local excision with 1-cm margin was performed. One year later the patient remains disease-free and her psoriasis is under good control.
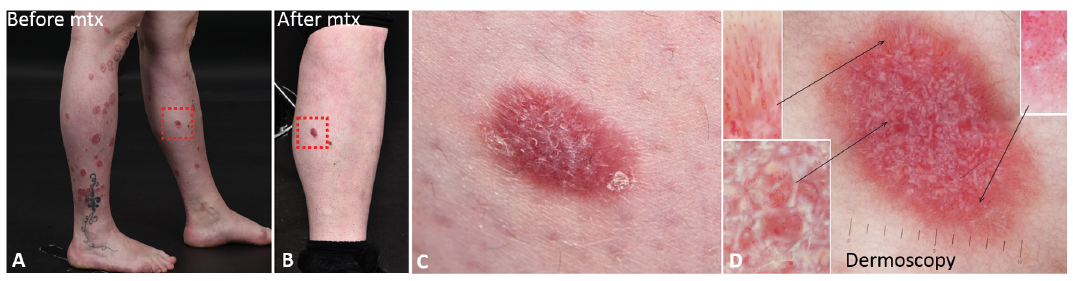
Fig. 1. Clinical picture and dermoscopy. (A) Psoriasis plaques on the lower legs with the melanoma highlighted. (B and C) After successful treatment for psoriasis with methotrexate the melanoma persisted. (D) Dermoscopy. Note: 2 images were merged. Polymorphic vascular pattern including dotted, coiled and looped vessels arranged randomly over the surface, showing a radiating arrangement in the periphery. Large red clods confining clusters of looped vessels. White lines and clods are seen over the entire surface under polarization dermoscopy. Dermoscopy × 10. Highlights × 20.
Fig. 2. Histopathology. (A–C) Haematoxylin and eosin staining showing prominent nests of atypical melanocytes of variable sizes (arrows) surrounded by an extensive inflammatory infiltrate (asterisks). (D and E) Melan-A stain confirming the nests as consistent with melanocytes. A, D: × 4, B: × 10, C: × 40, E: × 6.
To our knowledge, this is the first published case of AM concealed by psoriasis. AM is a rare entity (1, 2, 4), especially in a young patient without risk factors for melanoma, such as heredity, high levels of UV exposure or other significant risk factors, besides immunosuppression due to MTX. A small, but significant, increase in risk for cutaneous melanoma in patients treated with MTX has been concluded recently in a Swedish nationwide register study (5). AM is associated with poorer survival, as it commonly remains undiagnosed for longer than pigmented melanomas. Dermoscopy can aid in diagnosing AM (1, 2), but in the setting of concealing inflammatory dermatoses, such as psoriasis, AM can remain hidden until the inflammatory plaques subside. Psoriasis is common and has a global prevalence in adults of approximately 0.91–8.5 % (6); therefore it is not feasible to apply dermoscopy to every psoriasis plaque in every patient. The specific clues to AM differ from the signs of psoriasis and other inflammatory dermatoses in some important respects. In flat AM in particular, a combination of dotted vessels and linear vessels may be a strong clue to melanoma. Among non-vascular features white lines can be considered as the most important clue for AM (1, 2).
Dermoscopy of psoriasis is typified by regularly distributed dotted vessels and white scales. In our case white scales were present, as well as vessels as dots, but coiled and looped vessels were also abundant. Polarizing-specific white lines and polymorphic vessels are unexpected findings in psoriasis and were also a reason for biopsy.
To prevent difficult-to-find AM from going undiagnosed, it is crucial to be alert to patient history and employ a high index of suspicion regarding new or therapy-refractory plaques. We recommend using dermoscopy to scrutinize aberrant lesions and apply a low threshold for biopsy or excision in response to atypical findings.
The authors thank the patient for granting permission to publish this case report.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize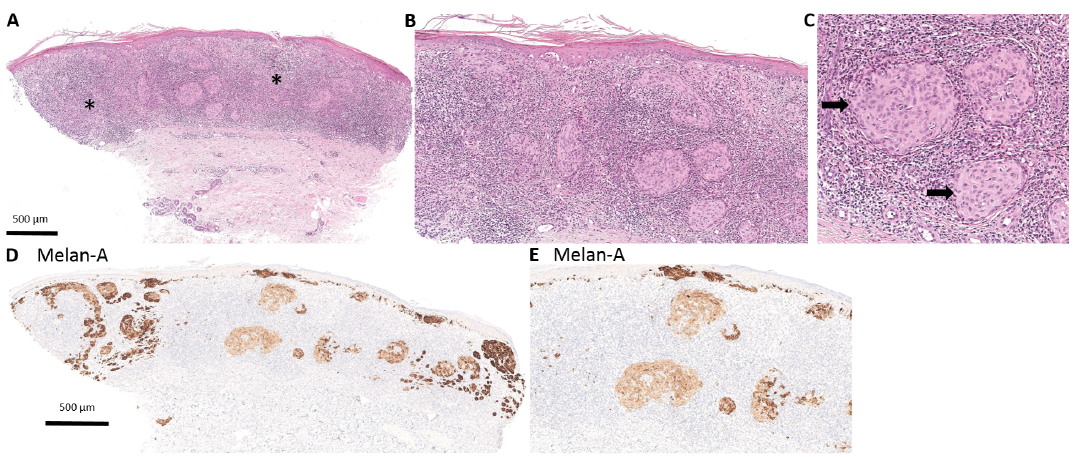 Click to show fullsize
Click to show fullsize