


1Division of Dermatology, Nagaoka Red Cross Hospital, and 2Division of Dermatology, Niigata University Graduate School of Medical and Dental Sciences, 1-757 Asahimachi-dori, Chuo-ku, Niigata 951-8510, Japan. *E-mail: rh19840629@med.niigata-u.ac.jp
Accepted Mar 24, 2020; Epub ahead of print Mar 26, 2020
Acta Derm Venereol 2020; 100: adv00108
Systemic corticosteroids are the main treatment for bullous pemphigoid (BP). CYP3A4 hepatic enzymes play an important role in steroid catabolism and in the metabolism of foreign compounds, with the majority of pharmaceutical compounds being substrates for CYP3A4 (1). Several antiepileptic drugs, such as phenytoin and carbamazepine, strongly induce CYP3A4 and attenuate the effects of steroids (2). We report here a case of refractory bullous pemphigoid that improved after discontinuation of phenytoin.
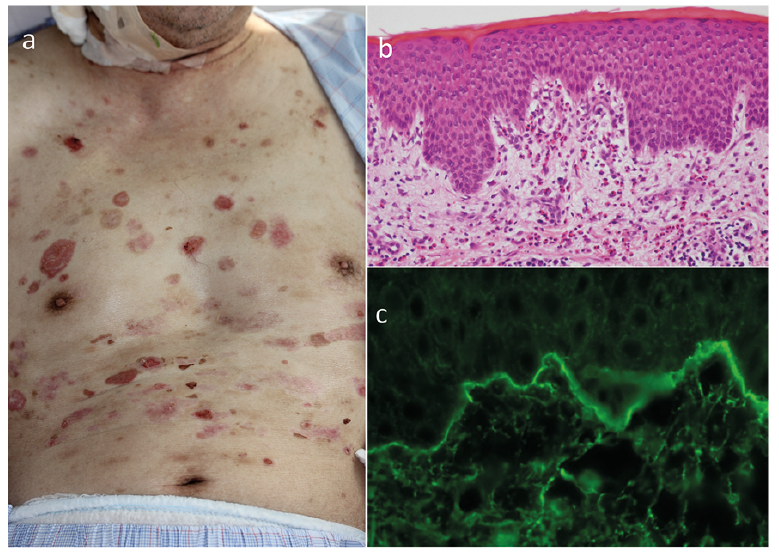
A 72-year-old man presented with a 7-month history of pruritus and generalized annular edematous erythema with blisters. He had a history of infantile cerebral palsy and epilepsy, and was treated with phenytoin, sodium valproate, and primidone. Based on the physical and histopathological findings, BP was diagnosed and treatment with 50 mg/day prednisolone (PSL) was started. Because his skin eruptions worsened despite the initial treatment, he was referred to our hospital. On his first visit, we found reddish or brownish erythema and numerous tense bullae on his entire body (Fig. 1a). His oral cavity and genital area were unaffected. Laboratory examinations showed a high titre of anti-BP180 antibodies, over 1,000, and eosinophilia of 17.6%. Histopathological findings of erythema on the trunk showed liquefaction degeneration with eosinophil infiltration (Fig. 1b). Direct immunofluorescence revealed linear deposition of IgG and complement C3 in the basement membrane zone (Fig. 1c). Treatment was started with intravenous methylprednisolone half pulse therapy, dose 500 mg/day for 3 days, and an oral daily dose, 1 mg/kg (50 mg), corticosteroid.
Fig. 1. Clinical and histological features. (a) Physical examination findings showing a number of dark-reddish erosions and tense bullae disseminated over the patient’s entire body. (b) Histopathology of biopsy showing a subepidermal blister and moderate infiltration of eosinophils in the dermis (original magnification ×10). (c) Direct immunofluorescence showing linear deposition of IgG and complement C3 in the basement membrane zone.
However, new bullae and erythema still developed, and intravenous immunoglobulin (IVIG) therapy was added, 400 mg/kg/day for 5 days, and double filtration plasmapheresis (DFPP). Despite these treatments, the disease activity could not be controlled. Moreover, steroid rotation from prednisolone to betamethasone was not effective. Finally, drug-related BP was suspected because phenytoin has been reported to strongly induce CYP3A4 and attenuate the effect of steroids. After treatment was switched from phenytoin and sodium valproate to levetiracetam, the patient’s skin symptoms improved rapidly and the titre of anti-BP180-NC16A antibodies improved (Fig. 2).
Fig. 2. Clinical course of the case. Although the patient was treated with intravenous half-dose of methylprednisolone (mPSL) pulse therapy, dose 500 mg/day for 3 days, an oral daily dose of 1 mg/kg (50 mg) corticosteroid (prednisolone; PSL), intravenous immunoglobulin (IVIG) and double filtration plasmapheresis (DFPP), the disease activity could not be controlled. However, skin symptoms and the titre of anti-BP180-NC16A antibodies improved after changing phenytoin and sodium valproate to levetiracetam. Moreover, the eruption had not yet appeared at this point. After changing the anticonvulsant, we could reduce the steroid dose, no new eruption appeared, and the titre of anti-BP180-NC16A antibodies decreased gradually.
With regard to the interaction between steroids and several drugs, CYP3A4, which is a drug-metabolizing enzyme in the liver, is strongly induced to enhance steroid metabolism, resulting in diminished pharmacological action (3). The main metabolic pathways of steroids include A-ring reduction and 6β hydroxylation, and the enzyme that catalyses 6β hydroxylation is CYP3A4 (4).
Because cortisol mainly undergoes A-ring reduction and 20-position reduction in most metabolic pathways, even when used in combination with drugs that induce CYP3A4, the effect is less attenuated and 80% of the effect remains (5).
Because dexamethasone and betamethasone are the main metabolic pathways for 6-hydroxylation, only 20% remains effective. Prednisolone is half-dihydrated at the 6-position and half-reduced at the 20-position, and its effect is reduced by half (6).
CYP3A4-inducing drugs include anti-epileptic drugs (e.g. phenytoin) and anti-tuberculosis drugs (e.g. rifampicin). In the dermatology field, CYP3A4-inducing drugs are, for example, vemurafenib and dabrafenib used for malignant melanoma, bexarotene used for mycosis fungoides, amenamevir used for herpes zoster, and bosentan hydrate used for skin ulcers of systemic scleroderma.
If the effects of steroids are thought to be diminished due to CYP3A4-inducing drugs, a discontinuation of the causative drug should be considered. A previous report has shown that 2-fold higher doses of CYP3A4-metabolized drugs may generally be required during concurrent treatment with phenytoin or carbamazepine (2). If it is difficult to change the drug, as in cases of antiepileptic or anti-tuberculous drugs, an increase in the corticosteroid dose is recommended. High-dose and long-term corticosteroid admission may be associated with side-effects; therefore, it is better to select drugs that exert lesser effects, such as azathioprine, when using CYP3A4-inducing drugs. Cyclosporin is also a CYP3A4-metabolized drug, and it has been reported that the blood concentration of cyclosporin decreased by approximately 50% using bosentan (7). Diaminodiphenyl sulfone is reportedly less effective with rifampicin; however, it is mainly metabolized by CYP2E1, and caution should be exercised when using such drugs.
In case of refractory diseases treated using corticosteroids, it should be considered whether the drug chosen for treatment induces CYP3A4.


 Click to show fullsize
Click to show fullsize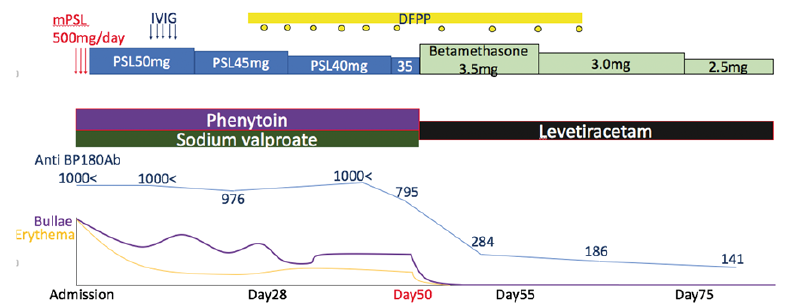 Click to show fullsize
Click to show fullsize