


1Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, and 2Copenhagen Research Group for Inflammatory Skin (CORGIS), Hellerup, Denmark
Prurigo nodularis is a pruritic dermatosis with poor treatment options. To describe treatment patterns, comorbidities, pruritus, and quality of life a survey was administered to 92 patients with prurigo nodularis. A total of 52 patients completed the survey. The most frequently used treatments were topical corticosteroids, which were prescribed to 49/52 patients, with positive effect in 13/49. A total of 46/52 patients were treated with ultraviolet B, and 9/46 reported a positive effect. A positive effect was reported for topical corticosteroids under occlusion in 21/40, for zinc dressing treatment in 17/37, for steroid injection in 9/14, for methotrexate in 5/16, and for thalidomide in 4/12 of treated patients. Thirty-six patients reported a Pittsburgh Sleep Quality Index >5, indicating poor sleep. Patients with prurigo nodularis are severely bothered by pruritus negatively affecting quality of life. Various treatments are prescribed; most frequently topical corticosteroids and ultraviolet B. Surprisingly, patients reported topical corticosteroids under occlusion, zinc-dressing treatment and steroid injection as the most effective.
Key words: prurigo nodularis; Hyde’s disease; pruritus; survey; treatment; quality of life.
Accepted Mar 24, 2020; Epub ahead of print Mar 26, 2020
Acta Derm Venereol 2020; 100: adv000119.
Corr: Tanja Todberg, Department of Dermatology and Allergy, University of Copenhagen, Herlev and Gentofte Hospital, Gentofte Hospitalsvej 15, DK-2900 Hellerup, Denmark. E-mail tanja.todberg@regionh.dk
Prurigo nodularis is a rare skin disease characterized by intense pruritus, leading to lack of sleep and reduced quality of life. For dermatologists worldwide, treatment of prurigo nodularis remains a challenge, as there are no approved treatments for the disease and patients are often insufficiently treated with the existing therapies. This patient-based survey examined treatment tendencies and treatment effectiveness, comorbidities, pruritus and quality of life in a cohort of patients with prurigo nodularis. Overall, topical corticosteroids and ultraviolet B are the most commonly used treatments; however, topical corticosteroids under occlusion, zinc-dressing treatment and steroid injection were reported as the most effective treatments.
Prurigo nodularis (PN) is a subtype of chronic prurigo dominated by multiple hyperkeratotic nodules with a symmetrical distribution (1, 2). The predominant symptom of PN is an intense pruritus, often leading to disturbed sleep and reduced quality of life (QoL) (3). PN is characterized as a distinct skin disease and is believed to be caused by underlying conditions in which itch is also part of the symptoms, such as atopic dermatitis, neuropathies, and chronic liver and kidney dysfunctions (2, 4). Repetitive itching on the skin may start a cascade of processes involving the immune system, neurones and epithelial cells, causing an urge to repeated scratching, known as the itch-scratch cycle (5). Many theories about the pathogenesis of PN have been hypothesized, including; growth of the peripheral nerves leading to hypersensitivity of the nerve endings, increased levels of substance P in the small nerve fibres in dermis, and interleukin-31 (IL-31) in blood; both being mediators of pruritus (6, 7).
For dermatologists, the management of PN is challenging, due to the lack of understanding of the disease, combined with limited treatment options.
To improve the knowledge of PN, a survey-based study was established to investigate demographic characteristics, comorbidities, commonly used treatments, pruritus specification and the effect of these from the patient’s perspective. Furthermore, the impact of PN on QoL was investigated.
Study approval was obtained from the Danish Data Protection Agency (ref. HGH-2017-120, I-Suite: 06038) and The Danish Health Authority (ref. 3-3013-2267/1). Patients were identified if they were ≥ 18 years of age and had been patients at the Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Denmark and received a diagnosis of PN (DL281) between 2006 and 2016. For all identified patients, charts were investigated to ensure that only eligible patients received a survey. Patients who had died, moved abroad, or had been misclassified with a PN diagnosis were excluded. The survey was programmed in REDCap and was sent to patients via email and regular post, as a large proportion of patients were elderly. The survey comprised 104 questions about PN, including previous and present treatments, the effectiveness of treatments assessed by the patient, pruritus specification, including visual analogue scale (VAS) pruritus, localization and intensity within the last month, active underlying dermatological and non-dermatological conditions, sociodemographic status, QoL, including Dermatology Life Quality Index (DLQI, range 0–30), and quality of sleep, measured by Pittsburgh Sleep Quality Index (PSQI, range 0–21, a score ≤ 5 defined as good sleep and > 5 indicating poor sleep). For the survey questions on treatments, all responses were validated with the registered data in the patient chart, and in cases where a mismatch between the survey response and the patient chart data were observed, information from the patient file was used.
Data were registered in REDCap and exported to Microsoft Excel (Version 1808) and SPSS (Version 22.0.0.0), where statistical analyses were performed, and data were presented using descriptive statistics or as means with standard deviations (SD).
Patient characteristics
A total of 132 patients with a diagnosis of PN were identified. Of these patients, 39 were excluded as they had either died, moved abroad, or were misdiagnosed. The survey was distributed to 92 eligible patients (mean ± SD age 64.4 ± 14.5 years), where 58 (62.4%) were women.
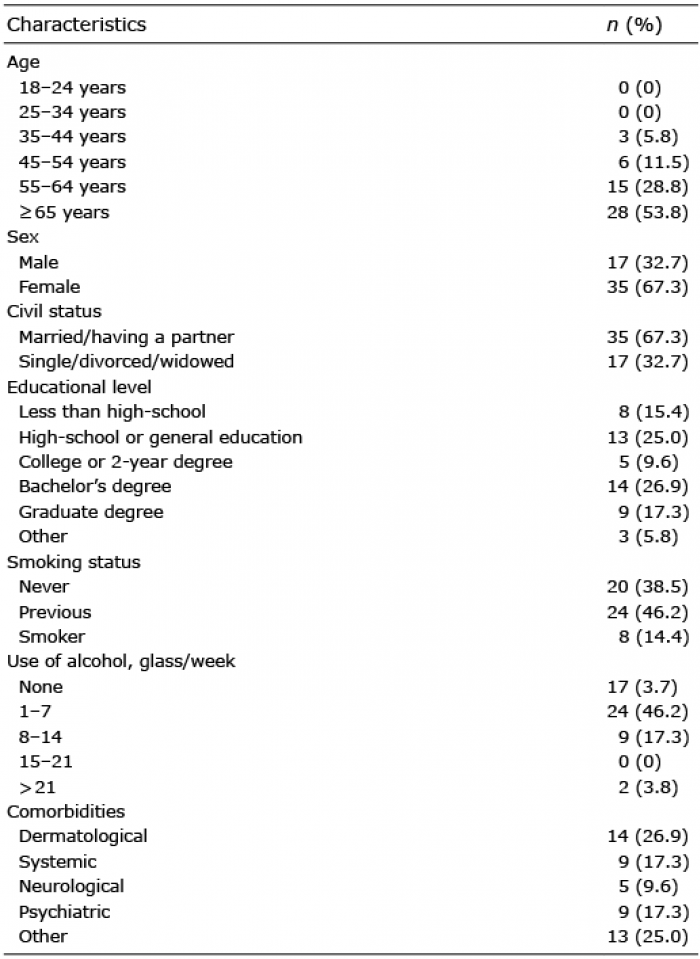
A response was received from 52 (55.9%) patients (mean ± SD age 64.4 ± 11.0 years), of whom 35 (67.3%) were women and 28 (53.8%) were ≥ 65 years of age. No significant difference in age or sex was found between responders and non-responders. All patients with PN had been diagnosed by a dermatologist. Patients’ sociodemographic characteristics are shown in Table I.
Mean ± SD duration of PN was 11.6 ± 8.2 years. Twenty-six (50.0%), patients had > 20 nodules and only 10 (19.2%) had < 6 nodules. The most frequently reported localization of PN were legs/feet (92.2%) and arms/hands (78.4%), followed by back (47.1%), buttocks/genitals (37.3%), chest (35.3%) and head/neck (19.6%).
More than a quarter (26.9%) of the patients had a concomitant dermatological disease; 8 (15.4%) had atopic dermatitis, which was the most commonly reported dermatological disease.
Regarding other diseases, 23 (44.2%) patients reported having at least 1 concomitant non-dermatological disease; and 9 (17.3%) had a psychiatric disease, which was the most commonly reported non-dermatological disease (Table I).
Table I. Patients’ sociodemographic characteristics and comorbidities (n = 52)
Treatment characteristics
For local treatments, all 52 patients had been treated with at least one type of topical treatment. The most commonly used were topical corticosteroids. A total of 49 patients (94.2%) had been treated with topical corticosteroids; of these 13 (26.5%) reported a positive effect on pruritus. A total of 40 patients (76.9%) had been treated with topical corticosteroids under occlusion; of these 21 (52.5%) reported a positive effect on pruritus. A total of 37 patients (71.2%) had been treated with zinc dressing treatment; of these 17 (45.9%) reported a positive effect on pruritus. A total of 14 patients (26.9%) had been treated with intradermal injection of corticosteroid; of these 9 (64.3%) reported a positive effect on pruritus.
For phototherapy, 46 patients (88.4%) had been treated with UVB (3 weekly irradiations of narrowband-UVB for 8–12 weeks is standard at the department); of these 9 (19.6%) reported a positive effect on pruritus.
Only 24 patients (46.2%) had been treated with at least one type of systemic treatment. The most frequently used systemic treatment was methotrexate (15–20 mg weekly). In total, 16 patients (30.8%) had been treated with methotrexate; of these 5 (31.3%) reported a positive effect on pruritus. A total of 12 patients (23.1%) had been treated with thalidomide (25–50 mg daily); of these 4 (33.0%) reported a positive effect on pruritus; however, thalidomide was associated with several side-effects (Fig. 1).
Fig. 1. Prescribed therapies and patient-assessed evaluation of treatment in a cohort of patients with prurigo nodularis. The y-axis represents number of treated patients. The x-axis represents various treatments. Colour-bars represent evaluation of treatment. Patients reporting treatment effect as: “positive” blue; “discrete effect” orange; “negative effect” grey; “no effect” yellow.
Pruritus characteristics and impact on quality of life
The patients experienced moderate to severe pruritus on the VAS scale (mean ± SD VAS 6.6 ± 2.4). In a majority of patients, pruritus occurred at least several times a day (65.4%), with the evening (66.7%) and night (41.1%) being reported as the most intense hours of pruritus. Pruritus characteristics are shown in Table II.
Thirty-nine (75.0%) responded that pruritus had a negative effect on their QoL, mean ± SD DLQI was 7.0 ± 5.6, indicating an overall moderate effect on QoL. Fourteen patients (26.9%) did not participate in social activities and were more absent from work compared with colleagues, or had to retire from work due to their disease. For sleep-quality, 10 patients (19.2%) used sleep medication at least once a month and mean ± SD PSQI was 6.2 ± 2.0, indicating poor sleep.
Table II. Pruritus characteristics in patients with prurigo nodularis; localization of pruritus, day- and night-time course of pruritus (*multiple answers possible), frequency of pruritus and quality of pruritus (*multiple answers possible)
Main findings and interpretation
This study found that the majority of patients with PN were elderly (53.8% were ≥ 65 years of age) and female (67.3%). In more than half of the patients (57.7%) we identified at least one underlying condition; however, patients had a wide range of conditions, with the most commonly reported being atopic dermatitis and psychiatric conditions. This study found that various treatments are prescribed to patients with PN, but, overall, the effectiveness of treatments is poor. Corticosteroids under occlusion, zinc dressing treatment, steroid injections, methotrexate and thalidomide were reported as the most effective treatments; however, results of steroid injections, methotrexate and thalidomide should be considered with caution, as the number of patients treated was small. In general, patients with PN are negatively affected by their disease, mainly due to severe pruritus.
In an EADV Task Force Pruritus survey, 73% of members considered PN to be a distinct condition (8). When looking at underlying conditions, the current study found that 58% of patients had at least one underlying condition, with the most common, at 15%, being atopic dermatitis. Likewise, Iking et al. (9) found a similar prevalence of atopic dermatitis in a cohort of 108 patients with PN (18% vs. 15%), which has also been described elsewhere (4). In the study by Iking et al., 87% of patients had an underlying condition; however, these data were extracted from a database and not entirely self-reported, which may explain the difference from our findings. Also, in a recent study by Boozalis et al. (4), it was found that PN was associated with numerous systemic conditions, such as HIV, chronic kidney diseases and diabetes. We were not able to recognize these findings in our study, which could be explained by ethnic differences, as our patient group was primarily Caucasian.
In the literature it has been discussed whether psychiatric conditions are more common in patients with PN and whether psychological distress could lead to picking of the skin, thereby inducing PN (1). It was found that 17% of patients had a psychiatric condition; of these 10% had depression. Similarly, in 2018, Jørgensen et al. (3) found, in a cohort of 877 patients with PN, 8.5% had depression, thus PN seems more often to be associated with having a psychiatric condition compared with the background population (10, 11).
It is well established that scratching behaviour may play a role in triggering the itch-scratch cycle (1, 3, 12). This emphasizes the importance of optimizing treatment for patients with pruritic diseases, such as atopic dermatitis, to stop patients commencing continuous scratching. Indeed, breaking the itch-scratch cycle may be an important treatment goal for patients with PN. In support of this, we found positive reporting in a large proportion of patients (46.9–52.5%), who had used corticosteroids under occlusion or zinc dressing treatment; ideally these should be considered as a first-line treatment.
Interestingly, this study found that the most commonly used treatments were topical corticosteroids and UVB; however, only a minor group of the patients reported these to have a positive effect (26.5% and 19.6%). This indicates that topical corticosteroids under occlusion should be tried first. In patients presenting only a few nodules intradermal injection of steroid may be beneficial, as a majority of treated patients (64.3%) reported this to have a positive effect.
In the literature immunosuppressants and gabapentin have been described as effective systemic therapies for pruritus (13, 14). This was also found in the EADV Task Force Pruritus survey, in which 27% and 17% of physicians reported immunosuppressants and gabapentin as the most effective therapies (8).
In the current study, only 6 patients had been treated with gabapentin (11.5%), thus the number is too small to evaluate the effect of these. Nearly one-third of patients (31.3%) considered methotrexate to have a positive effect, indicating that methotrexate should be considered at an early stage of the disease. In line with this, a recent review concluded that methotrexate was able to significantly reduce pruritus in patients with PN (15). Although a large proportion of patients (33.0%) treated with thalidomide reported this to have a positive effect, it should be prescribed with caution. In a study by Andersen & Fogh (16), thalidomide reduced pruritus in 32 of 42 (76.2%) treated patients with PN, but in 25 patients (59.5%) peripheral neuropathy was observed. Furthermore, thalidomide has a poor safety profile and is associated with several severe conditions, such as thromboembolisms, bone-marrow suppression and teratogenicity (16, 17).
As reported in other studies (3), patients with PN were found to carry a great burden of disease with a negative impact on everyday life, social activities and sleep, which highlights the importance of offering these patients the most effective on-hand treatment. Although we found that corticosteroids under occlusion and zinc dressing treatment could decrease pruritus, there is still a need for new treatments, as many patients are not sufficiently treated with the existing treatments. A clinical trial exploring the use of neurokinin-1-receptor antagonist has recently shown that it has an effect and a few case reports of patients with PN treated with dupilumab have shown promising results (18–20). Furthermore, nalbuphine (NCT02174432) and nemolizumab (NCT03181503) have been shown to be able to reduce pruritus in other dermatosis (21, 22), and both are currently being investigated as potential treatments for PN.
Strengths and limitations
This patient-based survey includes both the treatment patterns, the effectiveness of existing treatments and the continuous needs from the patient’s perspective. This study was established, containing detailed questions on therapies used, pruritus characteristics, comorbidities, and QoL, in order to retrieve a better understanding of PN, which has been warranted by the EADV Task Force Pruritus (8). It is hoped that this can guide physicians to improve the management of PN with the existing treat-ments. Secondly, all patient charts were investigated by a physician to ensure that only patients with correct diagnosis were included. Also, patient answers on treat-ment were validated. Thirdly, we identified, although the sample size was small, 92 patients with PN. However, the response rate was nearly 60%, which should be considered as a satisfactory result, as this is a vulnerable and elderly group of patients.
Limitations of this study are; a large part of the information is based on surveys, which is likely to induce recall bias. Although we found no difference in age and sex between groups of responders and non-responders, surveys often increase risk of selection bias, as patients with severe disease may be more prone to respond. Moreover, this was a descriptive study with no control group. An improvement would be to compare the patient group with patients who have other dermatological diseases, as has been done by Steinke et al., where patients with PN were found to have a decreased QoL compared with other pruritic dermatological diseases (23).
Conclusion
This study found that patients are severely affected by PN, especially due to severe pruritus. Many patients are treated with numerous treatments, including topical-, photo- and systemic therapy; however, for a large group of patients the existing treatments are not able to reduce pruritus. Patients considered the most effective treatments to be corticosteroids under occlusion and zinc dressing treatment, steroid injection, methotrexate and thalidomide.
In conclusion, these results emphasize the need for new therapies to improve the management of PN.
This study was supported by Aage Bangs Foundation.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize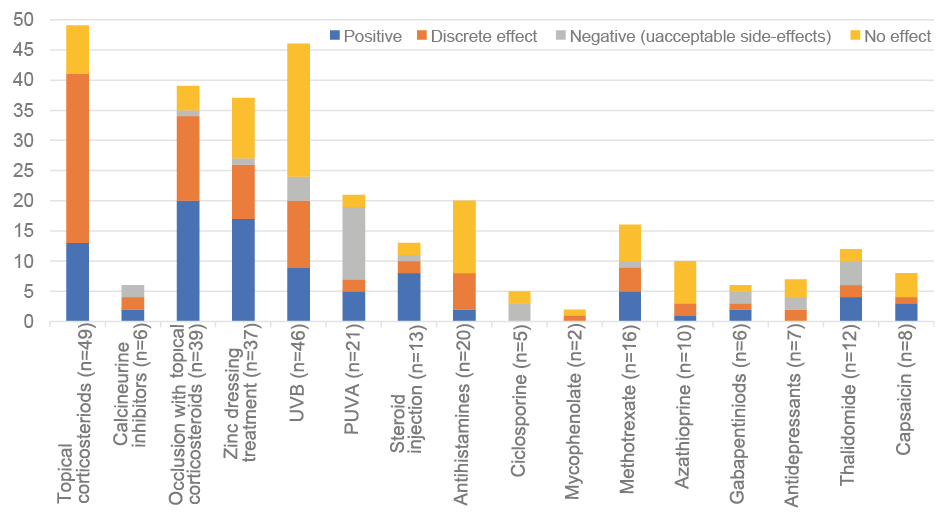 Click to show fullsize
Click to show fullsize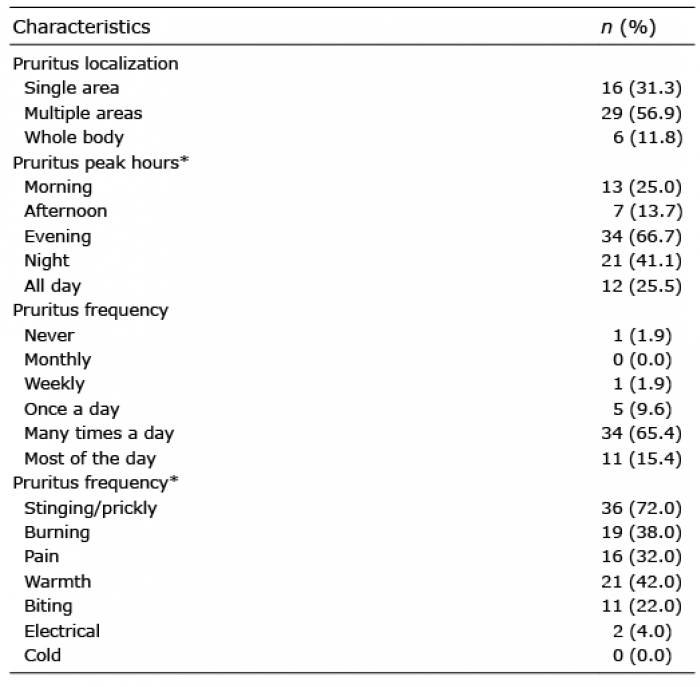 Click to show fullsize
Click to show fullsize