


1Department of Dermatology, University of Pennsylvania, Philadelphia, 2Geisinger Medical Center, Danville, PA, and 3Johns Hopkins University School of Medicine, Baltimore, MD, USA
Folliculotropic mycosis fungoides is a variant of cutaneous T-cell lymphoma characterized as having a folliculocentric infiltrate of malignant T cells along with a worse prognosis in comparison to the epidermotropic variants. Patients with advanced forms of folliculotropic mycosis fungoides are often poorly responsive to both skin-directed as well as to systemic therapies. We report here a high response rate using a novel therapeutic regimen combining interferon gamma, isotretinoin in low dose and topical carmustine, and in some cases concomitant skin-directed therapies, among 6 consecutive patients with refractory folliculotropic mycosis fungoides with stages IB through IIIB who had previously failed both topical and systemic therapies. The potential mechanisms of this multimodality approach are discussed.
Key words: cutaneous T-cell lymphoma; folliculotropic mycosis fungoides; interferon-gamma; carmustine; isotretinoin; therapeutic approach.
Accepted Feb 19, 2020; Epub ahead of print Mar 4, 2020
Acta Derm Venereol 2020; 100: adv00187.
Corr: Christina Del Guzzo, MD, Dermatology University of Pennsylvania, 3600 Spruce St, 2 Maloney, Philadelphia, PA 19104, USA. E-mail: christina.delguzzo@pennmedicine.upenn.edu
Folliculotropic mycosis fungoides is a distinct subtype of cutaneous T-cell lymphoma with poor prognosis and recalcitrance to conventional therapy. We propose a novel therapeutic approach for refractory folliculotropic mycosis fungoides using interferon gamma in combination with topical carmustine and low dose isotretinoin, and in some cases other skin-directed therapies including phototherapy and local radiation. Among 6 patients with advanced folliculotropic mycosis fungoides who had previously failed prior systemic therapy, four patients experienced complete responses with the other two having nearly complete responses while being treated with this regimen. The potential mechanisms of this treatment approach are discussed.
Folliculotropic mycosis fungoides (FMF) is a well described and distinct clinicopathologic variant of cutaneous T-cell lymphoma (CTCL) in which the malignant T-cell infiltrate invades the follicular unit. This contrasts with classical mycosis fungoides (MF) which typically manifests as epidermotropism of the malignant T cells without specific predilection for follicular epithelia. In general, FMF has a worse prognosis than the conventional epidermotropic variant of MF, even in early stages of the disease (1, 2).
Treatment of FMF is often challenging given its refractory nature to commonly used skin-directed and systemic therapies, including topical nitrogen mustard, UVB phototherapy, bexarotene and interferon (IFN)-α (1–3). The difficulty in obtaining and maintaining a treatment response in FMF is believed to be in part due to the deep penetration of lymphocytes into the hair follicle that limits responsiveness to many superficial skin-directed therapies. Others have proposed that it may also be related to a gene expression profile intrinsic to pilotropic tumor cells associated with poor prognosis (3, 4). It has already been demonstrated that topical carmustine is effective as monotherapy in early stage FMF, likely, in part, due to its deeper penetration than other topicals (5).
In this report, we describe a series of 6 patients with stage IB or greater FMF with treatment refractory disease who demonstrated clinical response to a novel multimodality therapeutic approach using IFN-γ in combination with topical carmustine ointment and/or low dose oral isotretinoin. The choice to evaluate these particular therapies was based upon the clinical experience of the dermatologists at the University of Pennsylvania and the hypothesis that these particular agents more effectively target the folliculocentric lymphocytes of FMF.
Patients
After obtaining approval from the institutional review board at the Hospital of the University of Pennsylvania, we conducted a retrospective review of patients with FMF treated in the Penn Cutaneous Lymphoma Clinic at the Hospital of the University of Pennsylvania between 2009 and 2019. Inclusion criteria for the study were patients with Stage IB or greater FMF that proved refractory to two or more therapies, including one systemic therapy, prior to initiation of a regimen of IFN-γ in addition to topical carmustine and/or low dose isotretinoin. The patients were identified by the clinicians individually screening their FMF patients for inclusion criteria. Six patients met inclusion criteria for the study. We have previously published a series of predominantly early stage patients that demonstrated that carmustine is a safe and effective treatment for FMF (5); this study focuses on more advanced and refractory patients.
Diagnosis was made by clinical and histologic criteria. Staging was based upon the recent ISCL/EORTC guidelines (6). Assessment of peripheral blood findings was conducted by flow cytometry and T-cell receptor gene rearrangement studies.
Treatment protocol
The course of optimal therapy was designed based on the clinicians’ experience using these therapeutics either individually or in a combined fashion. The starting dose of IFN-γ was 50 µg (1 million units) subcutaneously 3 times per week. The dose was typically elevated after 2 weeks if well tolerated to 100 µg 3 times weekly. Isotretinoin was started at 10 mg daily and increased to 20 mg daily as tolerated. Carmustine ointment was compounded by the pharmacy at the Hospital of the University of Pennsylvania. The 0.04% ointment was prepared by dissolving carmustine in absolute ethanol followed by mixing carmustine (BCNU) with Aquaphor ointment. Patients were instructed to apply the ointment overnight 5–7 times per week, with removal in the morning during bathing.
Patient response evaluation
The primary endpoint was global response based upon physical examination of skin and peripheral blood assessment. Partial response (PR) in the skin was defined as 50% or greater improvement in overall BSA. Complete clinical response (CR) was defined as full resolution of lesions on physical examination with no residual visible changes of follicular plugging or active skin lesions as well as continued absence of lymphadenopathy as none of the patients had lymphadenopathy at baseline. Flow cytometry was used to assess response in the peripheral blood for the one patient with blood involvement. Complete response in the blood was defined as B0 blood involvement following initiation of the treatment regimen (7). Patients were evaluated every 3 months. Post-treatment biopsy was not routinely performed. Toxicities were scored using CTCAEv4.0 (Common Terminology Criteria for Adverse Events version 5.0).
Patient characteristics
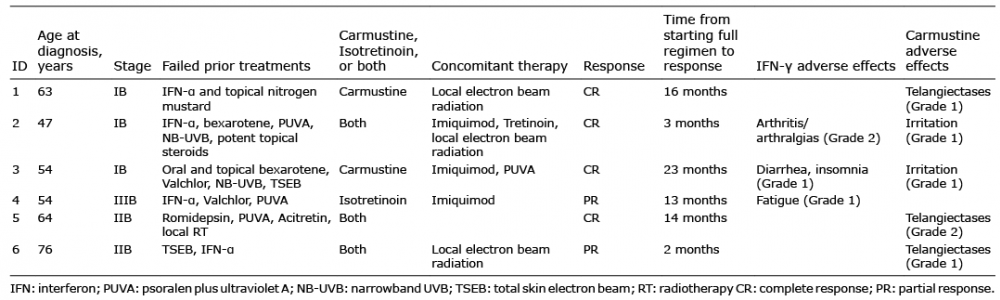
All 6 of the patients in the study were men, consistent with the male predominance of FMF noted in other studies (1, 2, 8). The median age at diagnosis was 58.5 years (47–76 years). At the time of diagnosis, 3 patients were stage IB, two patients were stage IIB, and one patient was stage IIIB. All of the stage IB and IIB patients had B0 blood involvement. All of the patients had refractory disease with 5 of the patients having failed both skin-directed therapies and systemic agents and two patients had progressive disease following total skin electron beam prior to starting the aforementioned triple drug regimen (Table I). The mean number of systemic and topical therapies failed prior to initiation was 3.5 (range 2–5).
Table I. Characteristics of 6 male patients with folliculotropic mycosis fungoides at initial diagnosis and response to therapy
Response to therapy
All of the patients were on IFN-γ, carmustine and/or isotretinoin simultaneously, but they were not initiated or discontinued concurrently in all patients. Three of the 6 patients were started on multimodality therapy concurrently, whereas two of the patients were initially started on IFN-γ with the addition of carmustine and/or isotretinoin within one year (3–11 months). One patient was started on carmustine with the addition of IFN-γ after 10 months. The mean time to at least partial response after initiating the selected full multimodality regimen was 13.7 months (2–23 months). The mean duration of follow-up was 50.5 months (32–59 months). All 6 patients were alive at last follow-up.
Three patients, one Stage IB and two Stage IIB, were treated with IFN-γ, carmustine, and isotretinoin. Two Stage IB patients received IFN-γ and carmustine. The single Stage IIIB patient was treated with IFN-γ and isotretinoin. Four patients achieved CR, and two achieved PR (Table I and Fig. 1). Of the 4 CRs, one was induced after experiencing a PR prior to addition of psoralen plus ultraviolet A (PUVA) to the regimen and two others after electron beam radiation to a single residual plaque. In addition, one of the patients that achieved a PR had limited local electron beam radiation therapy to isolated lesions that did not fully respond to therapy. Two of the 4 patients with a CR had a sustained CR at last follow-up. Patient 5 has had a sustained remission for 23 months on isotretinoin alone at last follow-up and Patient 2 has maintained his remission for 4 months on only methotrexate for acquired arthritis. Time to relapse for Patient 1 was 5.0 months but he developed only minimal disease recurrence of less than 1% BSA at last follow-up. Time to relapse for Patient 3 was 8.3 months but occurred in the setting of self-discontinuing IFN-γ and carmustine following his CR. One of the PRs (Patient 4) had a near complete response with very minimal active disease (< 2% BSA) that was sustained for a year but he developed somewhat worsened disease in the setting of having to dose reduce IFN-γ due to fatigue. The second PR was in a Stage IIB patient (Patient 6), who presented with extensive plaques and tumors, and who had initially improved significantly with minimal disease involvement (BSA 1%) on all 3 agents but worsened after having to discontinue IFN-γ for multiple months due to cost. None of the patients had nodal involvement at baseline nor did they develop clinical lymphadenopathy during the course of evaluation.
Fig. 1. Folliculotropic mycosis fungoides. A) Patient 5 prior to initiating therapy with proposed multimodality regimen. B) Complete response following treatment with interferon-γ, topical carmustine, and low dose isotretinoin. Permission given to publish these photos.
Tolerability
Treatment was not stopped at a particular time point but rather was discontinued for various reasons including complete response, progressive disease or adverse effects. Two of the 6 patients were on IFN-γ at the time of last follow-up. Two of the 4 patients (Patients 1 and 5) that discontinued IFN-γ were tapered off after complete response. IFN-γ was discontinued in one patient (Patient 2) due to the development of arthralgias while receiving local radiation therapy and IFN-γ simultaneously. Patient 6 discontinued IFN-γ due to prohibitive cost. Two patients could not tolerate the full dose of 100 µg of IFN-γ and required dose reduction due to the adverse effects including diarrhea, fatigue, and insomnia with resolution of these effects with lower doses.
Of the 5 patients on carmustine, 3 patients developed telangiectases. Two of the patients had only localized areas of involvement (Grade I) and did not discontinue carmustine due to this. Of note, both of these patients also had electron beam radiation, which is also known to cause telangiectases. The third patient developed Grade II telangiectases and discontinued the ointment due to this effect, Table I and Fig. 2. Two patients on carmustine experienced minor irritation after starting the ointment that improved with continued use and neither discontinued the medication due to the irritation. No specific adverse effects were reported with use of low dose isotretinoin.
Fig. 2. Telangiectases as a complication of topical carmustine therapy.
We report a series of 6 consecutive patients with advanced refractory folliculotropic mycosis fungoides who manifested significant clinical responses to a multimodality therapeutic approach using IFN-γ, carmustine ointment and low dose isotretinoin. Four patients experienced complete responses with the other two having nearly complete responses while being treated with this regimen. Four of the 6 patients also received skin directed therapy consisting of local electron beam radiation in 3 while one received PUVA in an effort to completely clear the skin disease. The regimen was well tolerated without significant adverse events. Although we were unable to assess precisely the time to treatment response as the treatment agents were typically added in a stepwise manner, responses characteristically proceeded in a slow but continuous manner.
IFN-γ remains an important component of our immunotherapy regimens for the treatment of advanced stage CTCL. We have previously reported on the high clinical response rates of Sezary syndrome patients to multimodality regimens employing IFN-γ along with photopheresis with or without retinoid compounds (9). In this setting, it has often been our experience that replacement of IFN-α with IFN-γ has resulted in improved clinical status and immunological responsiveness (9). We do know that IFN-γ can potently activate antigen presenting cells which would be advantageous when simultaneously treating patients with photopheresis or other therapeutics that require participation of antigen presenting cells, such as with Toll-like receptor agonists.
In our current series of patients with FMF, use of IFN-γ appears to have similarly produced benefit superior to that achieved with IFN-α. Mechanisms underlying the superiority of IFN-γ have not been clearly defined. The perifollicular infiltrate may be a critical site at which IFN-γ may exert a prominent effect. Within the biopsies of many of our patients with folliculotropic mycosis fungoides, reactive CD8+ T cells of varying intensity may be observed in the perifollicular region, adjacent to the malignant cells (Fig. 3). It is possible that IFN-γ may exert a more prominent effect than IFN-α to activate the antitumor activities of the cytotoxic T cells, although this remains unproven at this time. An important advantage of IFN-γ is that it appears to produce fewer cognitive, neurologic, constitutional and autoimmune adverse effects when compared to IFN-α (10). As response rates are often slow, long term therapy with IFN is typically required. Thus, a systemic therapeutic agent with fewer adverse effects, such as low dose IFN-γ, is clearly highly desirable.
Fig. 3. Perifollicular CD8 T-cells in a CD4 predominant folliculotropic mycosis fungoides.
Another important component of our treatment regimen for refractory FMF involved the use of 0.04% compounded carmustine ointment. We have previously reported on the benefit of this agent among FMF patients who had failed to respond to topical nitrogen mustard ointment (5). Our clinical experience has repeatedly demonstrated greater efficacy of carmustine ointment in comparison to nitrogen mustard for therapy of FMF. In regard to the conventional concentrations of both compounds currently in use to treat CTCL, it is clear that measurable metabolites of carmustine can be found in blood and urine, while in contrast, no metabolites of nitrogen mustard can be measured in these compartments (11, 12). This data suggests that carmustine may successfully penetrate down to the follicle while nitrogen mustard may be more rapidly metabolized in the upper regions of the skin accounting for the greater efficacy of the former drug. Larger trials of the use of carmustine are needed to more adequately define the action of this drug in FMF.
In addition to the use of IFN-γ and topical carmustine, low dose isotretinoin has been a useful adjunct to induce clinical responses among our FMF patients. Four of the 6 patients had failed the previous use of IFN-α and/or bexarotene in high doses, yet had excellent clinical responses to our triple-drug regimen which included isotretinoin. Isotretinoin can induce apoptosis of sebocytes within the follicular unit leading to atrophy of sebaceous glands (13). Whether this effect may alter chemotaxis and recruitment of malignant T cells into the follicle in FMF is unknown. Nevertheless, it does appear that isotretinoin may synergize with Th1 cytokines to enhance CD8+ T-cell functions (14, 15). This effect may also be critical in regard to activating the perifollicular cytotoxic T-cell response.
The study was limited by small patient numbers from a single institution in addition to variable timing of initiation and duration of treatment for the different drugs in the regimen. In addition to IFN-γ, isotretinoin, and carmustine, additional skin-directed therapies, including highly localized electron beam in 3 cases and PUVA in one case, were used as therapy; while the addition of these therapies could be seen as somewhat confounding, they were all added in an effort to convert a partial response to a complete response following initiation of the primary regimen. FMF is known to be recalcitrant to therapy and the duration to response was extended but nevertheless responses occurred in all patients on this regimen despite prior refractoriness to conventional therapy.
Given our understanding of FMF as a distinct subtype of CTCL with poor prognosis and recalcitrance to conventional therapy, we propose a novel multimodality therapy for FMF with therapeutic agents that likely more effectively target the deeply penetrating lymphocytes in the follicular unit that characterize the disease. We demonstrate that this combined systemic and skin-directed therapeutic approach using IFN-γ in combination with topical carmustine ointment, low dose oral isotretinoin, and in some cases radiation and phototherapy, allowed for complete response or near complete response in patients previously refractory to prior therapies, including IFN-α and bexarotene. Additional studies are needed to further characterize how these therapeutic agents target the tumor cells of FMF and to define the full range of benefits of these drugs in this more aggressive variant of CTCL.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize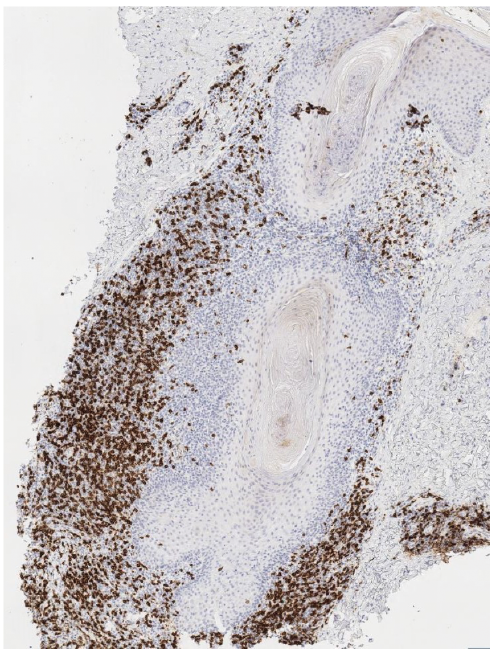 Click to show fullsize
Click to show fullsize